


The ASCO 2026 Annual Meeting in Chicago has officially come to an end, leaving the oncology community with a massive wave of new data, practice-changing updates, and a clearer plan for patient care worldwide. From the remarkable survival results shared during the Sunday Plenary sessions to critical discussions on safely reducing treatment intensity, this year’s meeting showed that cancer care is advancing rapidly.
Beyond the major clinical trials, the true energy of the week came from the people on the floor. The meeting highlighted strong global collaboration, celebrated the achievements of rising young researchers, and focused heavily on making life-saving treatments accessible to patients everywhere.
As clinicians and researchers head home to process these updates and apply them to daily practice, here is a comprehensive look back at the main trials, major tumor tracks, and standout moments that defined this important week.
The conference officially opened with a powerful Presidential Address by ASCO President Eric Small. Focusing on his core theme, ‘The Science and Practice of Translation: Improving Cancer Outcomes Worldwide,’ Dr. Small emphasized the urgent need to break down barriers and make sure clinical laboratory breakthroughs actually reach patients in real-world communities globally. It was the perfect framing for a week defined by data meant to change standard practice immediately.

Following this global call to action, the meeting dove straight into the heavy-hitting data. Here are the main clinical highlights and major trial updates that dominated the floor across each tumor track.
Breast Cancer
Sarah Sammons
“Big week for breast cancer at ASCO26. A few highlights from the meeting!”
“Metastatic
TROPION-Breast02 + ASCENT-03 (TNBC, PD-L1 ineligible): Two practice-changing Trop2 ADC options for 1L. Subsequent analyses confirm benefit. 2 good options.
VIKTORIA-1 (HR+/HER2-, PIK3CA-mutated, 2L post-CDK4/6i):
Gedatolisib + fulvestrant beat alpelisib with a much cleaner toxicity profile. Triplet did not add anything with palbociclib. Less hyperglycemia, less diarrhea. Stomatitis remains a challenge. Will be a nice doublet option if approved. IV drug.
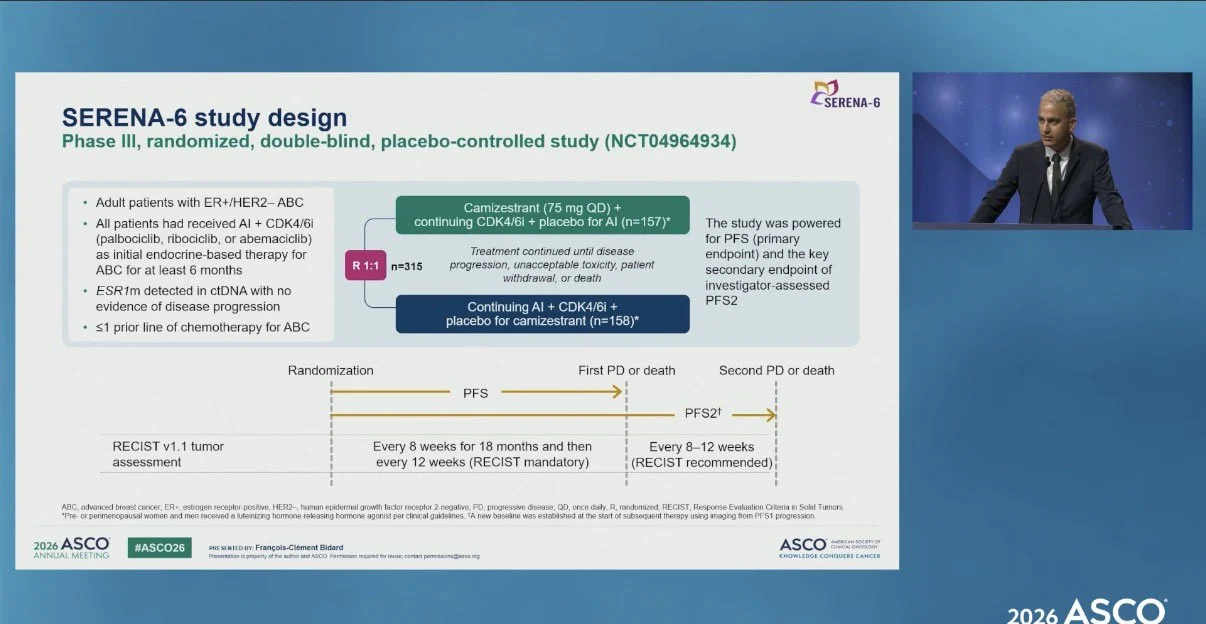
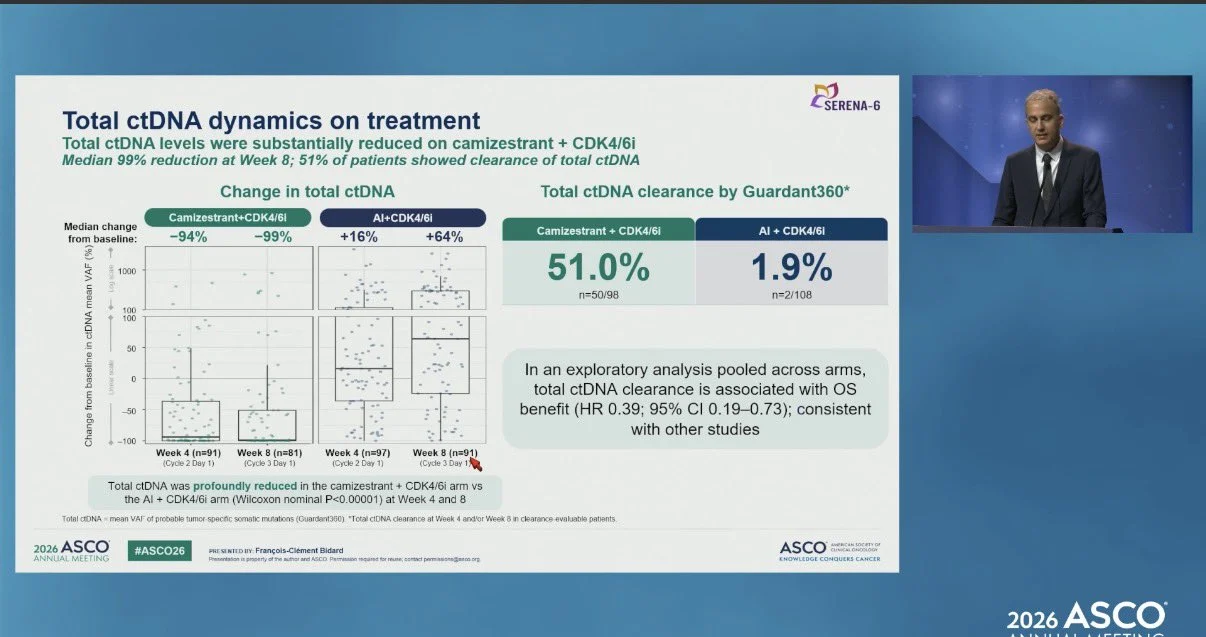
SERENA-6 (HR+/HER2-):
Switching to camizestrant when ESR1 mutation is detected on ctDNA, before progression, yielded 51% ctDNA clearance vs 1.9%. Compelling biology. Let’s see what the FDA does.
persevERA (HR+/HER2-, 1L):
Giredestrant + palbociclib did not beat letrozole + palbociclib (33.1 vs 28.2 mo, p=0.15). The 1L SERD moment has not arrived yet. Metastatic SERD benefit appears limited to ESR1-mutant disease.
Early Stage
lidERA (HR+/HER2-): First new adjuvant endocrine therapy in decades. Giredestrant cuts recurrence risk about 30% across pre and postmenopausal patients in subgroup analyses. Premenopausal patients need OFS. FDA submission underway.
KEYNOTE-522 at 7 years (TNBC, stage II-III):
EFS 78.3% vs 69.8%, OS 85.1% vs 77.2%. The benefit is durable and real. But real-world irAE rates up to 54%. We need a biomarker to identify who can safely skip immunotherapy.
OPTIMA (HR+/HER2-, node-positive):
Chemo omission non-inferior in low genomic risk node-positive patients including N2 using Prosigna. Practice changing for postmenopausal patients. For premenopausal, the key insight is that chemo benefit in low genomic risk patients is largely driven by ovarian suppression, not cytotoxicity. Still need more premenopausal N2 data. Enroll to OFSET.
OASIS-4 (HR+, on ET):
Elizanetant improves hot flashes AND sleep across tamoxifen, AI, and GnRH agonist therapy. Non-hormonal and safe for HR+ patients. An adherence tool we have really needed.
REDUSE (bone mets):
Denosumab every 12 weeks after induction is non-inferior to every 4 weeks for skeletal-related events, with less hypocalcemia, less ONJ, and more than 50% reduction in drug costs. Smarter de-escalation with no efficacy tradeoff.
GLP-1 RAs: Real-world data showing 43% reduction in metastatic progression and 30% mortality reduction in HR+/HER2- patients on ET + CDK4/6i. Still observational, but the tumor GLP-1 receptor expression data suggests this is more than just a metabolic effect. Prospective studies needed.
Grateful for the science.”
Elisa Agostinetto
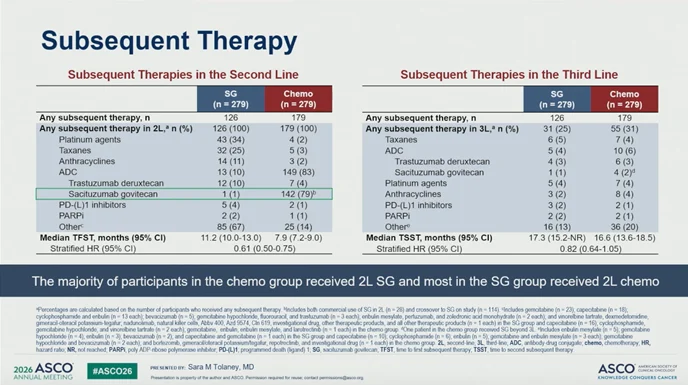
“At ASCO26 metastatic breast cancer session, Sara Tolaney presents results on the PFS2 from the ASCENT-03 trial.
PFS2 was longer in the SG arm vs CT arm, despite high rate of tx crossover, with most pts in the CT arm receiving SG after progression (79% in 2L, 82% any L).”

Naoto T Ueno
“Both ASCENT-04 and ASCENT-03 efficacy is biomarker independent. Is this surprising? Not really. We have seen a similar pattern across the DESTINY-Breast studies, where no biomarker has been statistically meaningful enough to clearly define who benefits.
This may be a fundamental feature of ADC biology. ADCs are not classic targeted therapies in the narrow sense. They use the antibody to deliver a potent payload, and once enough drug reaches the tumor, the payload can effectively annihilate cancer cells.
That is why expression level, BRCA mutation status, or HER2-low versus HER2-ultralow may not always behave as clean predictive biomarkers.”
You can also read:
ASCENT-03 Shows SG Benefit Across TNBC Biomarker Subgroups

Kazuki Nozawa
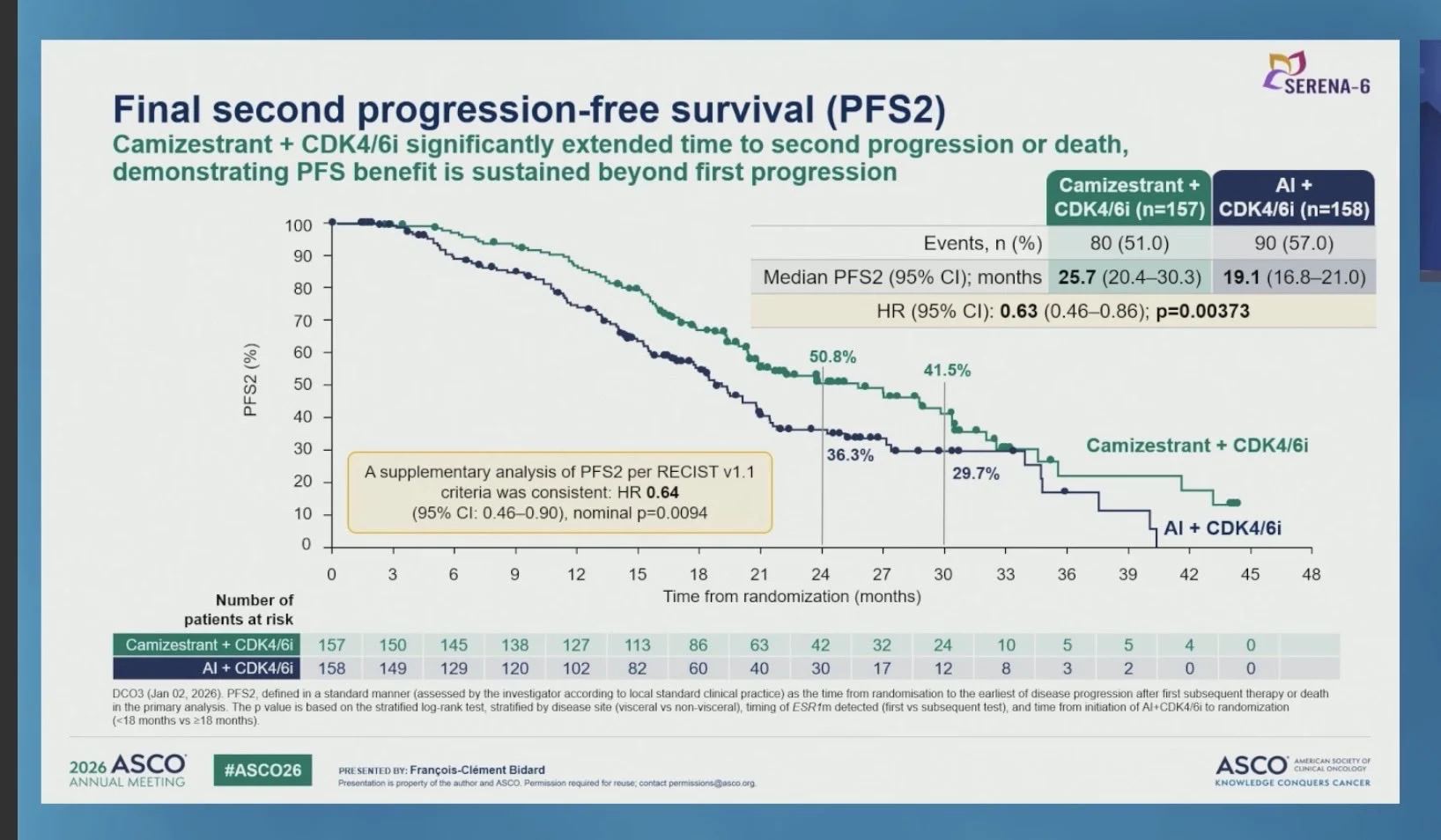
“SERENA-6 Trial – Final PFS2 Analysis
Switching to camizestrant + CDK4/6i at the emergence of ESR1 mutations in ER+/HER2− advanced breast cancer.
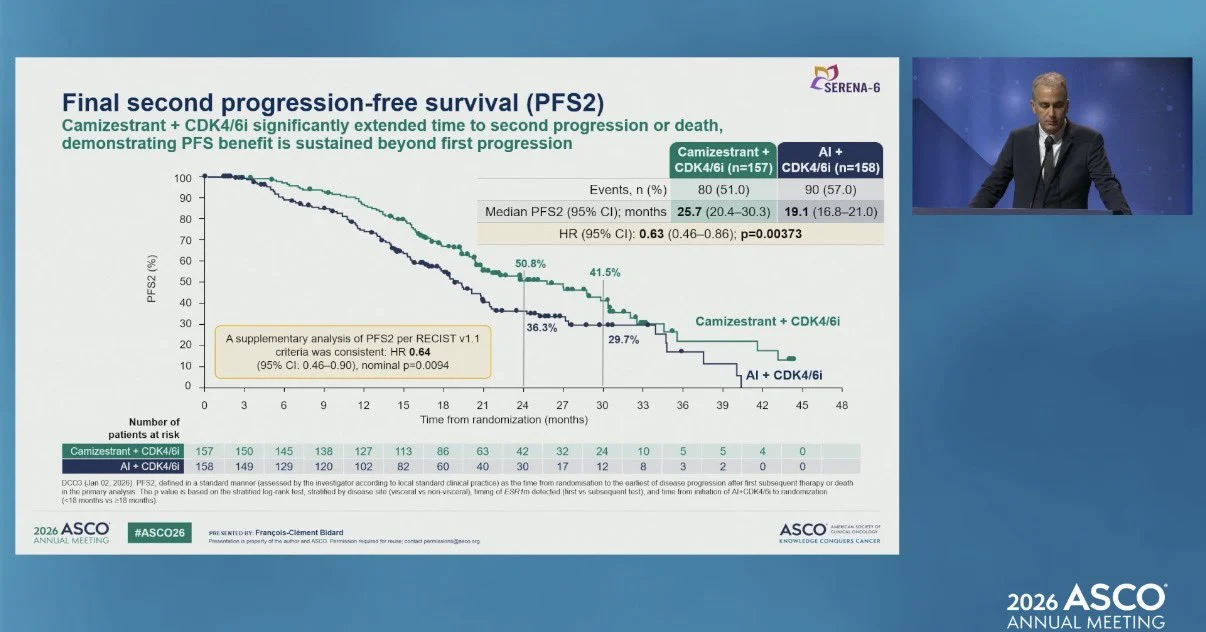
Updated PFS: median 7.6-month improvement – HR 0.45, with 1 in 3 patients still progression-free at 24 months.
PFS2 (final): 25.7 mo vs 19.1 mo – HR 0.63 (p=0.00373), confirming the benefit extends well beyond first progression.
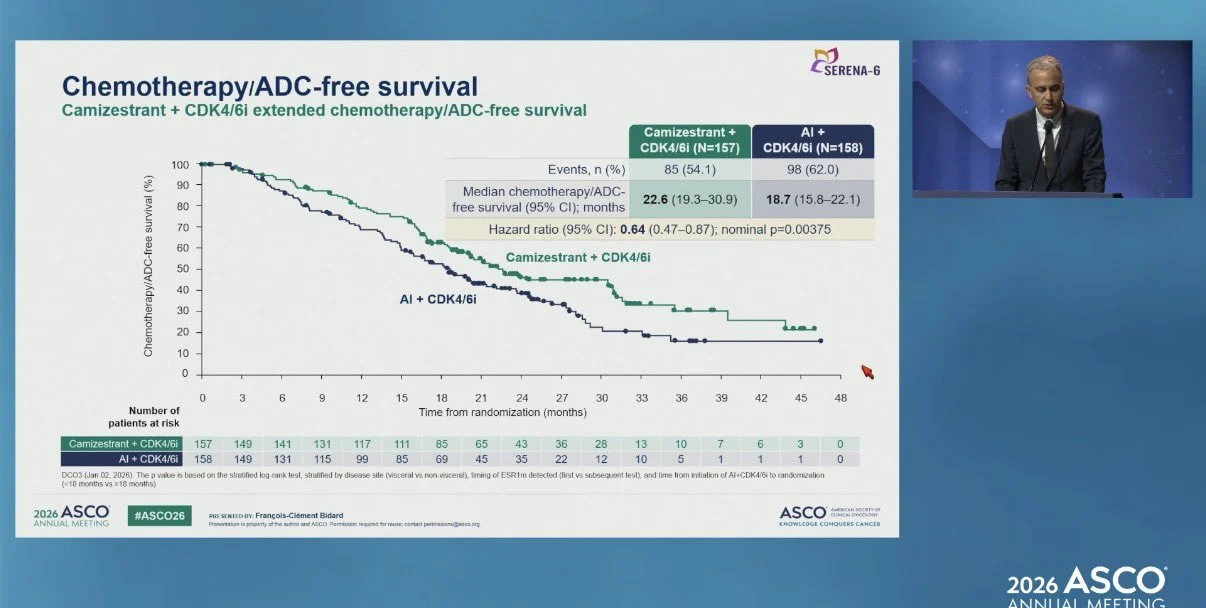
Additional findings:
- Chemotherapy/ADC-free survival: 22.6 mo vs 18.7 mo – HR 0.64
- OS HR: 0.87, continuing to mature in favor of camizestrant.”

Tuğba Başoğlu
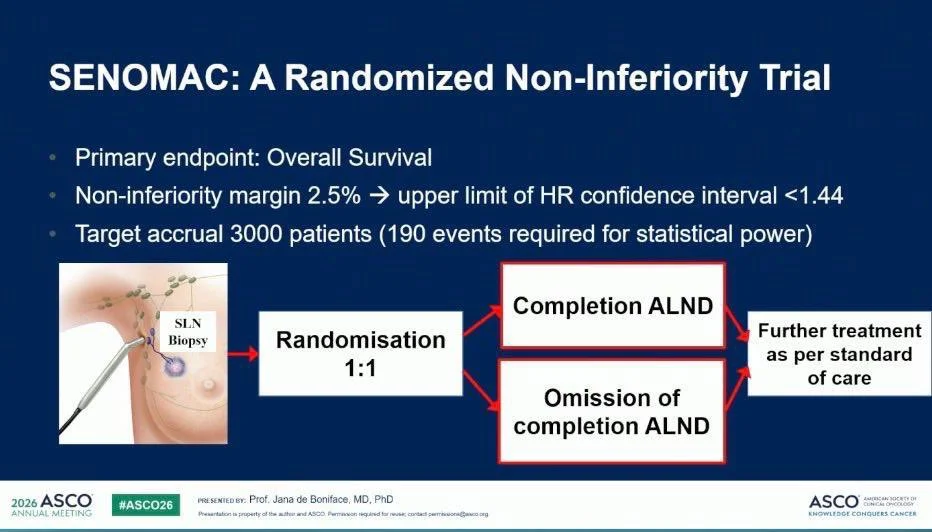
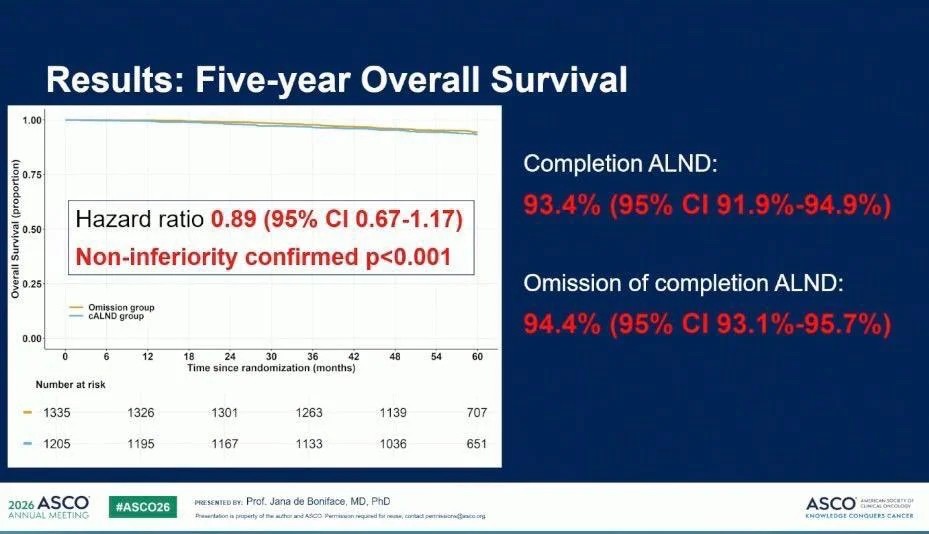
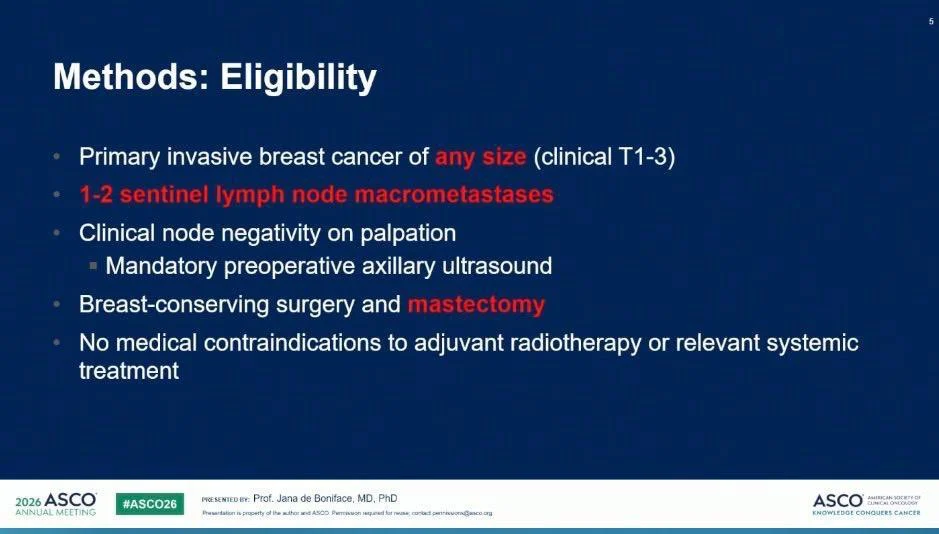
“SENOMAC confirms that less can be more in axillary surgery.
- 5-year OS: 94.4% vs 93.4%
- Omission of completion ALND was non-inferior to ALND
- Significantly better quality of life and arm function
- Fewer arm-related symptoms
For patients with 1–2 positive sentinel lymph nodes, routine completion ALND may no longer be necessary.
Same survival. Less morbidity. A new standard of care.”

Read further on the SENOMAC trial:
SENOMAC: Omitting Completion Axillary Dissection Maintains Survival and Reduces Arm Morbidity in Breast Cancer

Yara Abdou
“How helpful is PFS2 without crossover?
In SERENA-6, none of the control arm patients received camizestrant on progression and only a small minority received another oral SERD. ”

Yakup Ergün
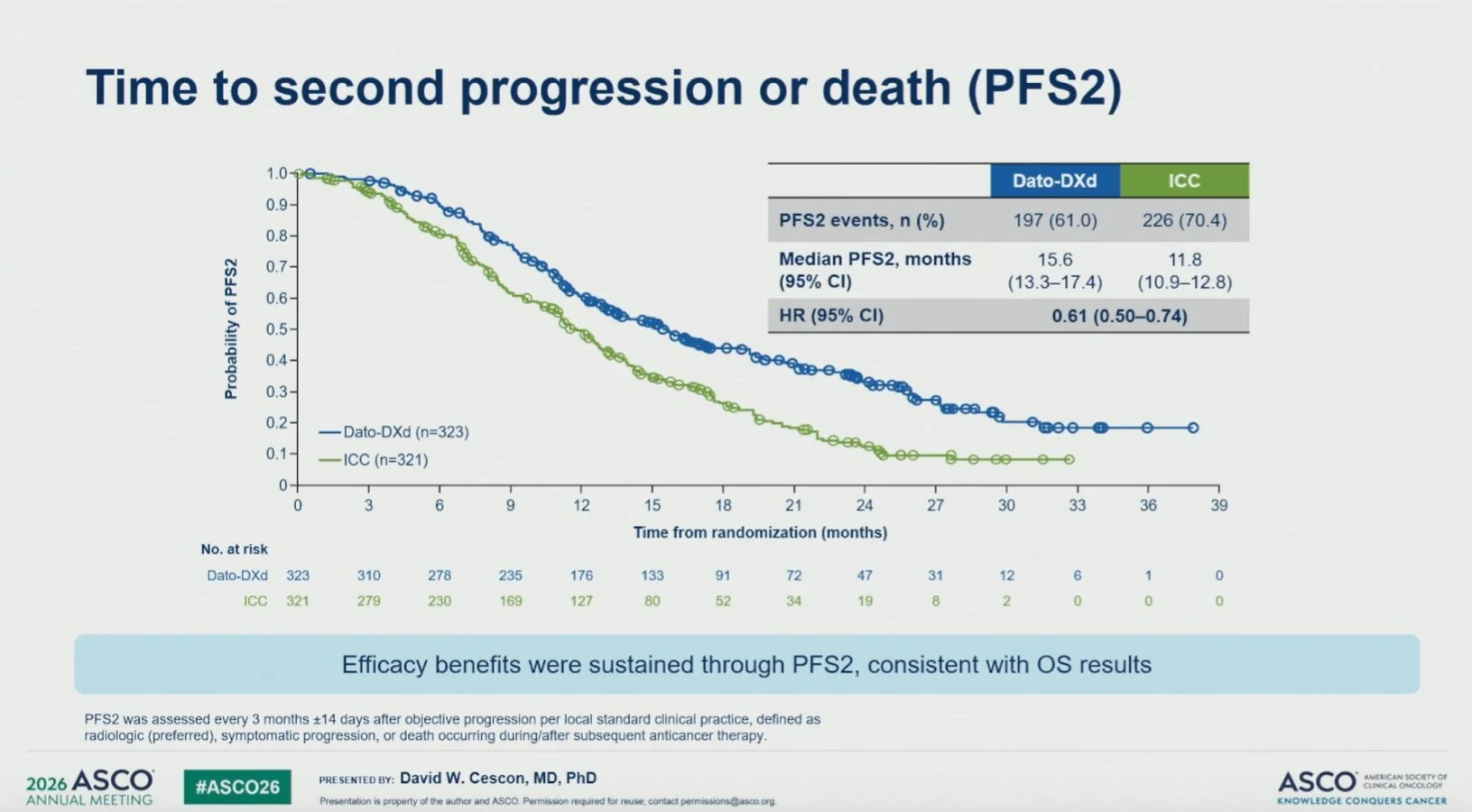
“TROPION-Breast02 PFS2
Like ASCENT-03/04, TROPION-Breast02 showed a PFS2 benefit with an ADC in 1L mTNBC:
PFS2: 15.6 vs 11.8 months HR 0.61
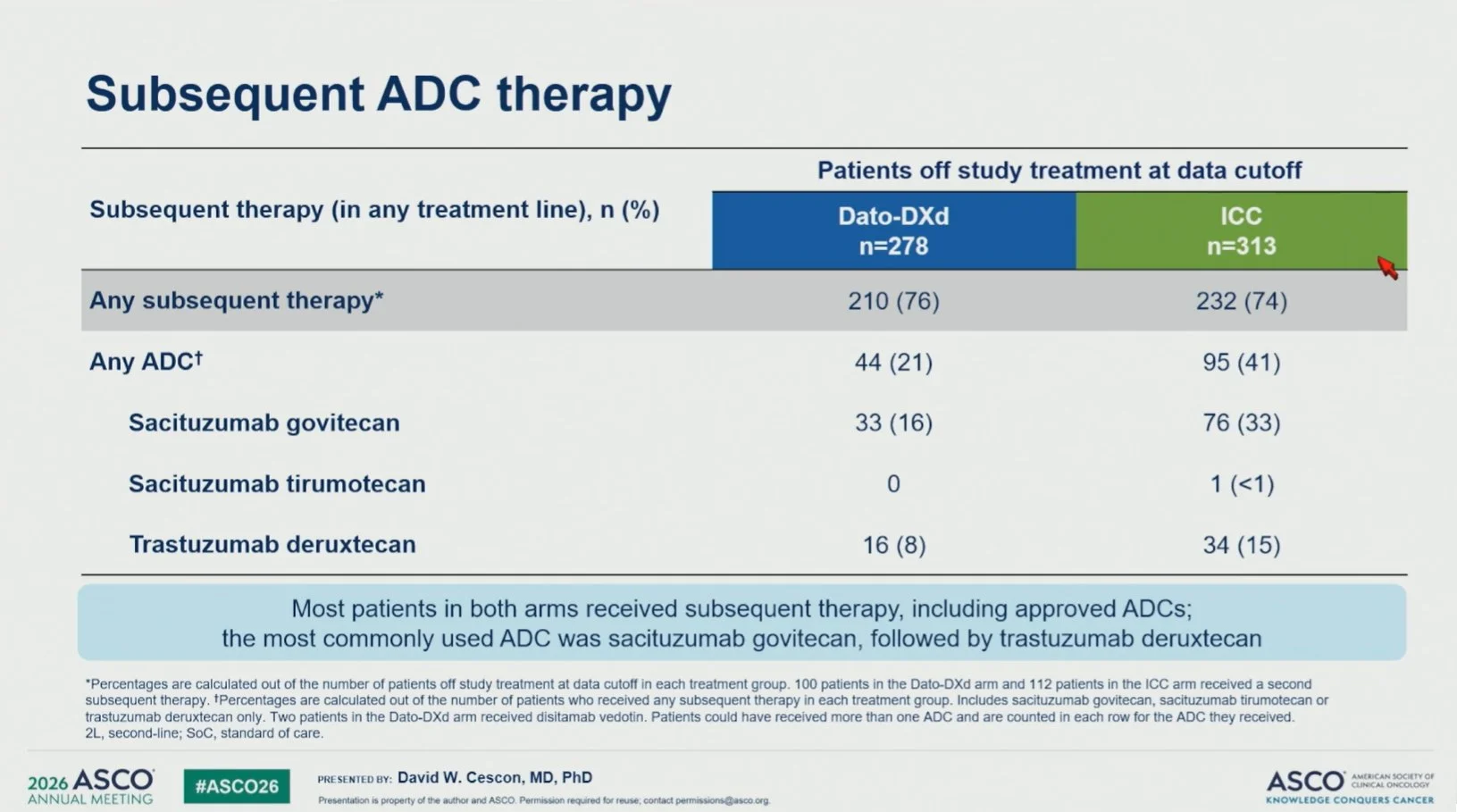
However, unlike the ASCENT studies, crossover was not allowed. Subsequent ADC use was reported in 41%, but the proportion receiving it specifically in 2L was not clear (I couldn’t see it.)
That said, Dato-DXd had already shown better ORR and a significant OS benefit!”

Lung Cancer
Estela Rodriguez
“The sexiest survival curve at ASCO26 by far.”
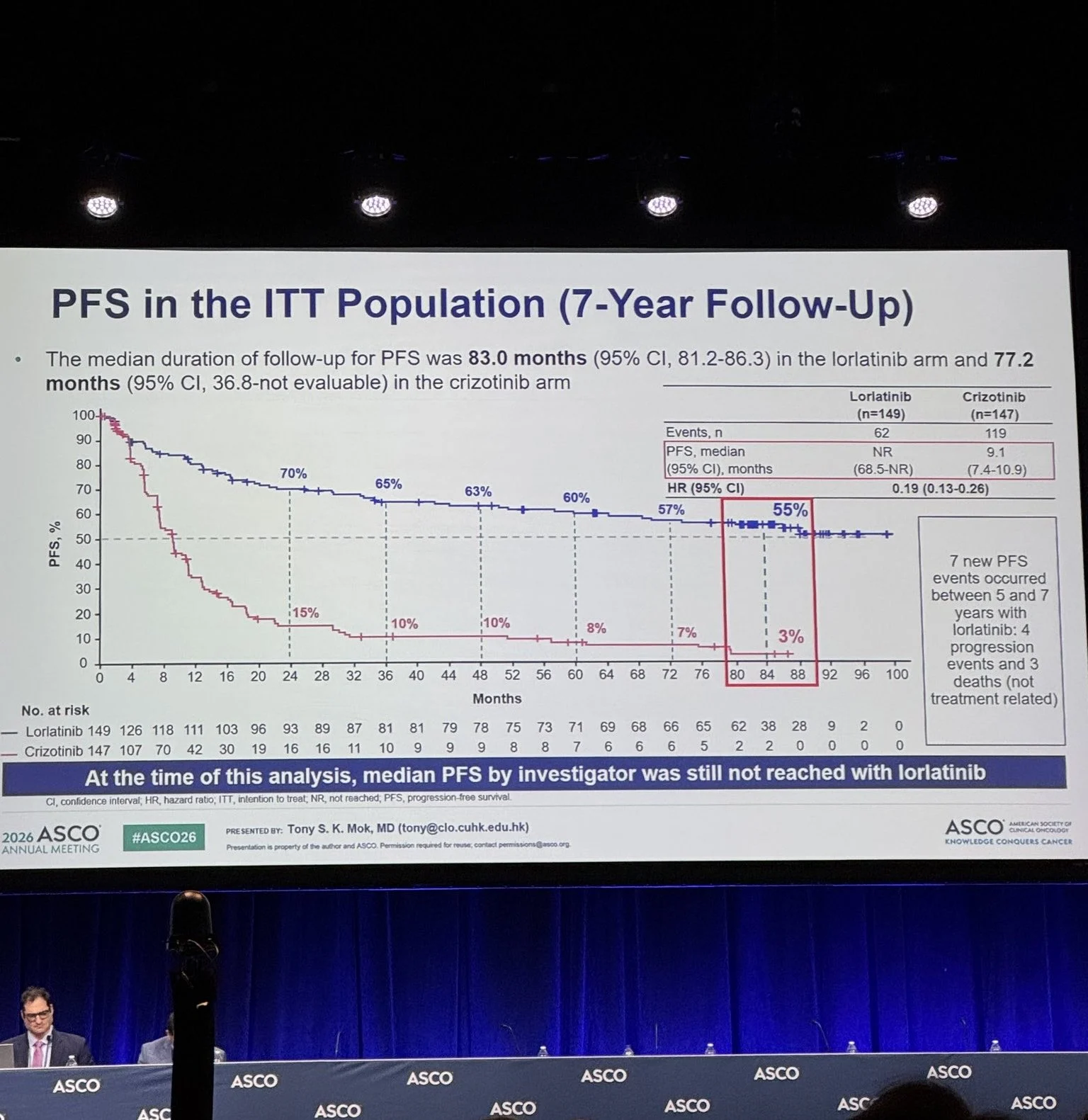
“Updated 7-year PFS from the ITT population of lorlatinib in the CROWN trial for ALK+ lung cancer, presented by Tony Mok.
Longest duration of response yet seen with targeted therapy in lung cancer: median PFS still not reached at 7 years. 55% vs 3% for crizotinib (HR 0.19).
Looking forward to see what the next generation of ALK inhibitors will bring in terms of efficacy and improved toxicity profile.”

Alfredo Addeo
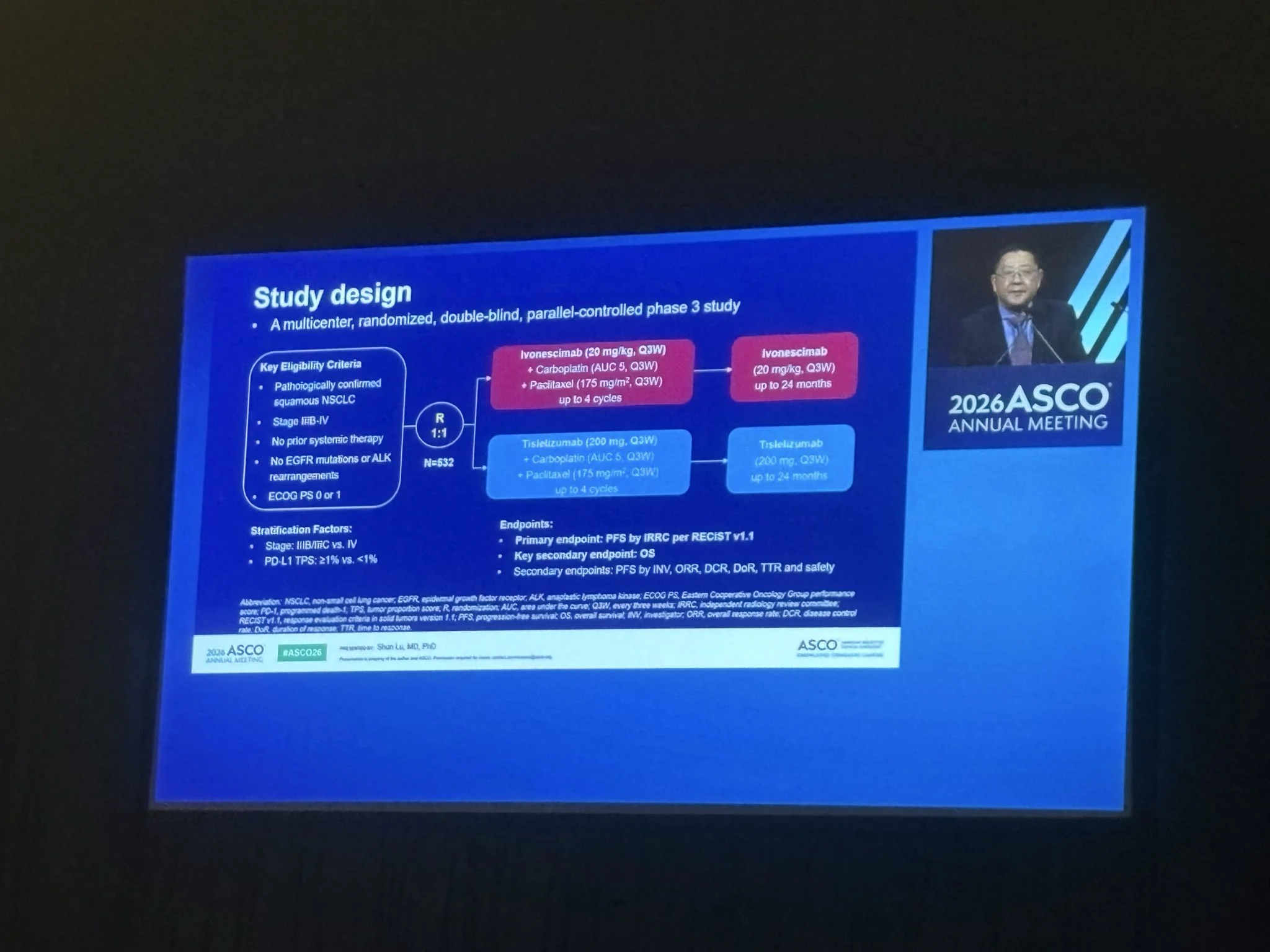
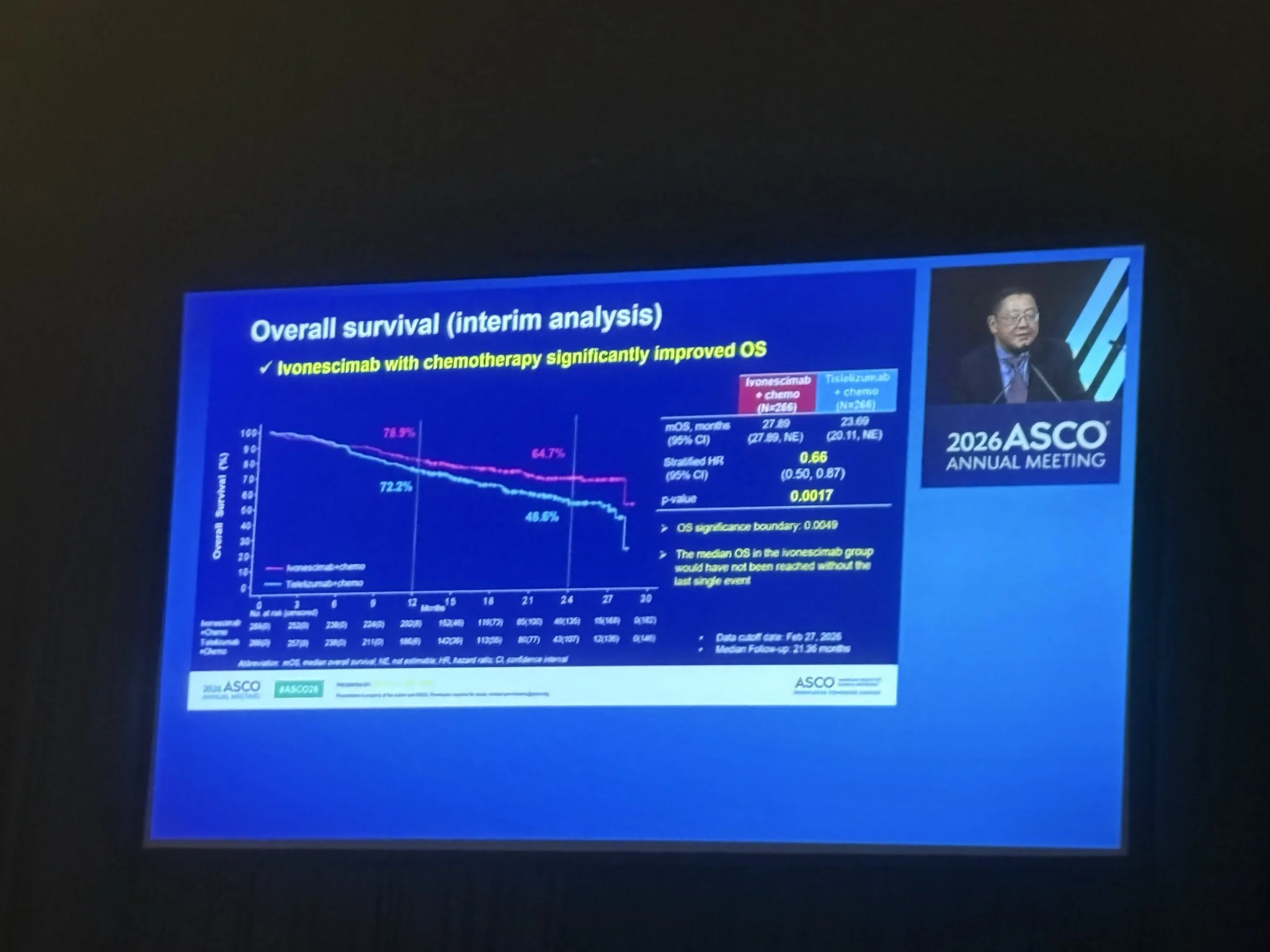
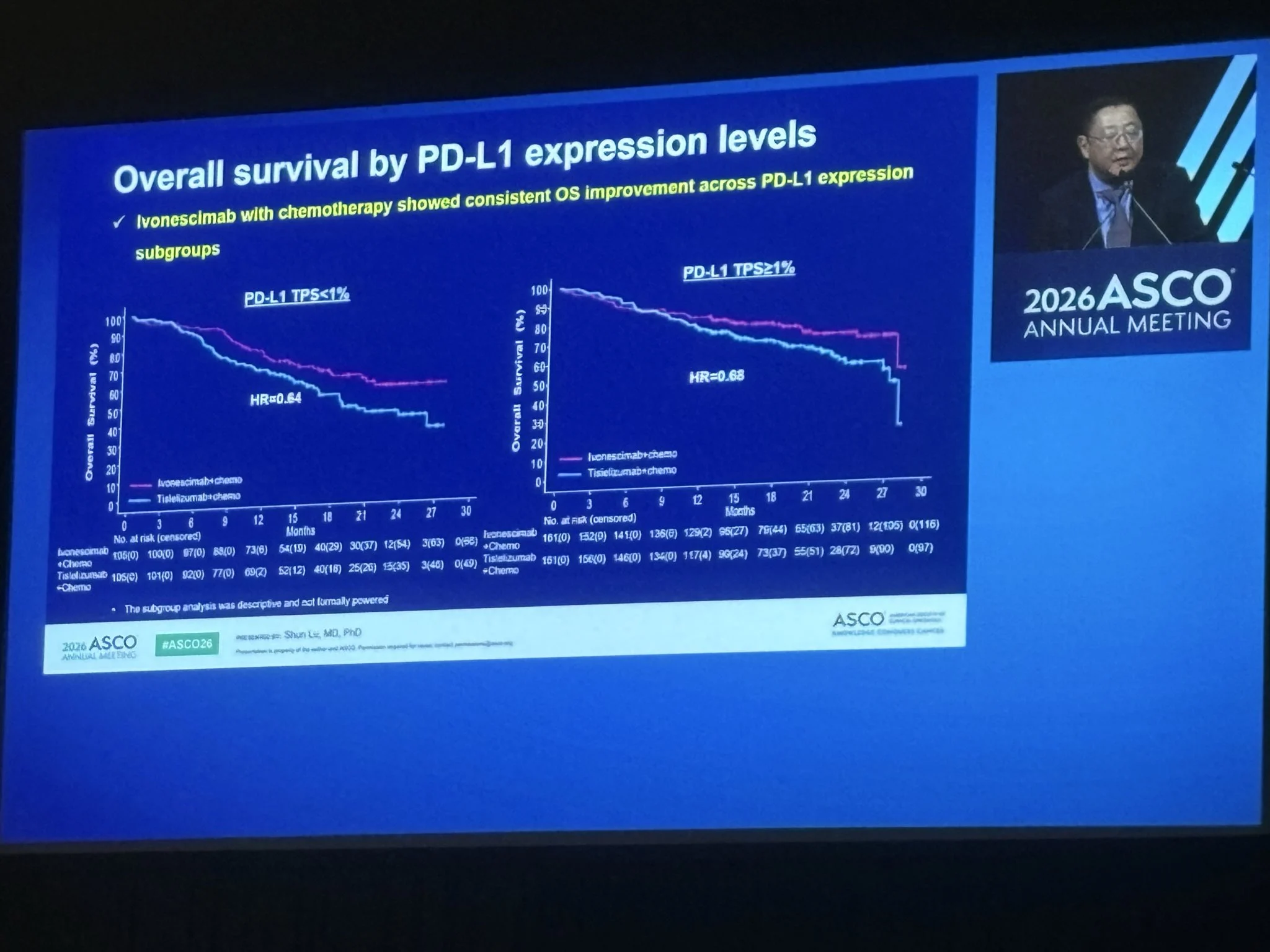
“One of the most awaited presentations( at least by me), ASCO26: HARMONi-6, shows that ivonescimab + chemo significantly improves OS Vs tislelizumab + chemo in first-line advanced Sq NSCLC (HR 0.66). A positive phase III study with a clinically meaningful OS benefit and simultaneous publication in The Lancet
Caveat: this was a study conducted entirely in China. How these data will translate globally remains an important question?”
“Let’s see what HARMONI 3 will show.”

Read more on the HARMONi-6 trial:
HARMONi-6 Trial at ASCO Plenary 2026: Ivonescimab Plus Chemotherapy Improves Overall Survival in Advanced Squamous Non-Small Cell Lung Cancer

Sakditad “Tew” Saowapa
“Lol, fun and good metaphor for VEGF targeting in sq NSCLC.
- 2006: Bevacizumab + chemo in NSCLC (NEJM) – The Devil Wears Prada drops
- 2026: Ivonescimab + chemo vs tislelizumab + chemo in sq NSCLC (HARMONi-6, The Lancet) – The Devil Wears Prada 2 hits theaters.”
“What’s old is new again – VEGF blockade is back in fashion.”

Balazs Halmos
“I don’t know if they wore Prada or not but double shout-out for 2 fantastic presentations by two legendary and very stylish Women in Thoracic Oncology leaders at ASCO26 plenary!”

Amol Akhade
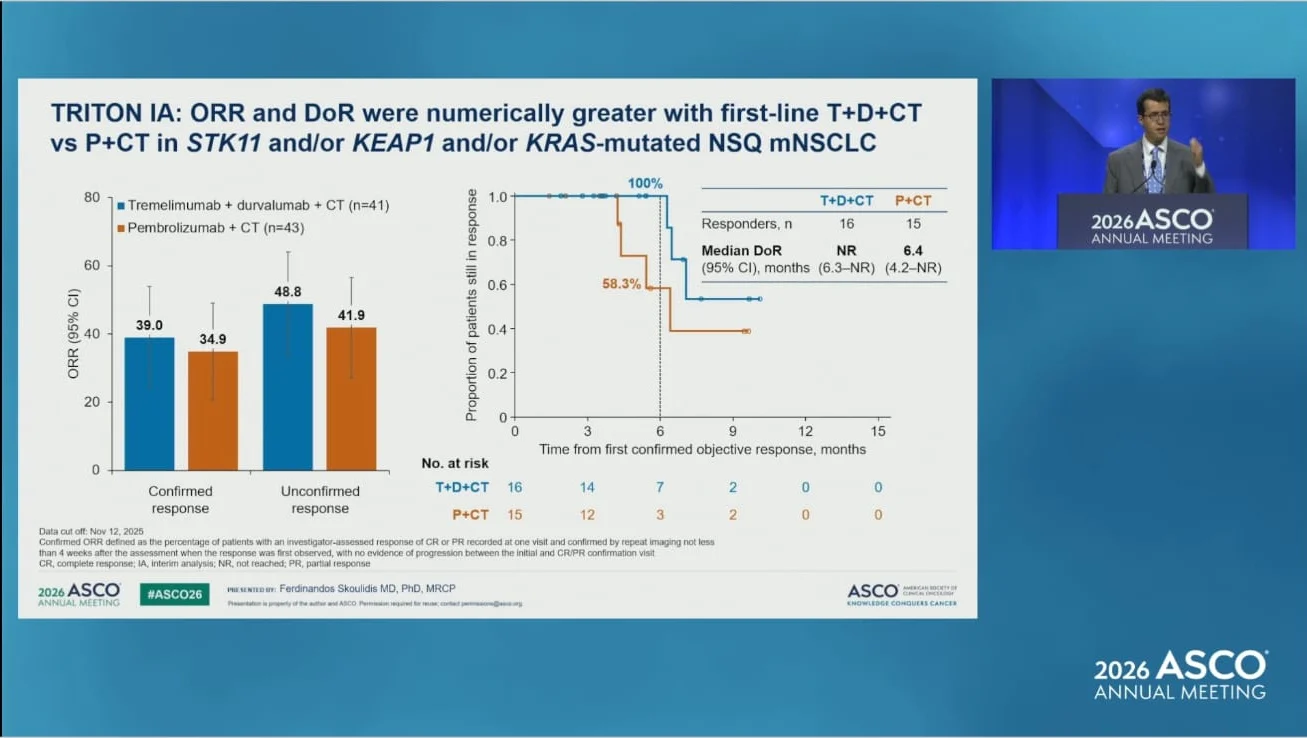
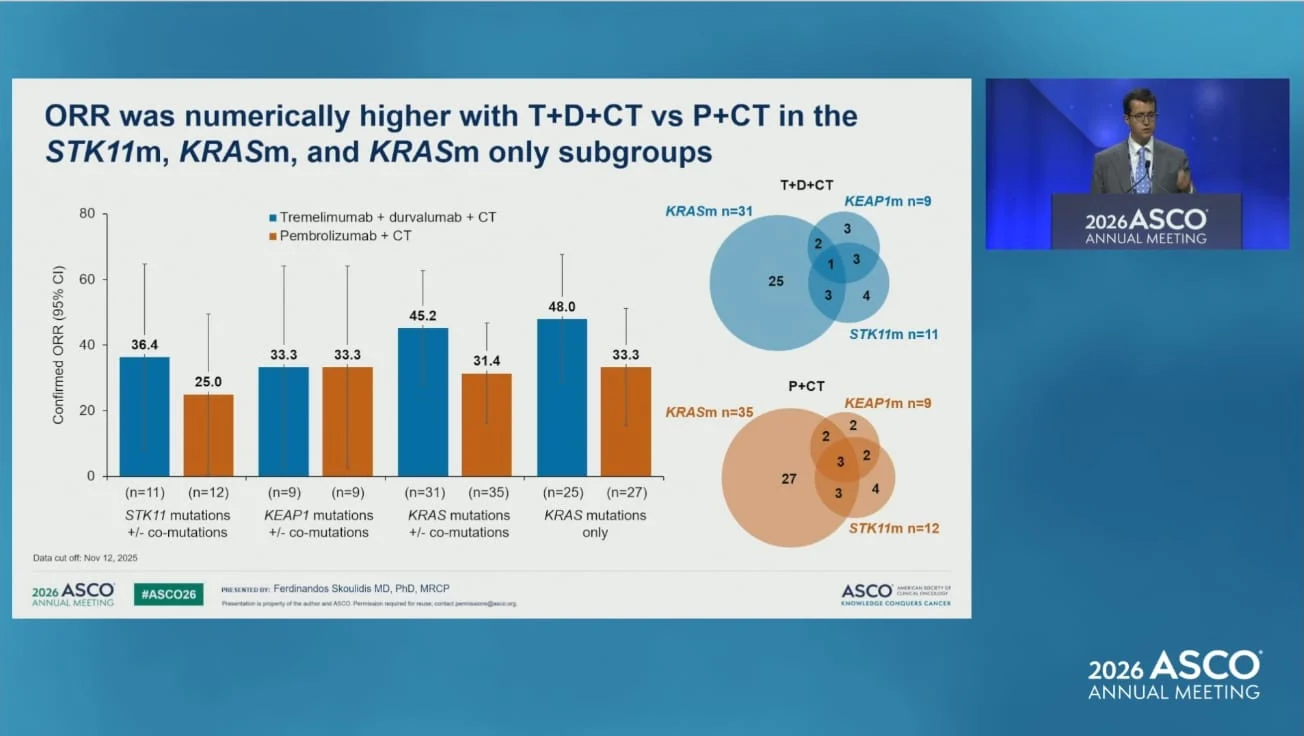
“ASCO 2026 | TRITON IA
Tremelimumab + Durvalumab + Chemotherapy vs Pembrolizumab + Chemotherapy
- Confirmed ORR: • 39.0% vs 34.9%
- Unconfirmed ORR: • 48.8% vs 41.9%
- Duration of Response: • Not reached vs 6.4 months
Subgroup signals favored the CTLA-4/PD-L1 combination:
- STK11-mutant: 36.4% vs 25.0%
- KRAS-mutant: 45.2% vs 31.4%
- KRAS-mutant only: 48.0% vs 33.3%
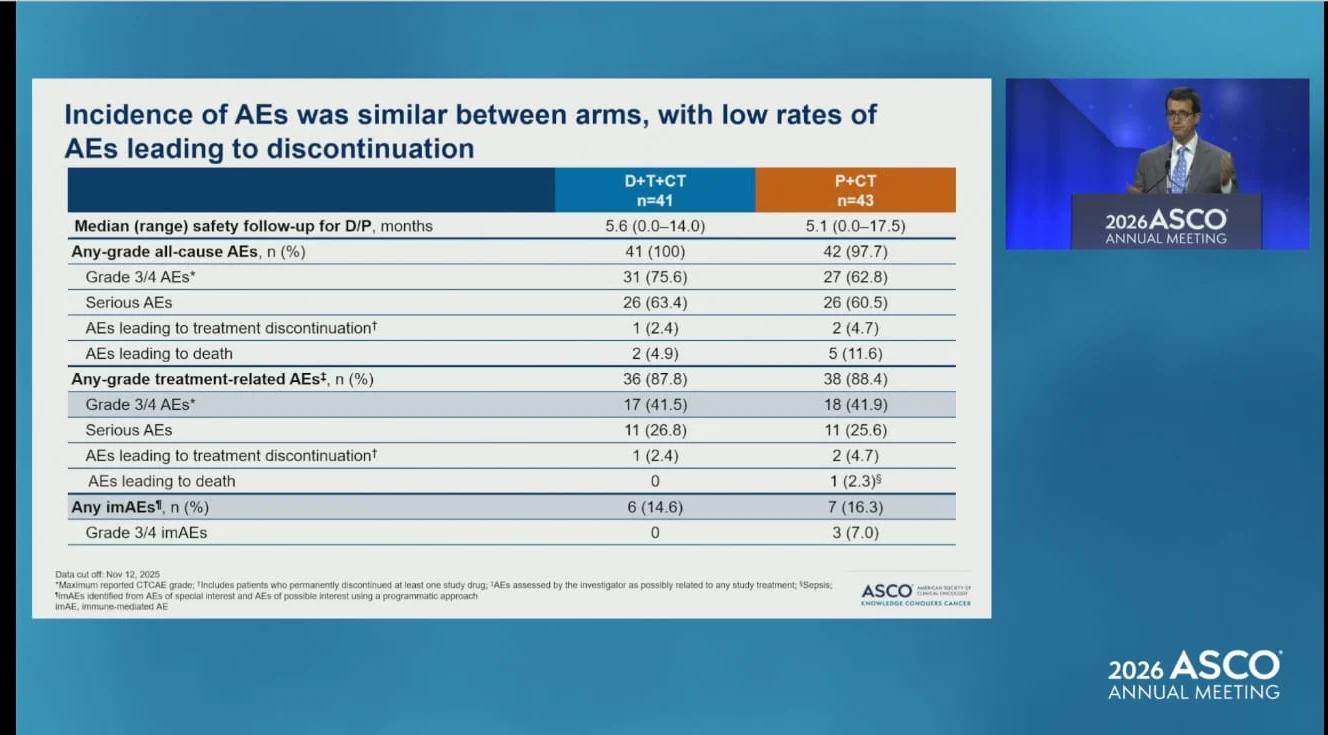
Safety was broadly comparable between arms, with low discontinuation rates and no new safety signals.
These are early, small-number data, but they align with prior observations from POSEIDON that adding CTLA-4 blockade may help overcome resistance associated with STK11/KEAP1 biology.
Interesting signal. Practice-changing? Not yet.”

Read also:
TRITON Interim Analysis: Tremelimumab Plus Durvalumab And Chemotherapy Shows Early Response Signal In STK11/KEAP1/KRAS-Mutated NSCLC

Antonio Calles
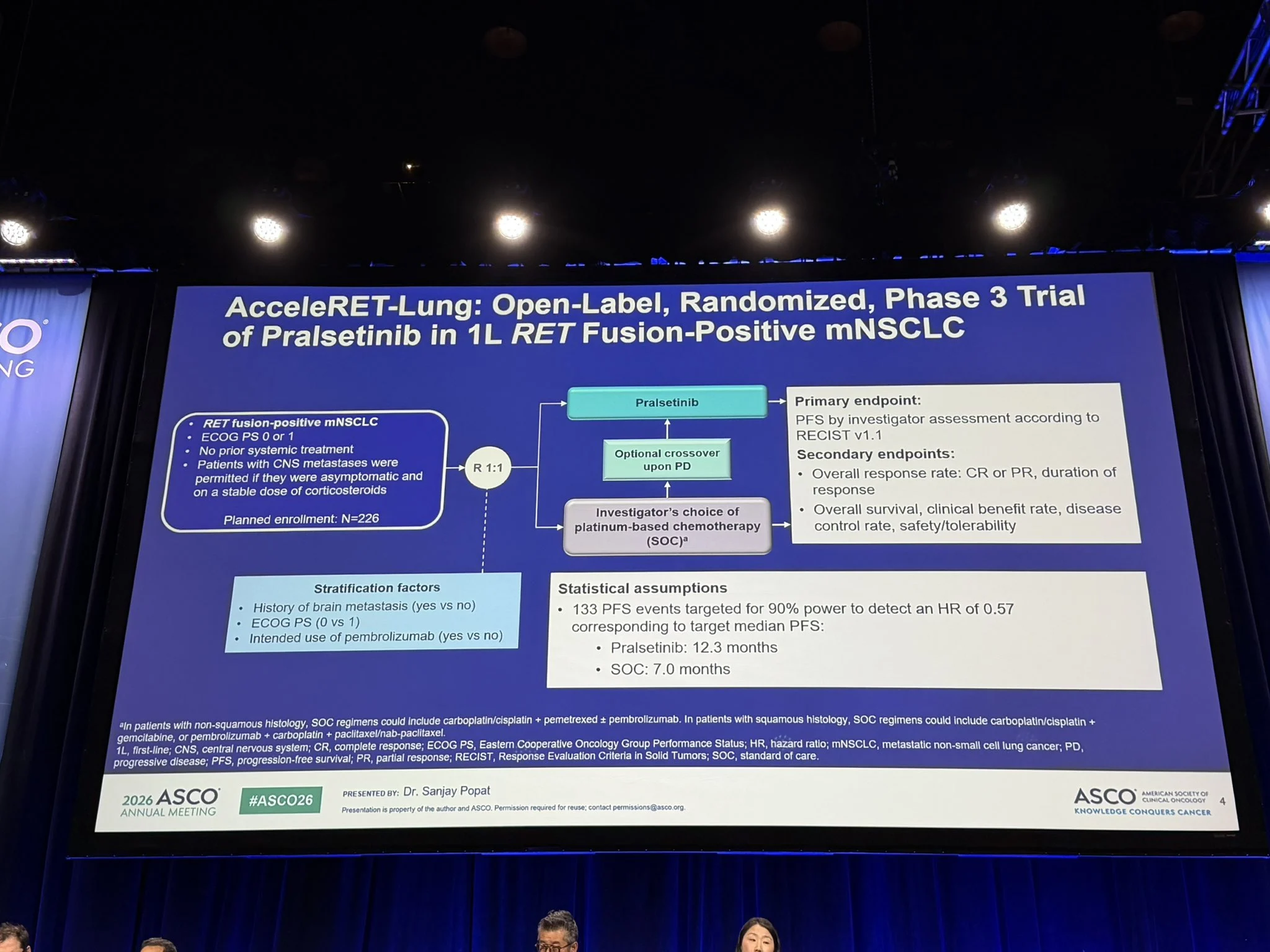
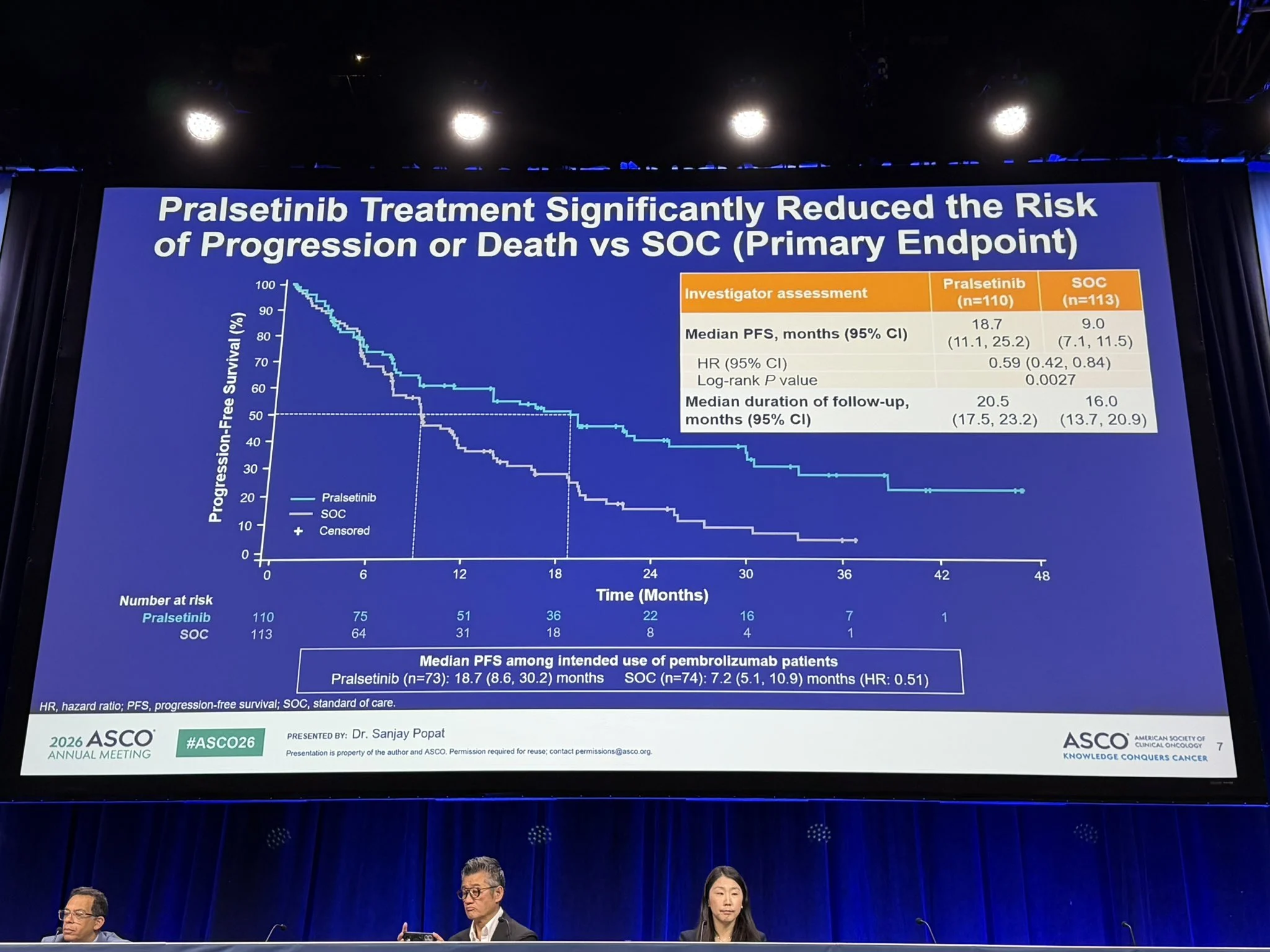
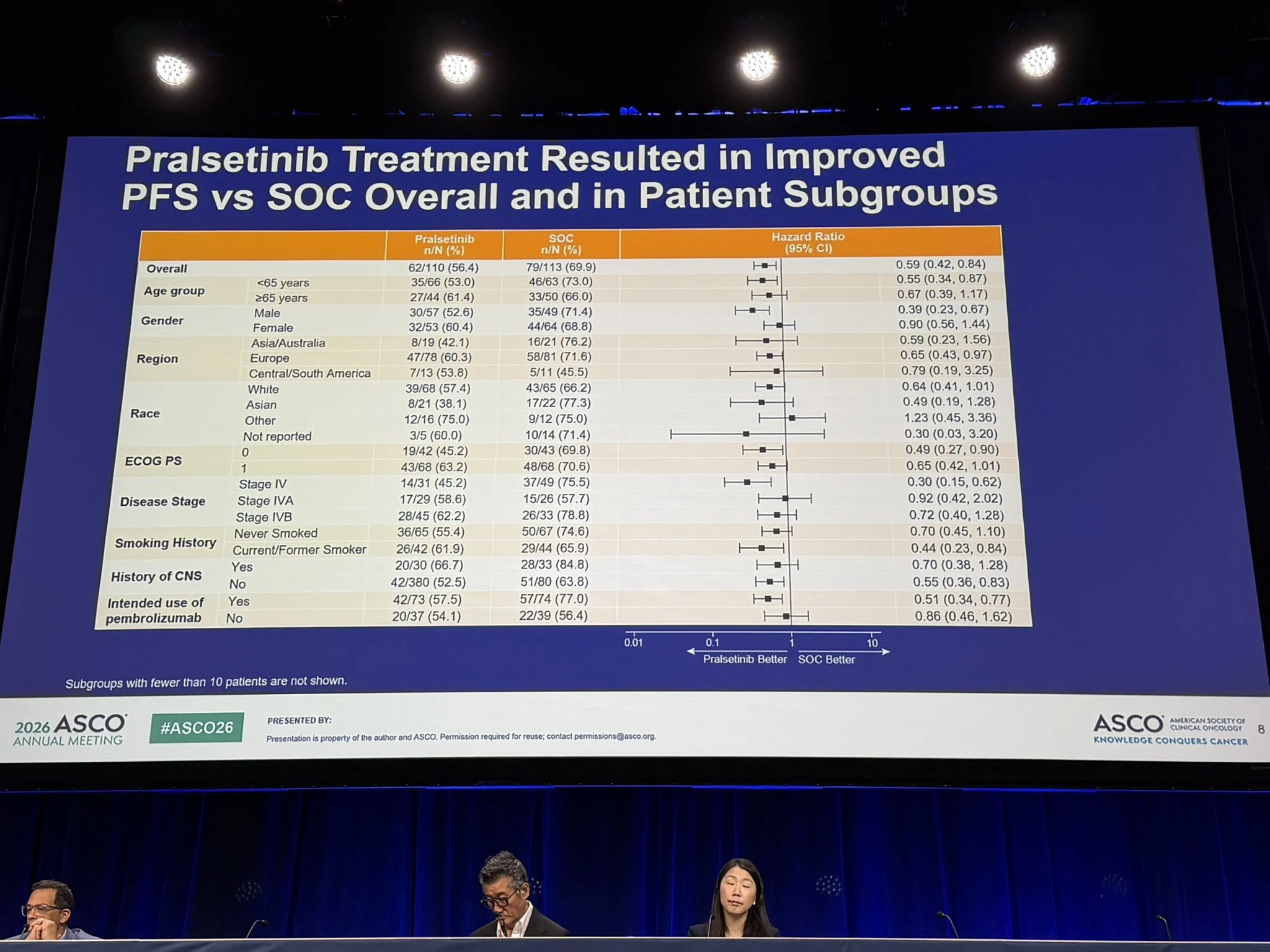
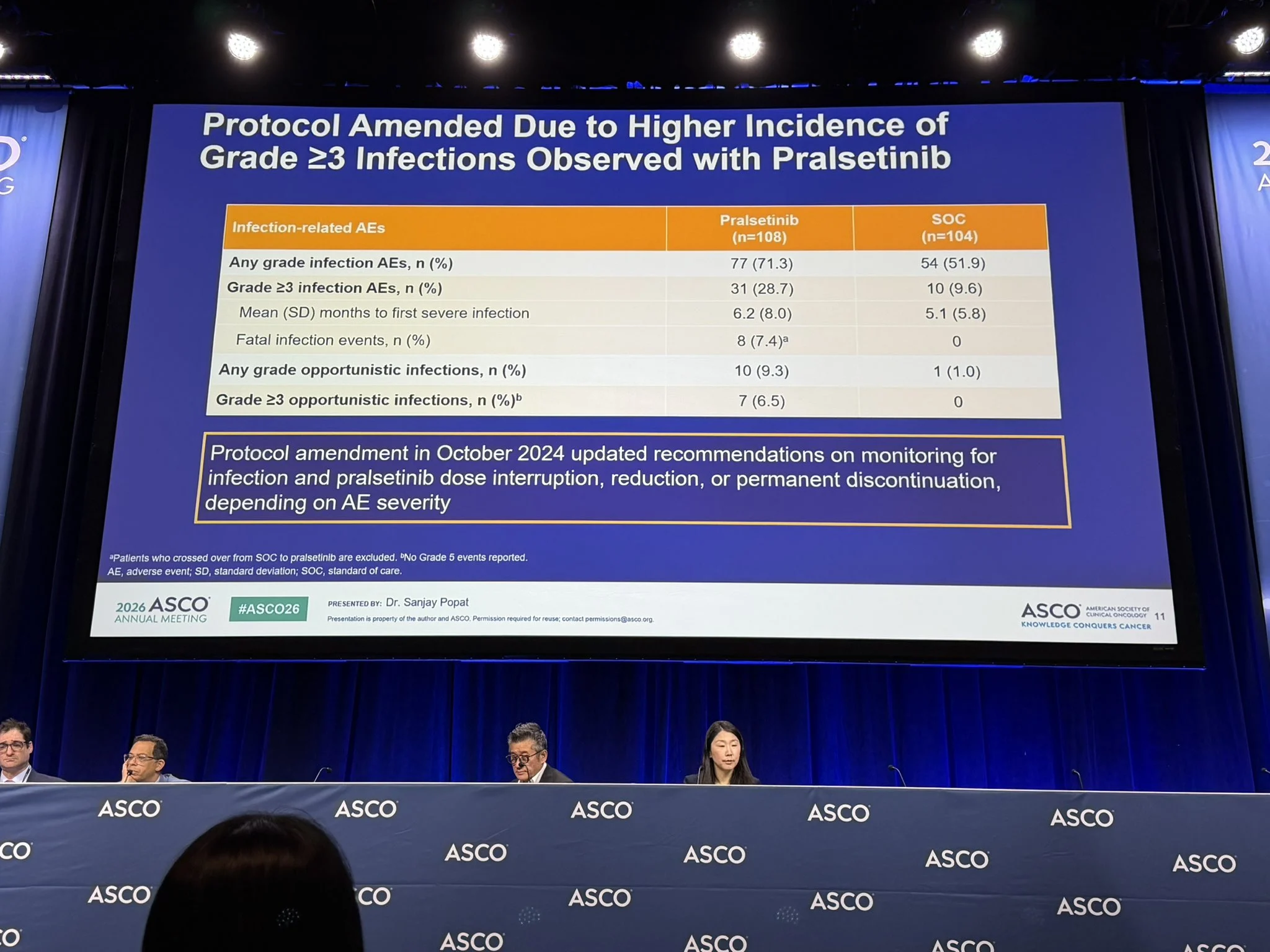
“AcceleRET-LUNG: Pralsetinib improved PFS vs SOC 1L chemo-IO in RET+ NSCLC
Special attention to an increased risk of infections.
Phase III trials still needed to properly assess benefit/risk ratio and detect uncommon toxicities but exemplifies the multiple challenges facing in infrequent conditions with competitive alternatives.”

Ana I. Velázquez Mañana
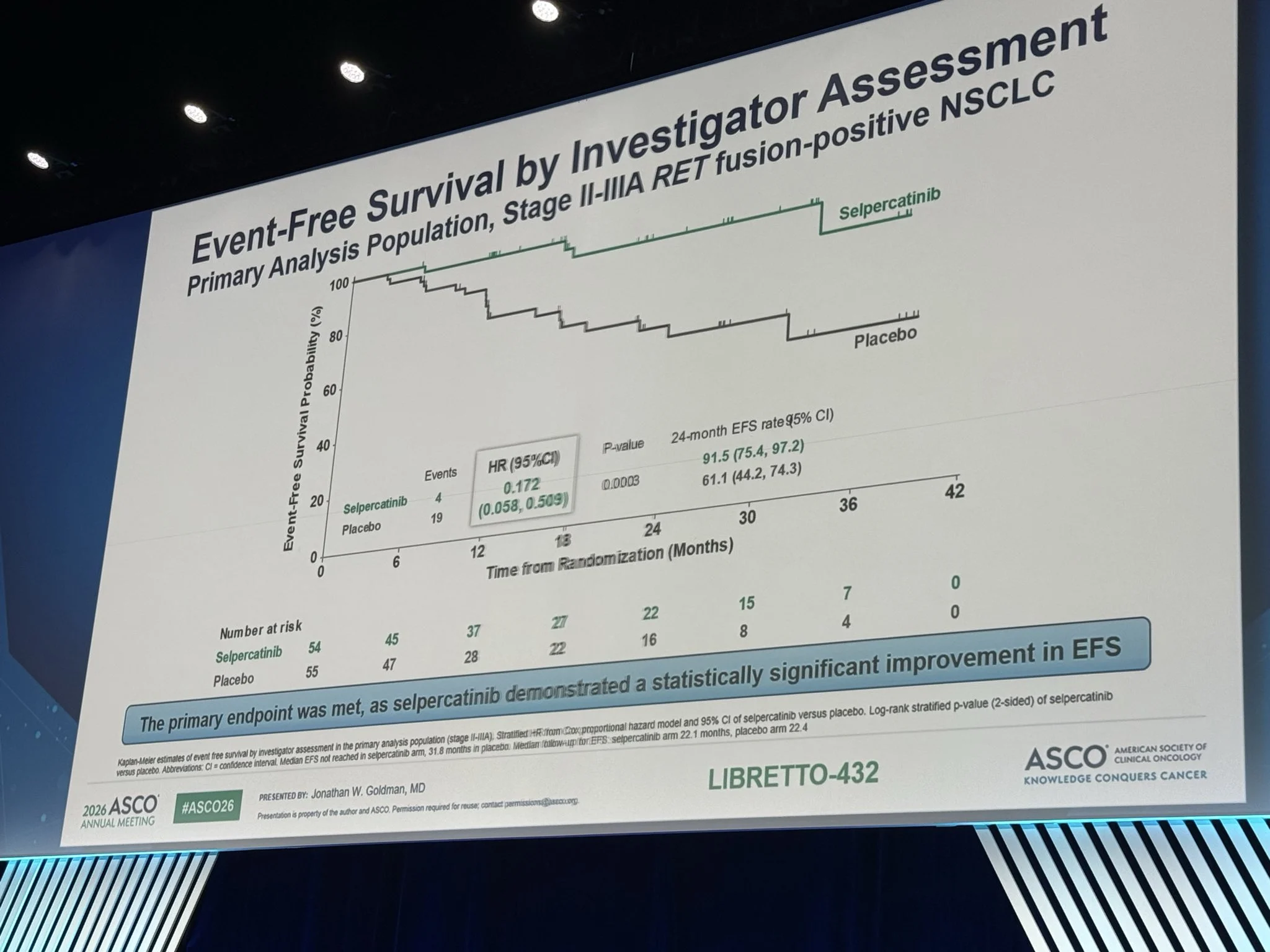
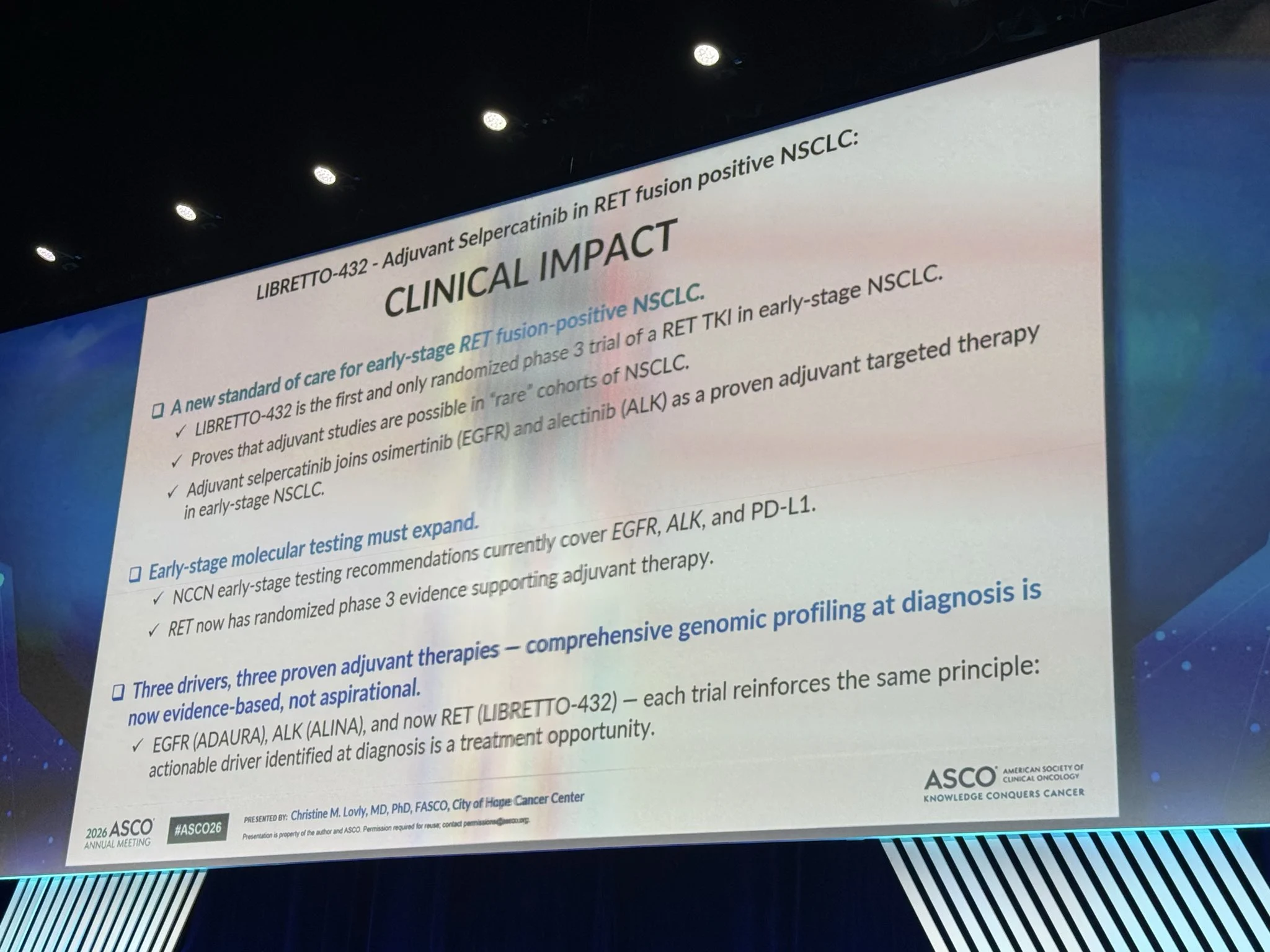
“LIBRETTO-432 Adjuvant selpercatinib significantly prolonged EFS in early-stage RET+ NSCLC presented at ASCO26
As nicely summarized by Christine Lovly, broad NGS testing of early-stage diagnosis in a population that doesn’t meet Lung Cancer screening criteria, side effect management, survivorship, cost and global access remain limited and are key challenges that limit adoption of this highly effective therapy.”

Balazs Halmos
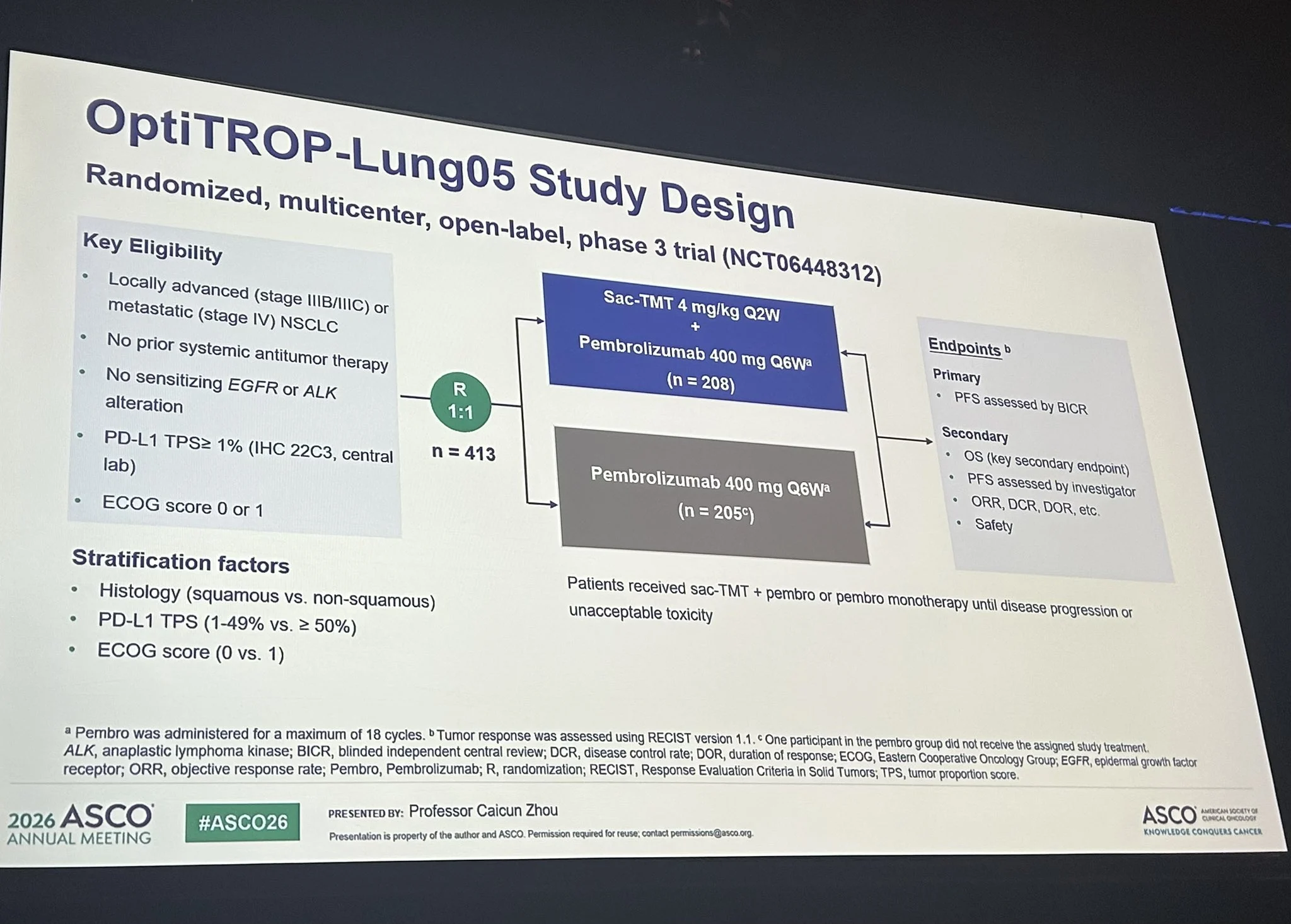
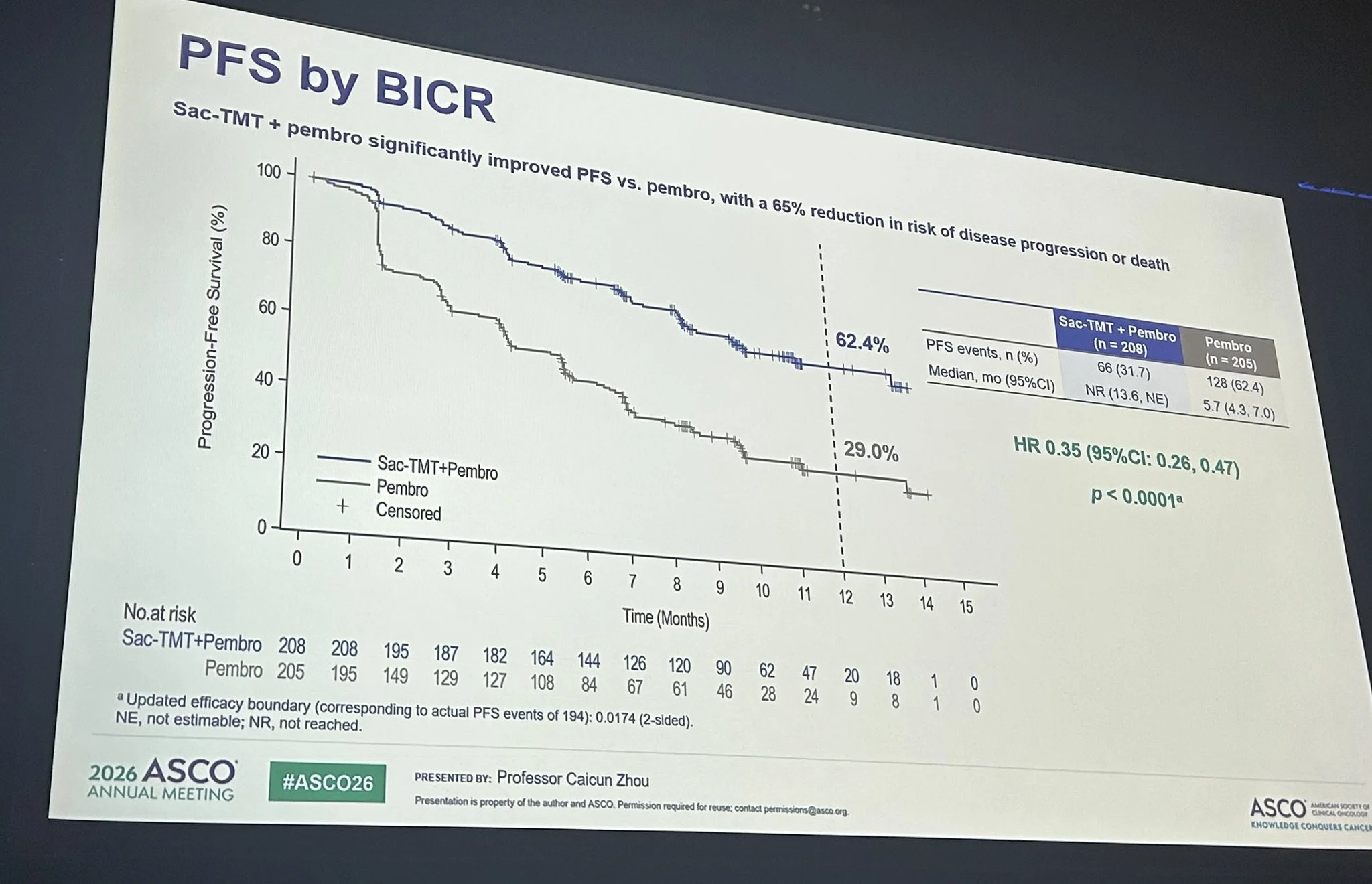
“OptiTROP-Lung05– should we be Optimists about the use of Trop2 ADCs frontline for advanced PD-L1+ NSCLC?
Well- in light of much improved RR and impressive PFS (better for tps 1-49 and. NonSQ) + clear trends for OS benefit with an expected AE profile w/o worrisome signals:
“I’d say- lets bring on the Trops!”

Read further on OptiTROP-Lung05, AcceleRET-Lung, and LIBRETTO-432.
Gastrointestinal Сancer
Benjamin L. Ebert
“A major breakthrough was just presented at American Society of Clinical Oncology (ASCO) for the treatment of pancreatic cancer. The Phase 3 clinical trial showed that a new drug, daraxonrasib, more than doubles survival of patients with previously treated metastatic pancreatic cancer, compared to chemotherapy treatment. Not only do these findings have the potential to redefine the standard of care for pancreatic cancer, but they also offer renewed hope for continued advances for patients facing this devastating disease.
“The thousands of usually staid oncologists in the audience rose for an emotional standing ovation. New treatments with this magnitude of benefit remain exceedingly rare, and unprecedented for pancreatic cancer, one of the most lethal and difficult to treat cancers.”
The results were presented by Brian Wolpin, Dana-Farber Cancer Institute’s Robert T. and Judy B. Hale Chair in Pancreatic Cancer and Director of our Gastrointestinal Cancer Center, who led this clinical trial and presented it in the plenary session of the ASCO meeting. Brian has devoted his career to treating patients with pancreatic cancer and to developing new therapies. The unprecedented findings presented today will benefit patients with pancreatic cancer around the world. This advance shows, once again, how rigorous science and innovative drug development can lead to transformative progress for previously intractable diseases.”

Yüksel Ürün
“This is not simply a new pancreatic cancer drug.
It is a reminder that even “undruggable” biology can become treatable with persistence.”
“Daraxonrasib doubled median OS vs chemotherapy in RAS G12 metastatic pancreatic cancer: 13.2 vs 6.6 months.
A remarkable ASCO moment.”

Read more on RASolute 302 Trial:
RASolute 302 Trial at ASCO 2026 Plenary Session: Daraxonrasib Improves Survival Versus Chemotherapy in Previously Treated Metastatic PDAC

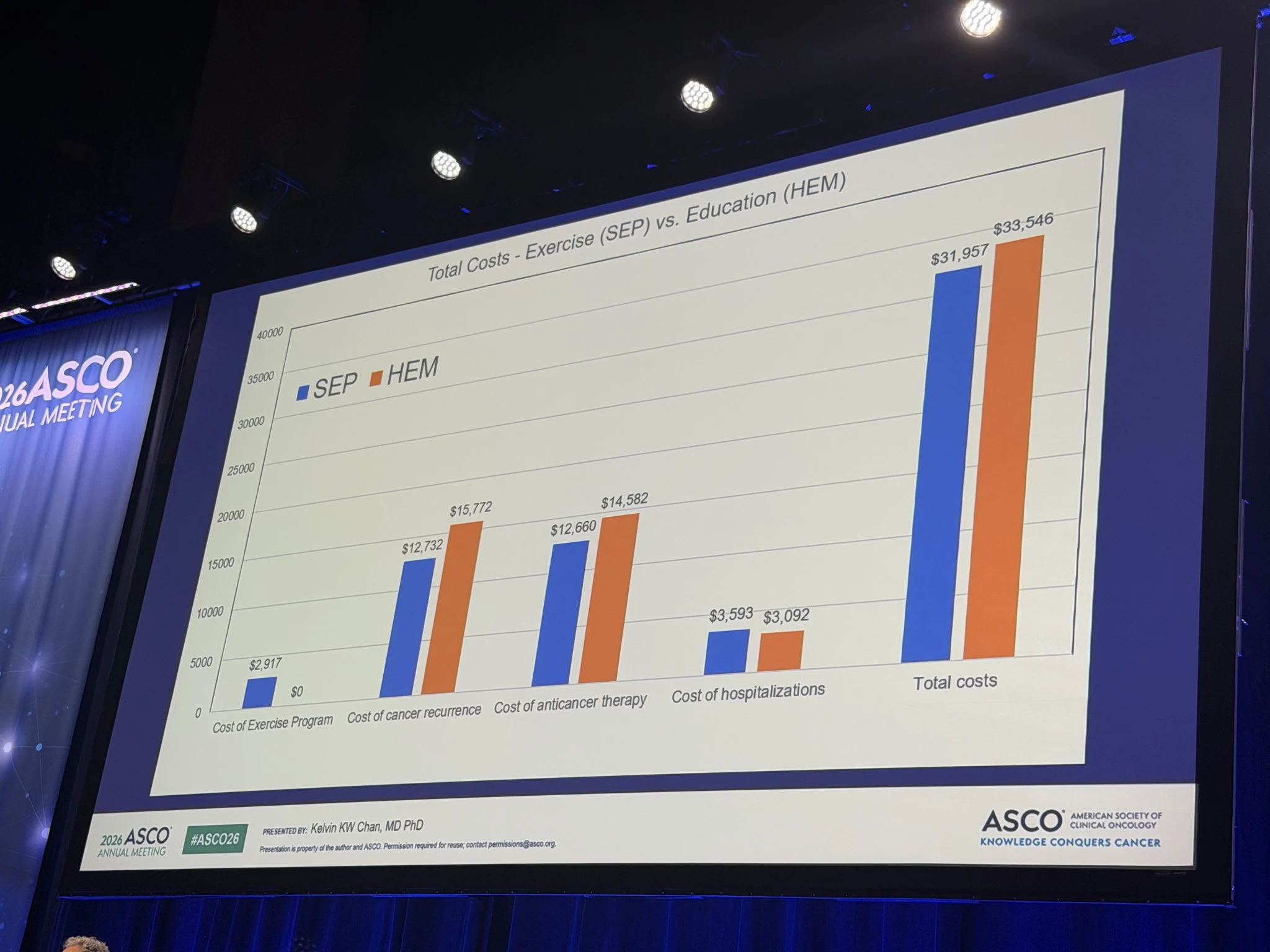
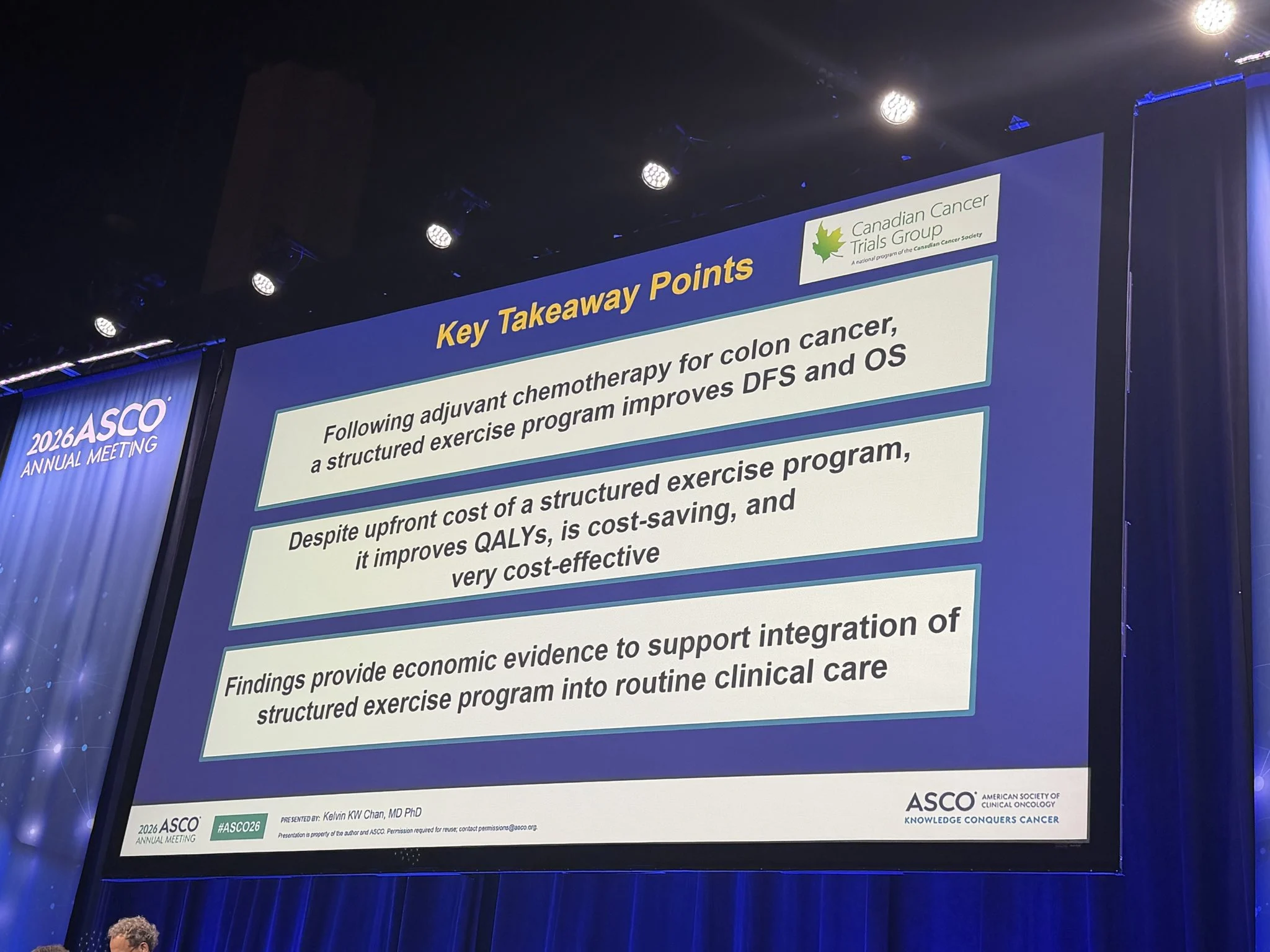
Sharlene Gill
“Cost-utility analysis of CHALLENGE trial of structured exercise (SEP) after ACT for stage 2-3 colon cancer CCTG.
- SEP improves DFS and OS
- SEP is less costly and more effective ‘Win-Win’
- We need to implement SEP into routine care”

Arndt Vogel
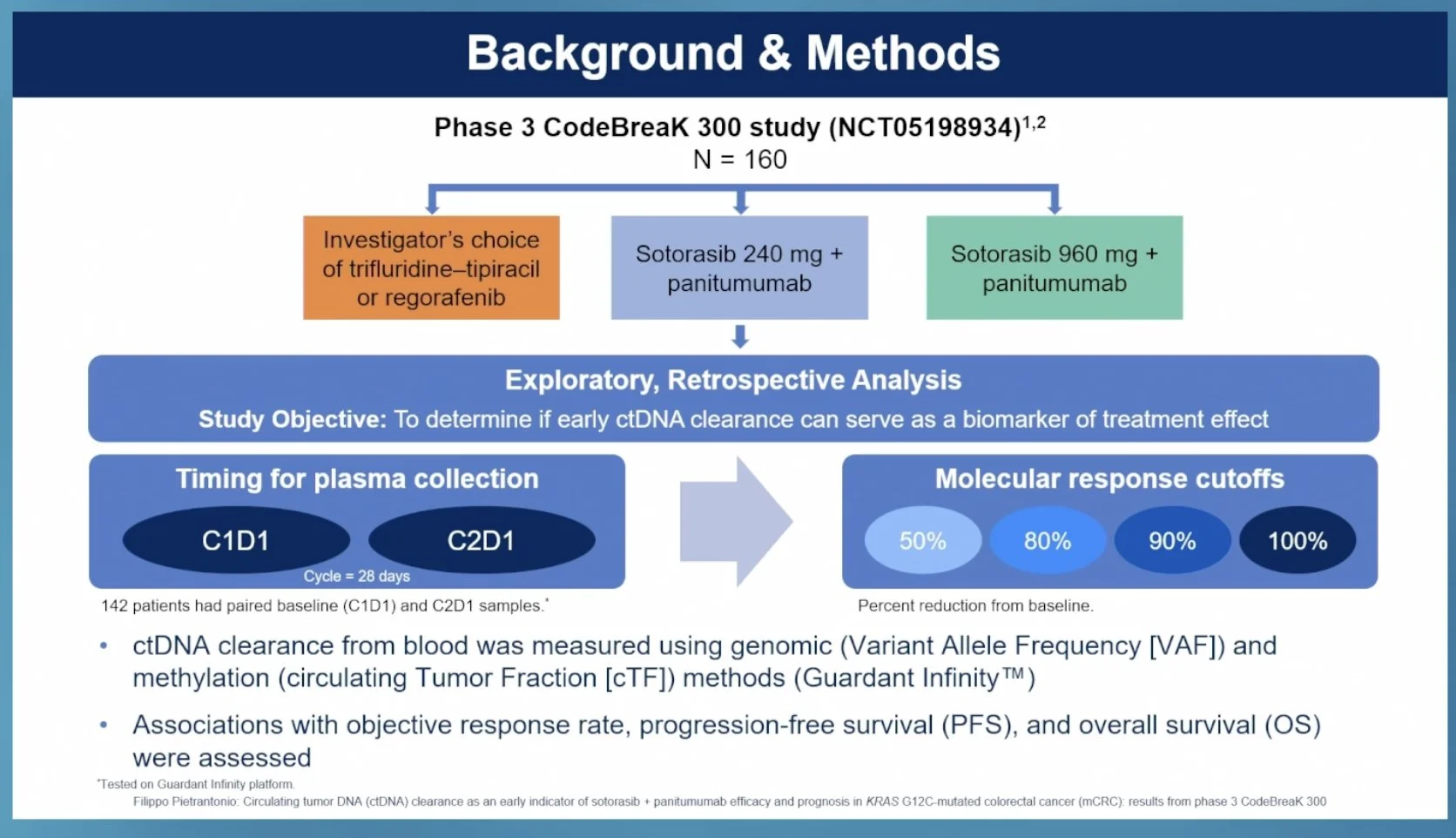
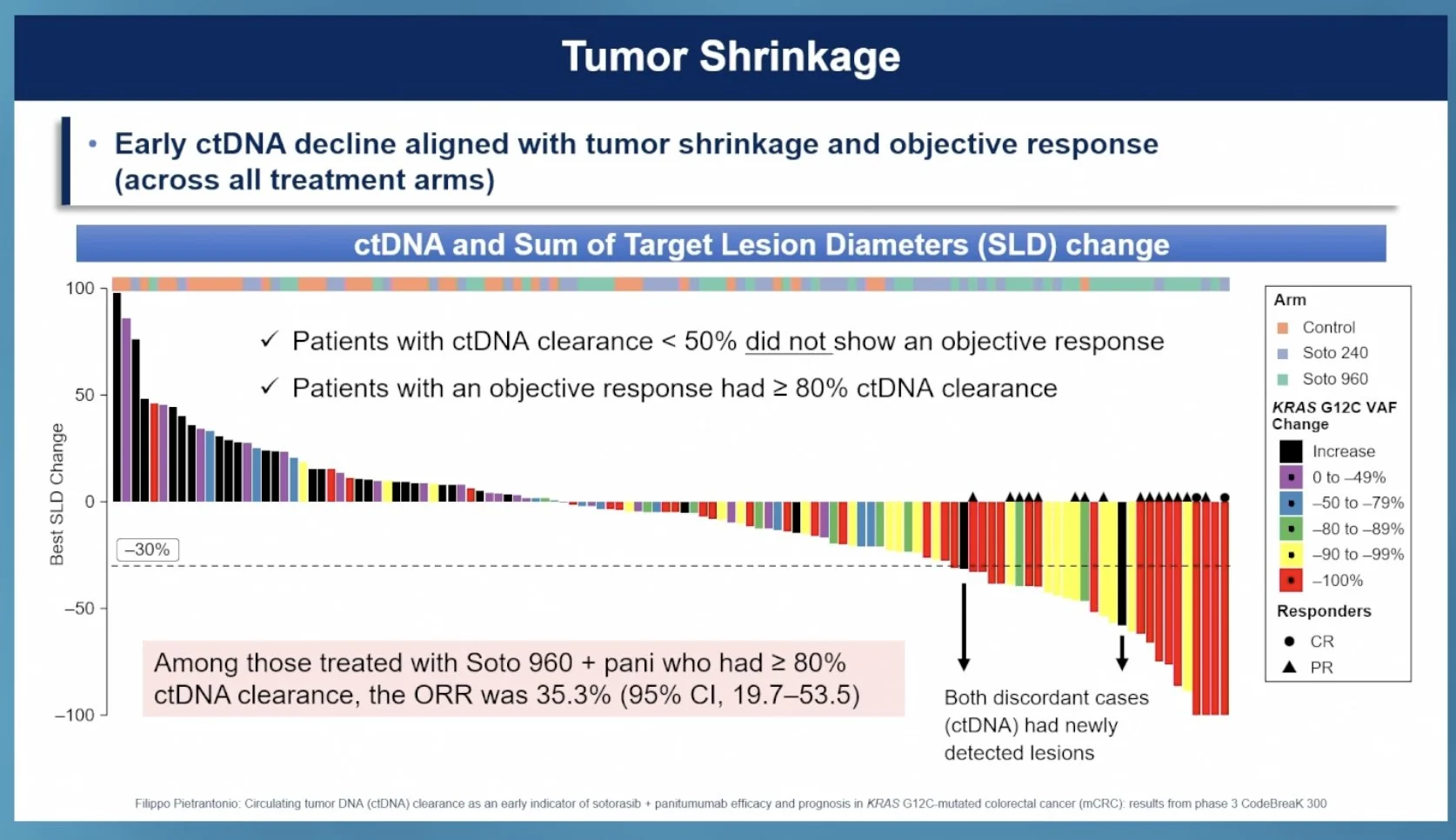
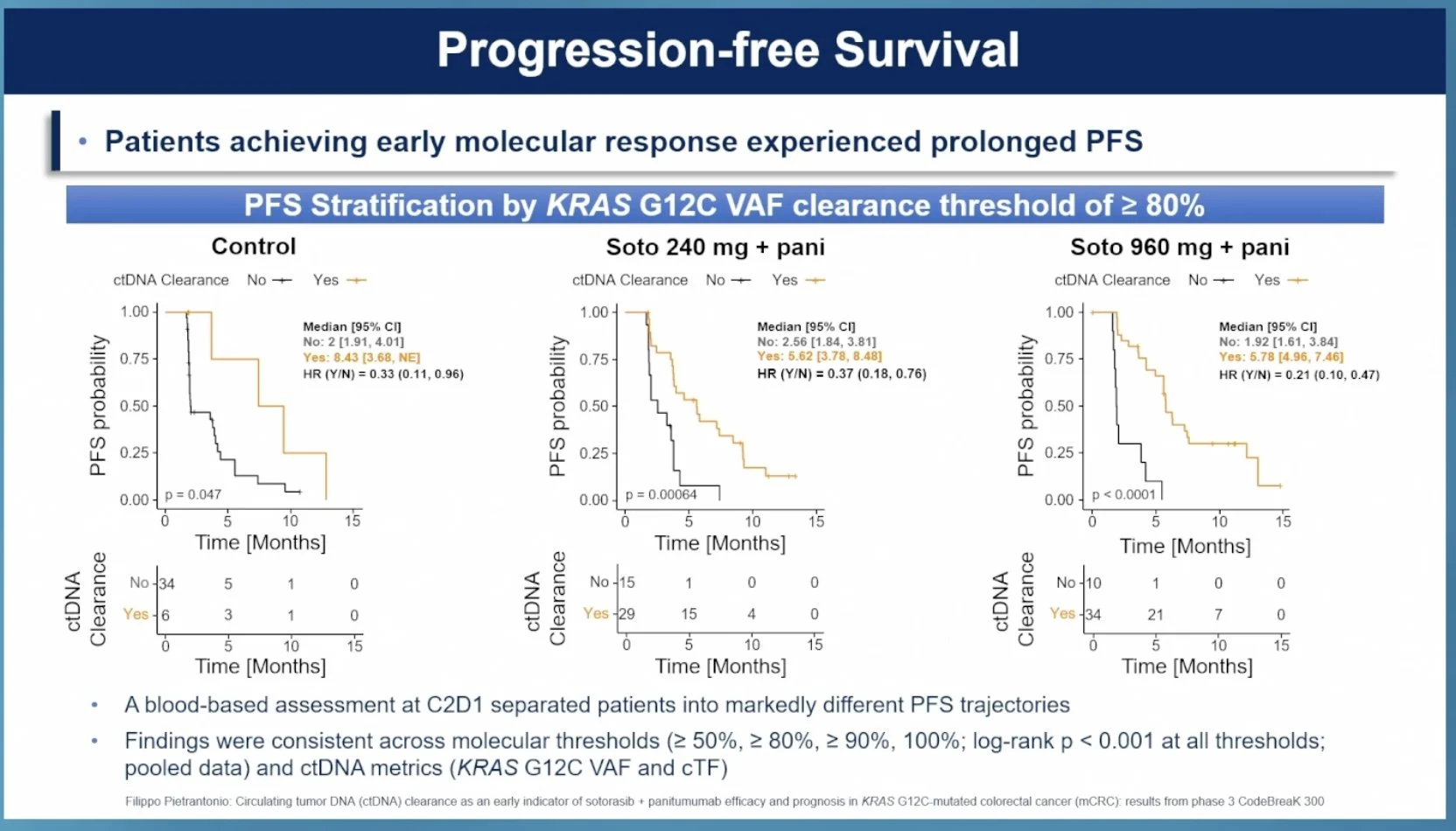
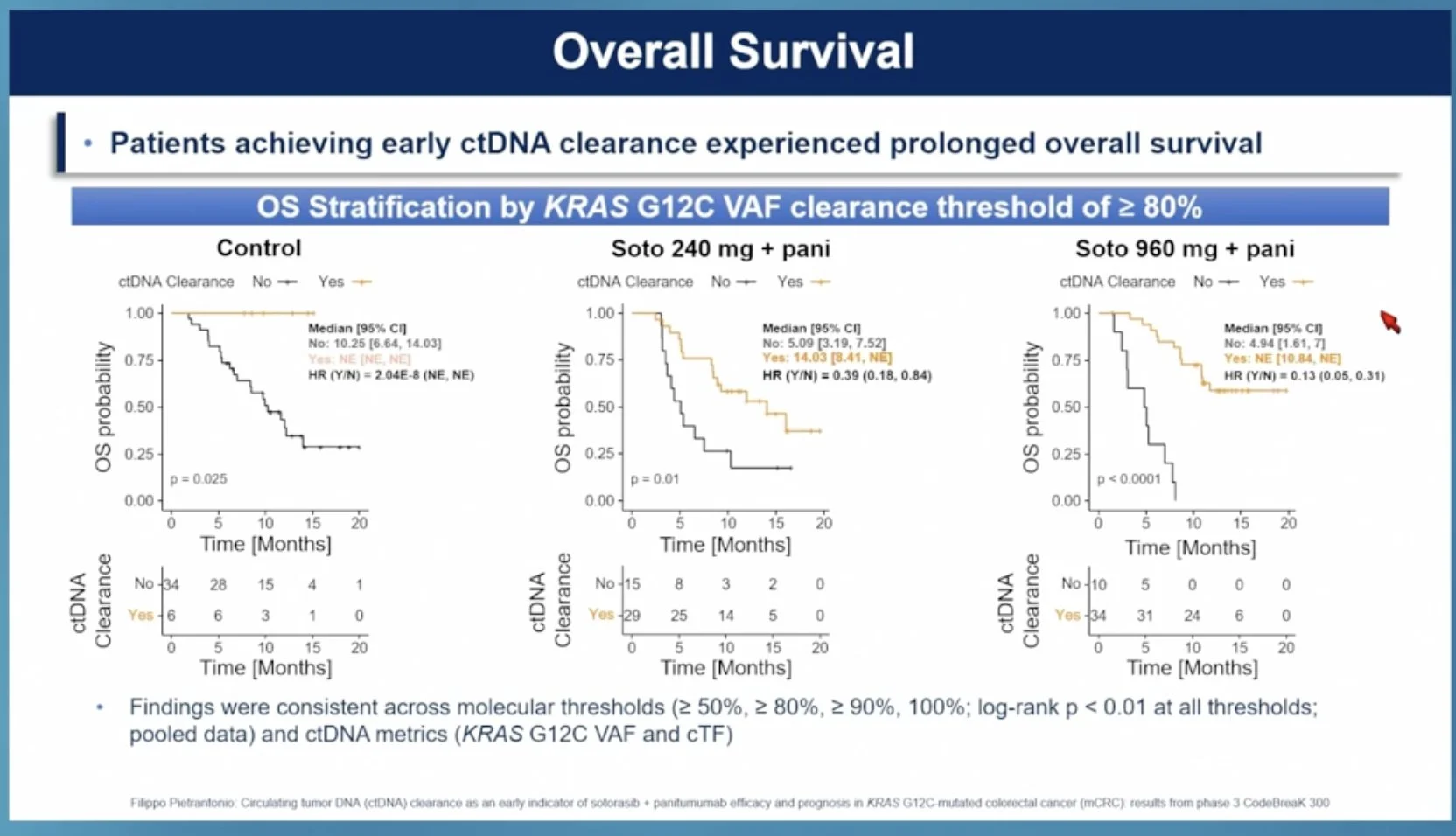
“ctDNA clearance as an early indicator of sotorasib + panitumumab efficacy and prognosis in KRAS
G12C–mCRC: Results from phase 3 CodeBreaK 300
- ctDNA clearance = early biomarker for response
- Significantly higher with sotorasib
- Could be useful in the clinic”

Read also:
CodeBreaK 300 at ASCO 2026: ctDNA Clearance Evaluated as an Early Response Biomarker in KRAS G12C-Mutated mCRC

Eduardo Terán
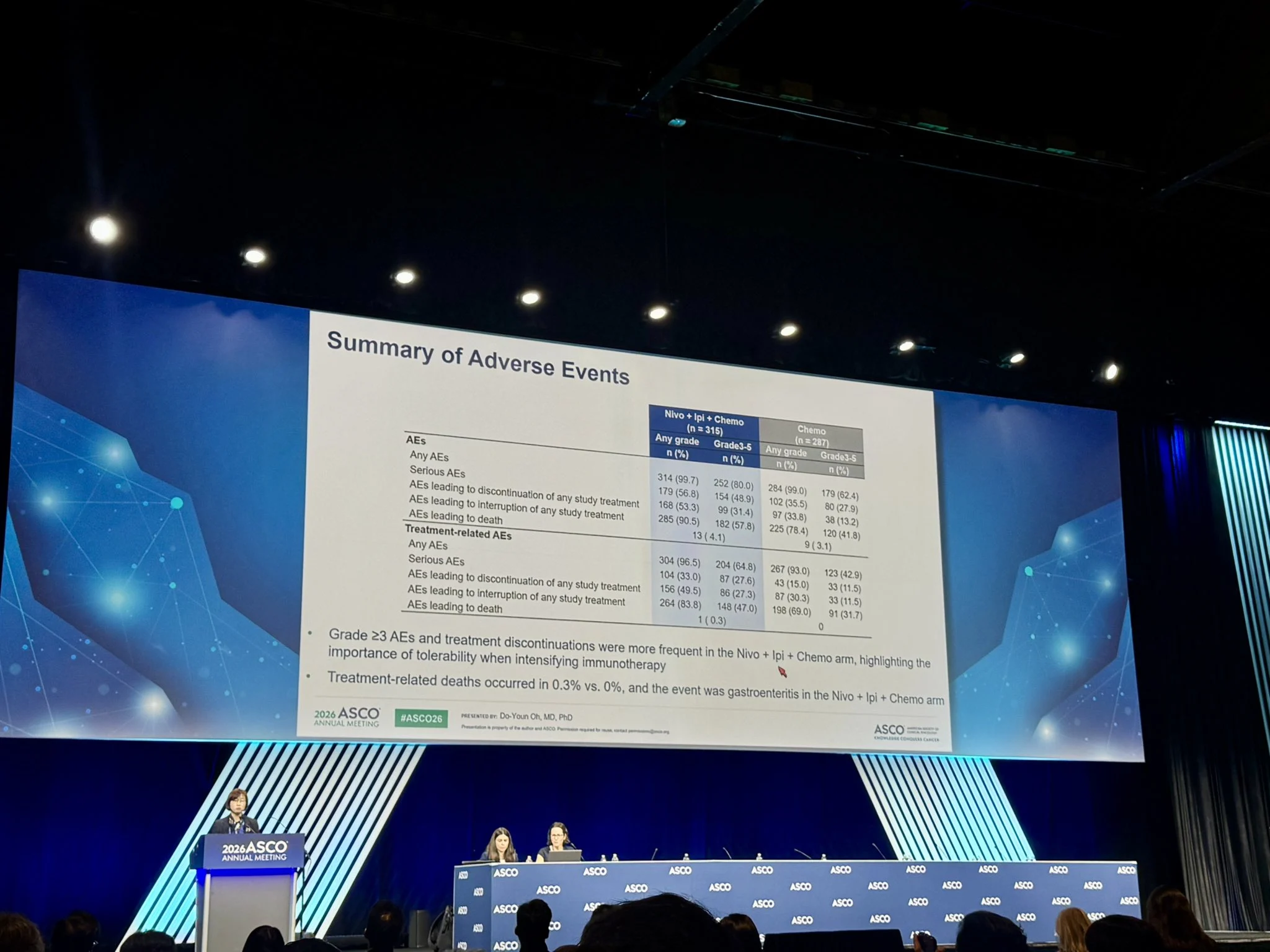
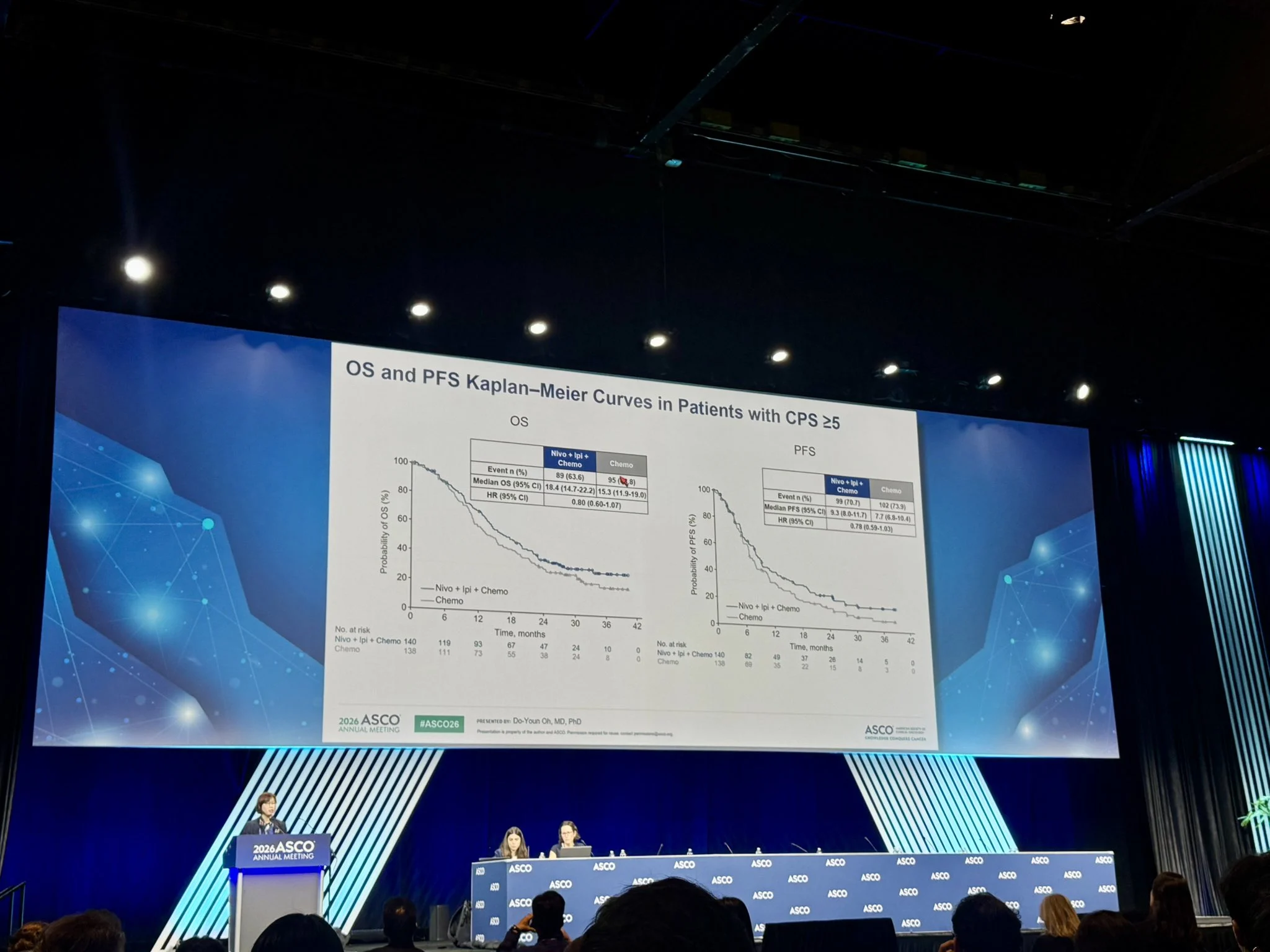
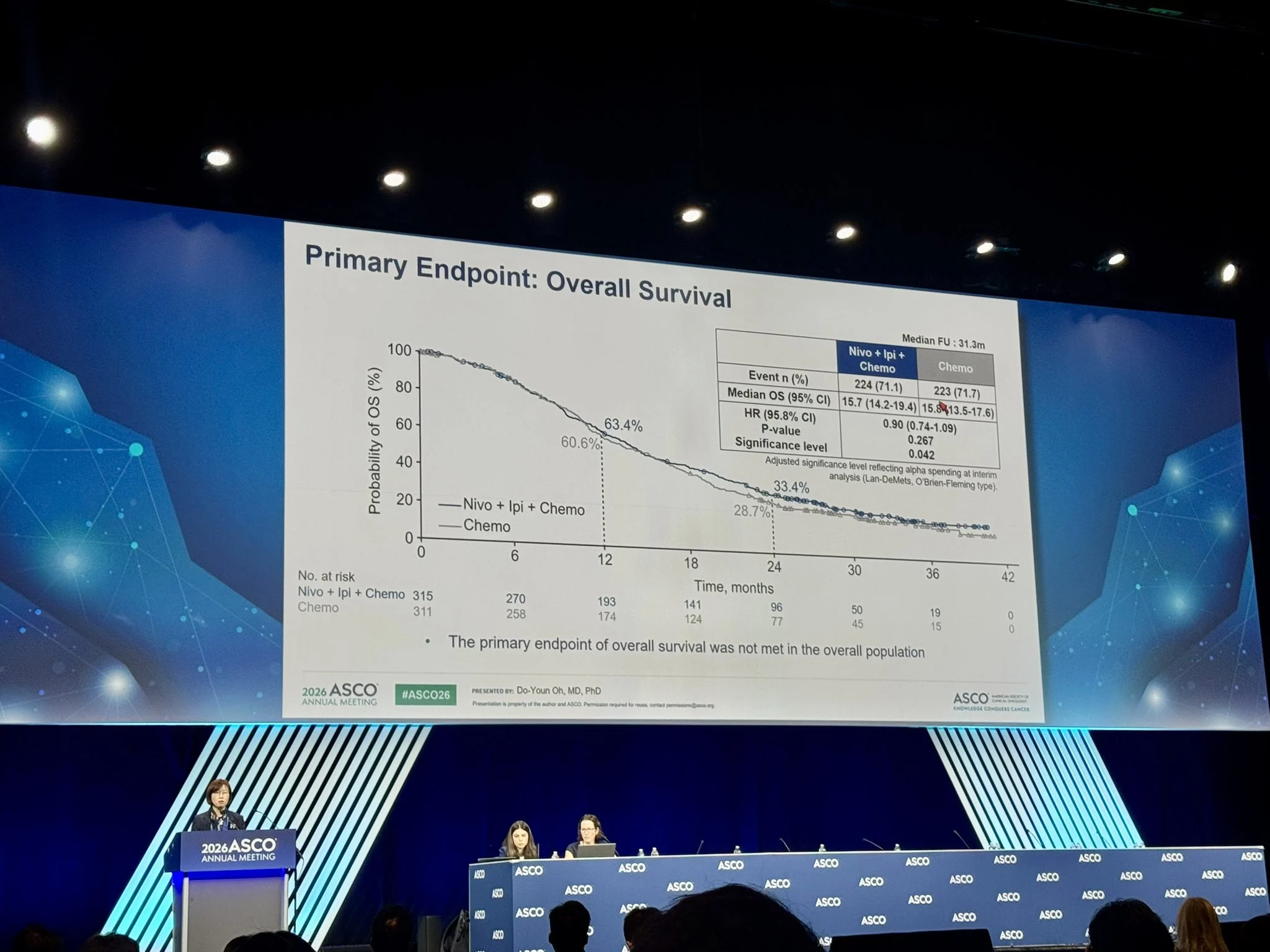
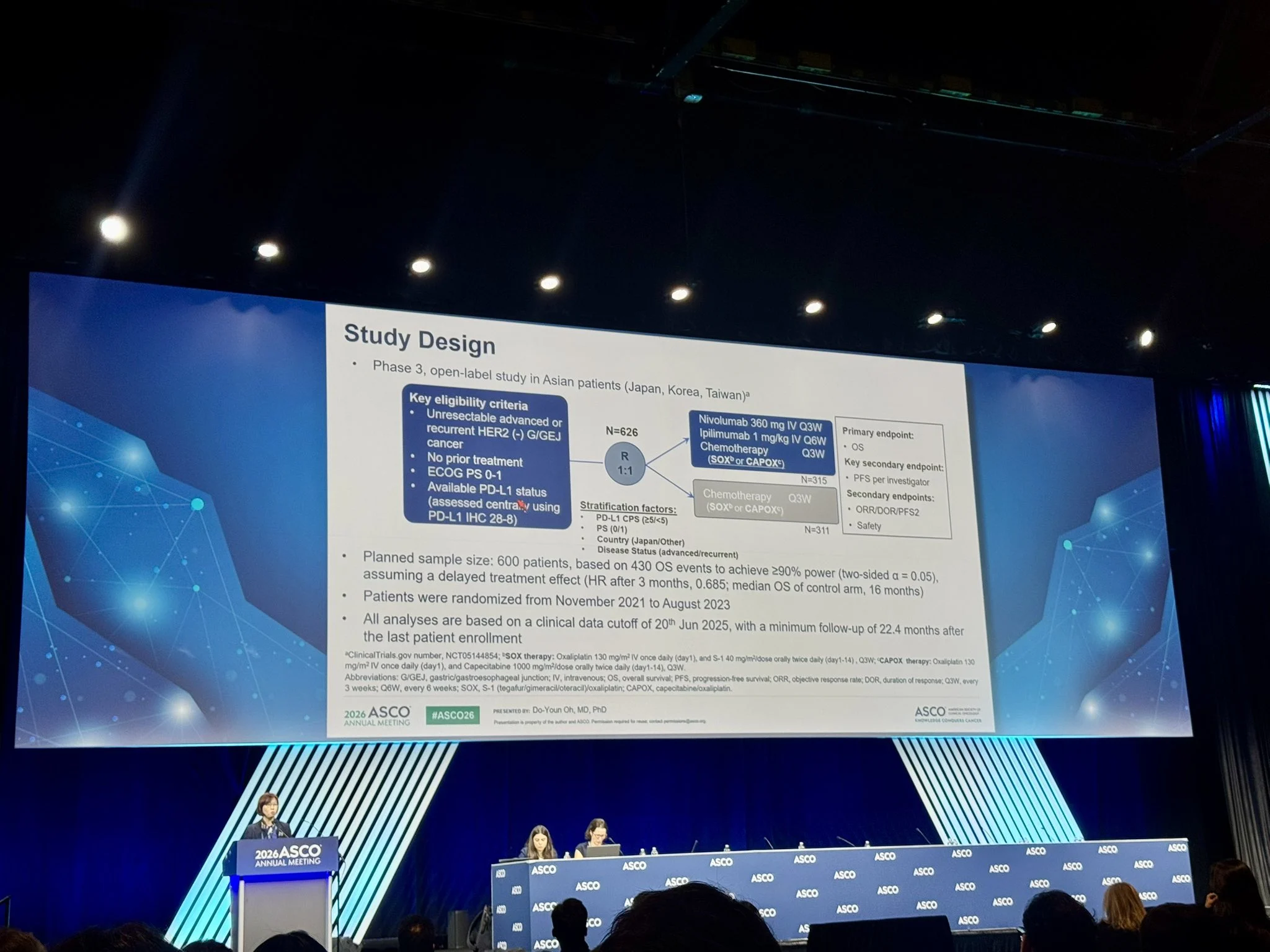
“ATTRACTION-6. Adding IPI to NIVO + CT failed to improve OS in 1L
HER2-negative advanced G/GEJ cancer.
“More toxicity. More treatment discontinuations. No survival gain.”
Worth noting: the comparator was CT alone, not a contemporary IO-CT.
Wait for bsAbs era.”

Arndt Vogel
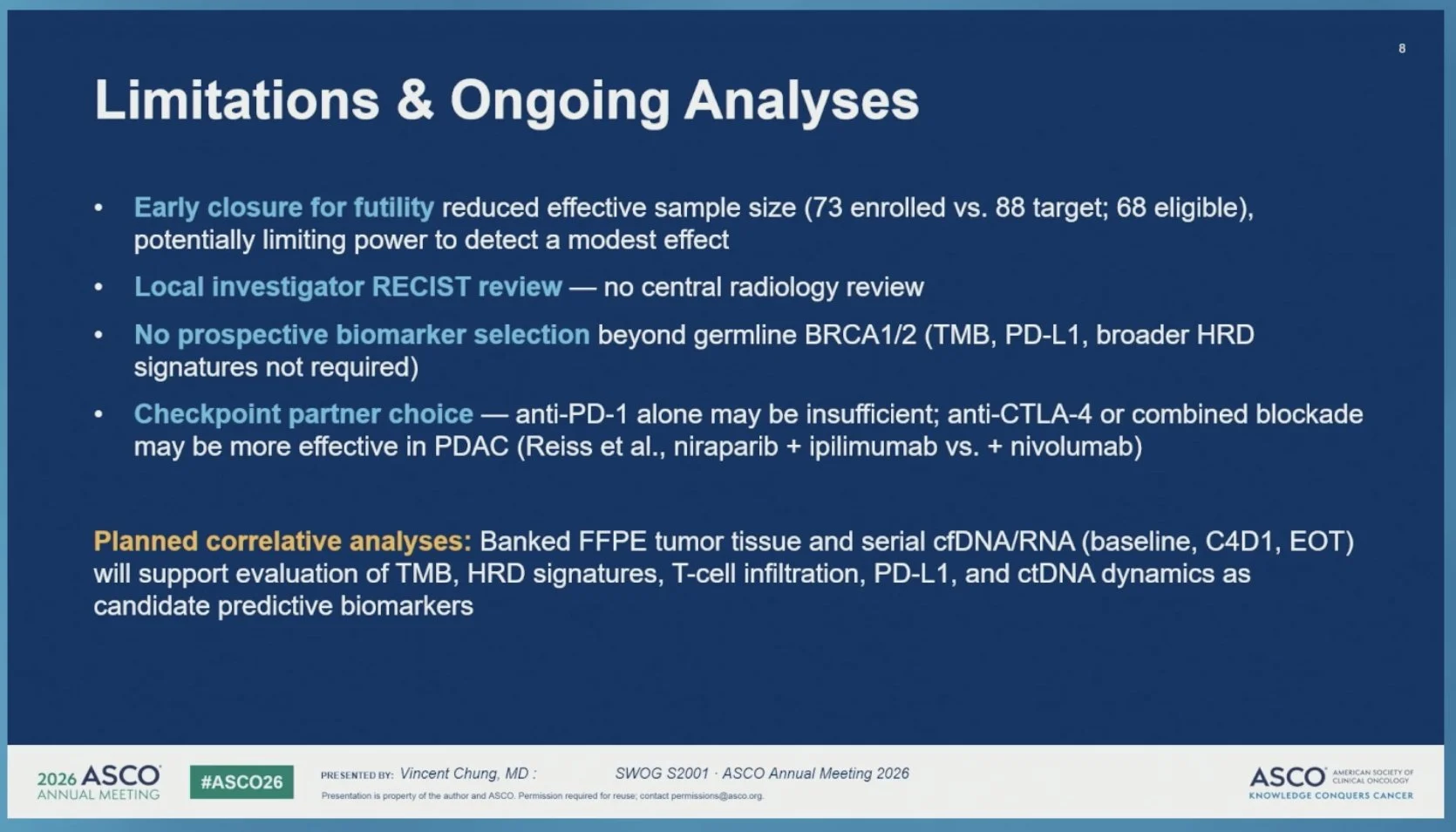
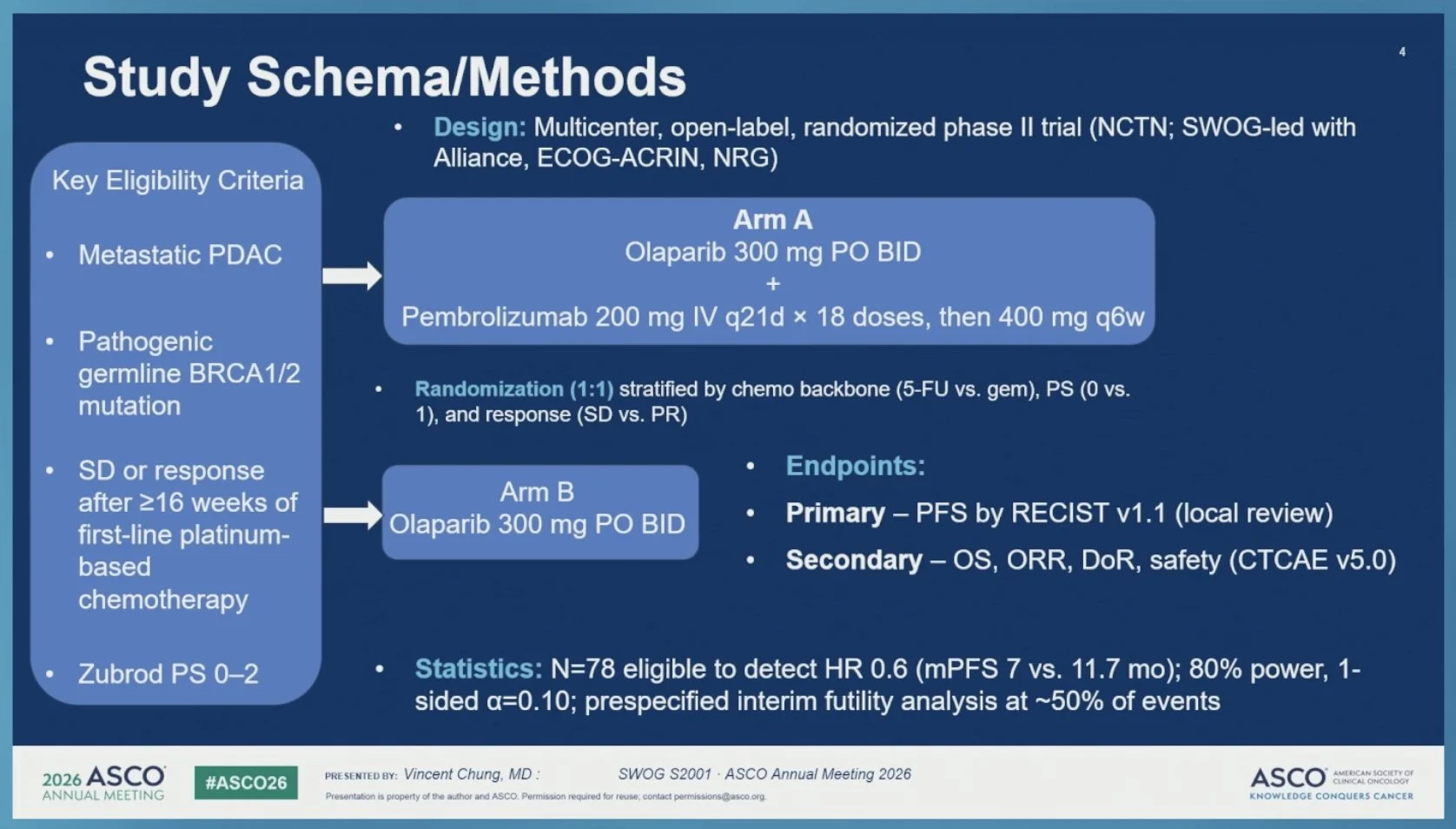
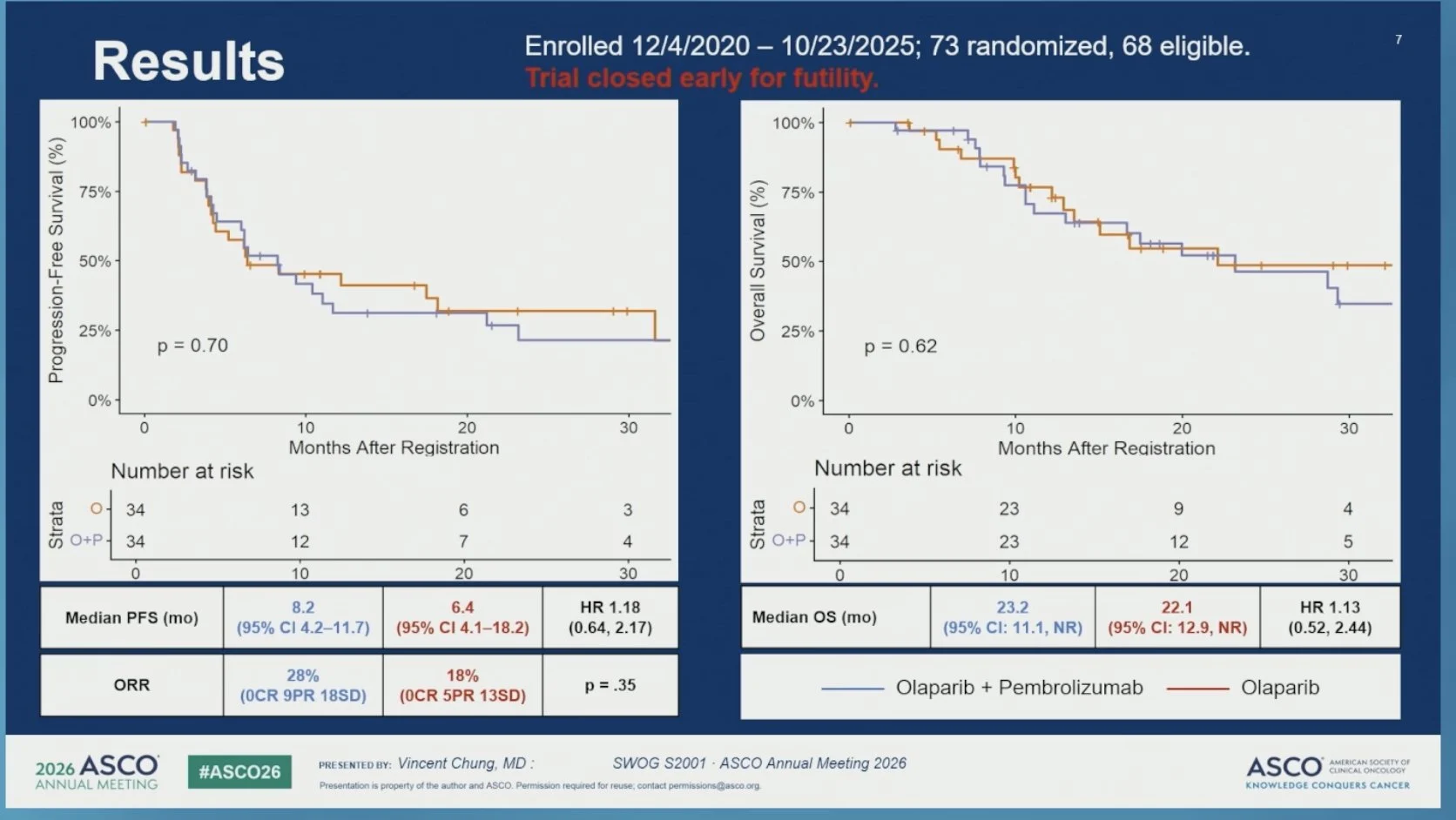
“Randomized phase II trial of olaparib and pembrolizumab vs olaparib alone as maintenance therapy in mPDAC with gBRCA1/2 mutations: SWOG S2001.
- Good rationale, but closed early due to futility
- Correlative analysis awaited
- Olaparib remains SOC.”

Read further on SWOG S2001, ATTRACTION-6, and CHALLENGE Trials.
Genitourinary Cancer
Tom Powles
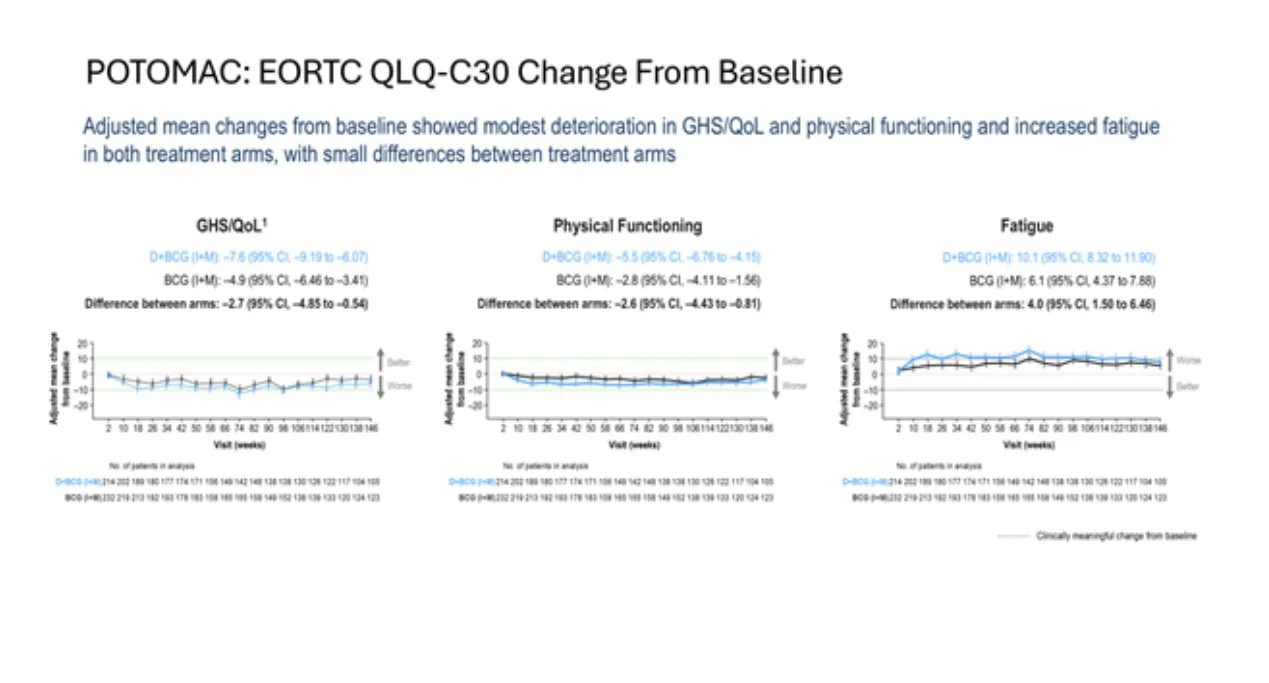
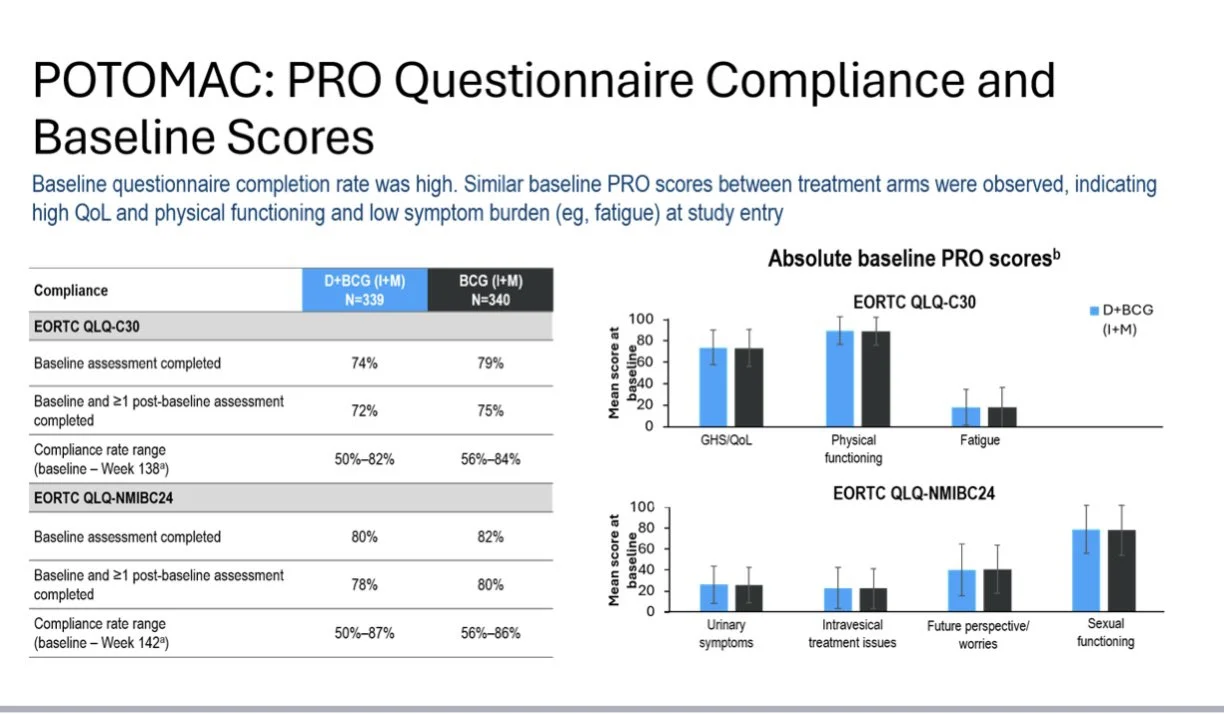
POTOMAC QOL: A year of durvalumab with BCG shows a delay in DFS and is FDA-approved, ASCO26.
Here, durvalumab appears to have little effect on QOL. We know ICIs have a ~10% rate of life-changing toxicity (~10% ), which affects QOL. New tools/methods are needed to unpick the details for patients.

Read also:
POTOMAC at ASCO 2026: Phase 3 Trial Reports 5-Year OS and PROs With Durvalumab Plus BCG in High-Risk NMIBC

Rashid K. Sayyid
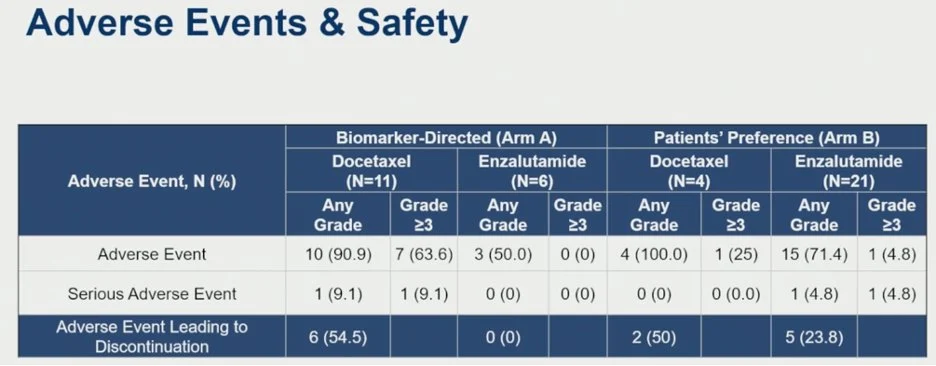
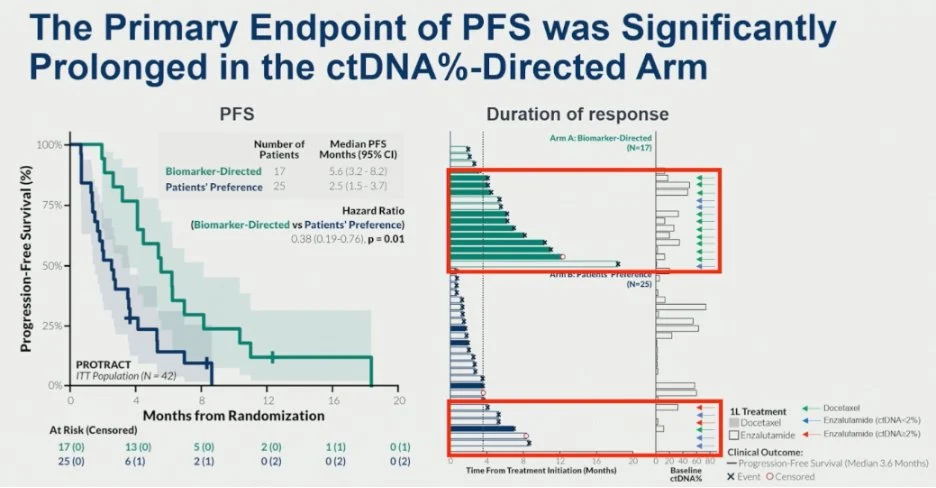
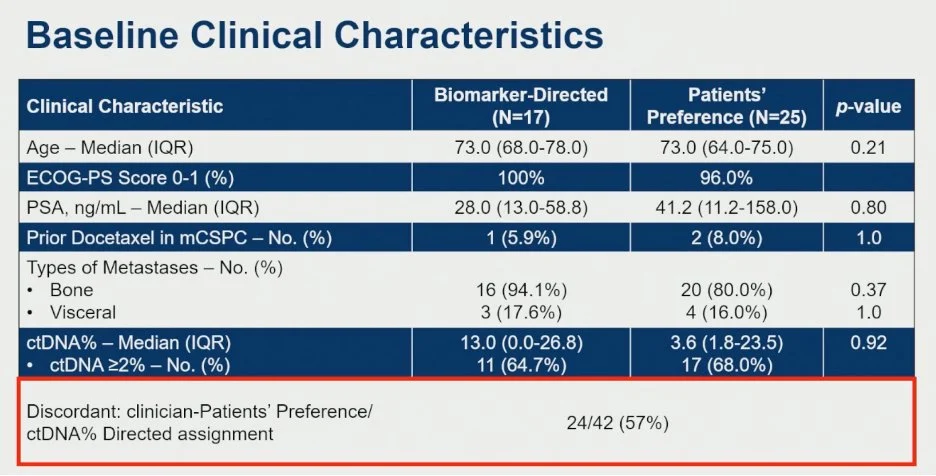
“PROTRACT: Ph 2 ctDNA-guided therapy vs physician/patient choice in mCRPC progressing after AAP (prior doce 6-8% in mCSPC)
Biomarker arm: ctDNA%≥2 Doce; <2% Enza (crossover allowed)
- Trial stopped early: n=42 enrolled of planned 100 due to poor enrolment
- PFS: 5.6 vs 2.5 mo (HR 0.38; p=0.01)
- PSA50 response: 53% vs 28%
- OS: 46.3 vs 15.3 mo (HR 0.39; p=0.04)
No new safety signals; toxicity consistent with docetaxel and enzalutamide.”

María Natalia Gandur Quiroga
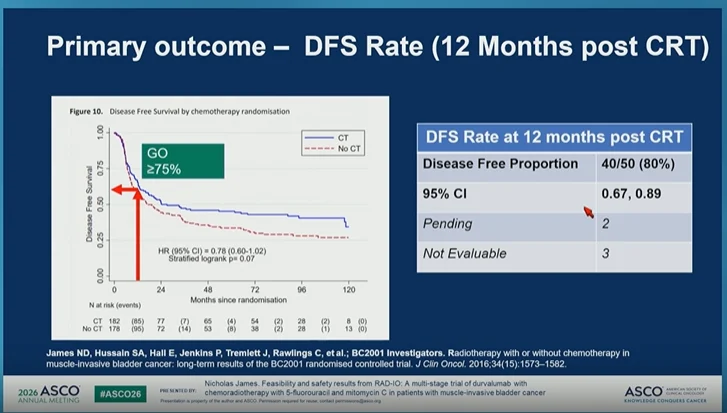
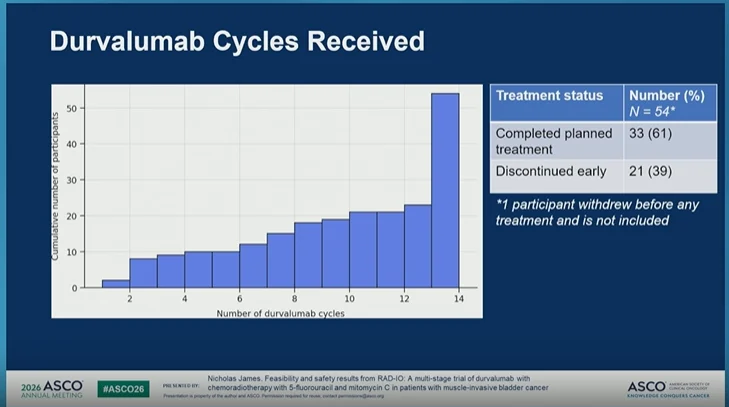
“ASCO26 Abstract 4504 | RAD-IO
Durvalumab + chemoradiotherapy in muscle-invasive bladder cancer Presented by Nicholas D. James
Bladder preservation in MIBC remains one of the most important curative-intent questions in GU oncology.
The key question here:
Can immune checkpoint inhibition be safely integrated with standard chemoradiotherapy?
RAD-IO evaluated durvalumab with bladder-directed chemoradiotherapy using 5-FU + mitomycin C in patients with muscle-invasive bladder cancer.
Study design
Stage 2 efficacy cohort:
- T2 N0–2 M0 MIBC
- CRT + durvalumab
- Single-arm phase II design
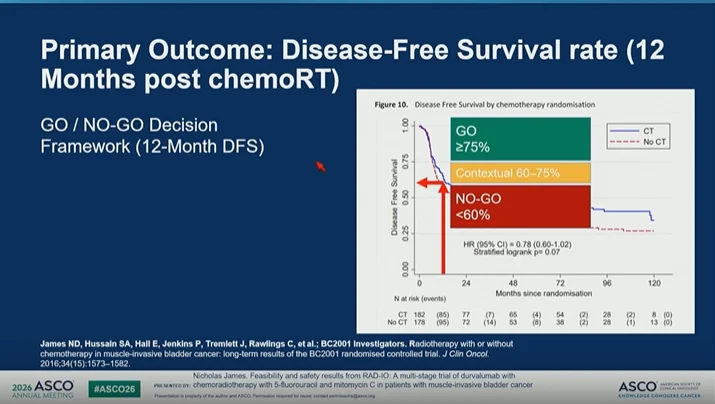
- Primary endpoint: 12-month disease-free survival
- 12-month DFS used as a surrogate for longer-term outcome
The trial used a clear GO / NO-GO framework:
- GO: DFS ≥75%
- Contextual: 60–75%
- NO-GO: <60%
Feasibility
Among 54 participants who started treatment:
- 100% received full radiotherapy: 55 Gy in 20 fractions
- 0 stopped radiotherapy early
- 87% had no RT extension or delay
- 100% received mitomycin C
- 100% received week 1 5-FU
- 78% received week 4 5-FU
- 61% completed planned durvalumab
- 39% discontinued durvalumab early
So, delivery of CRT was highly feasible, while immunotherapy completion was more challenging.
Primary outcome
At 12 months post-CRT:
- DFS rate: 80%
- 40/50 disease-free
- 95% CI: 0.67–0.89
This crossed the prespecified GO threshold.
Secondary outcome PFS was consistent:
- No event: 83.6%
- Distant metastasis: 9.1%
- Local disease: 7.3%
My take:
RAD-IO provides an encouraging signal that durvalumab can be integrated with bladder-preserving chemoradiotherapy in MIBC.
But this is not yet practice-changing. Important caveats:
- single-arm phase II design
- 12-month endpoint
- no randomized comparator
- durability and late toxicity remain critical
- completion of durvalumab was imperfect
Still, this is a very relevant direction.
“In an era where systemic therapy is becoming increasingly active in urothelial cancer, bladder preservation strategies need to evolve too. The next question is not simply whether CRT works.”
It is:
- Which patients are best suited for bladder preservation?
- Can immunotherapy improve the cure without compromising safety?
- How should we integrate systemic therapy, radiation, surgery, and patient preference?
For MIBC, the future may be a more personalized curative-intent pathway – not one-size-fits-all cystectomy versus CRT.”

Read more on the RAD-IO Trial:
RAD-IO at ASCO 2026: Durvalumab Plus Chemoradiotherapy in Muscle-Invasive Bladder Cancer

UChicagoCancerCenter
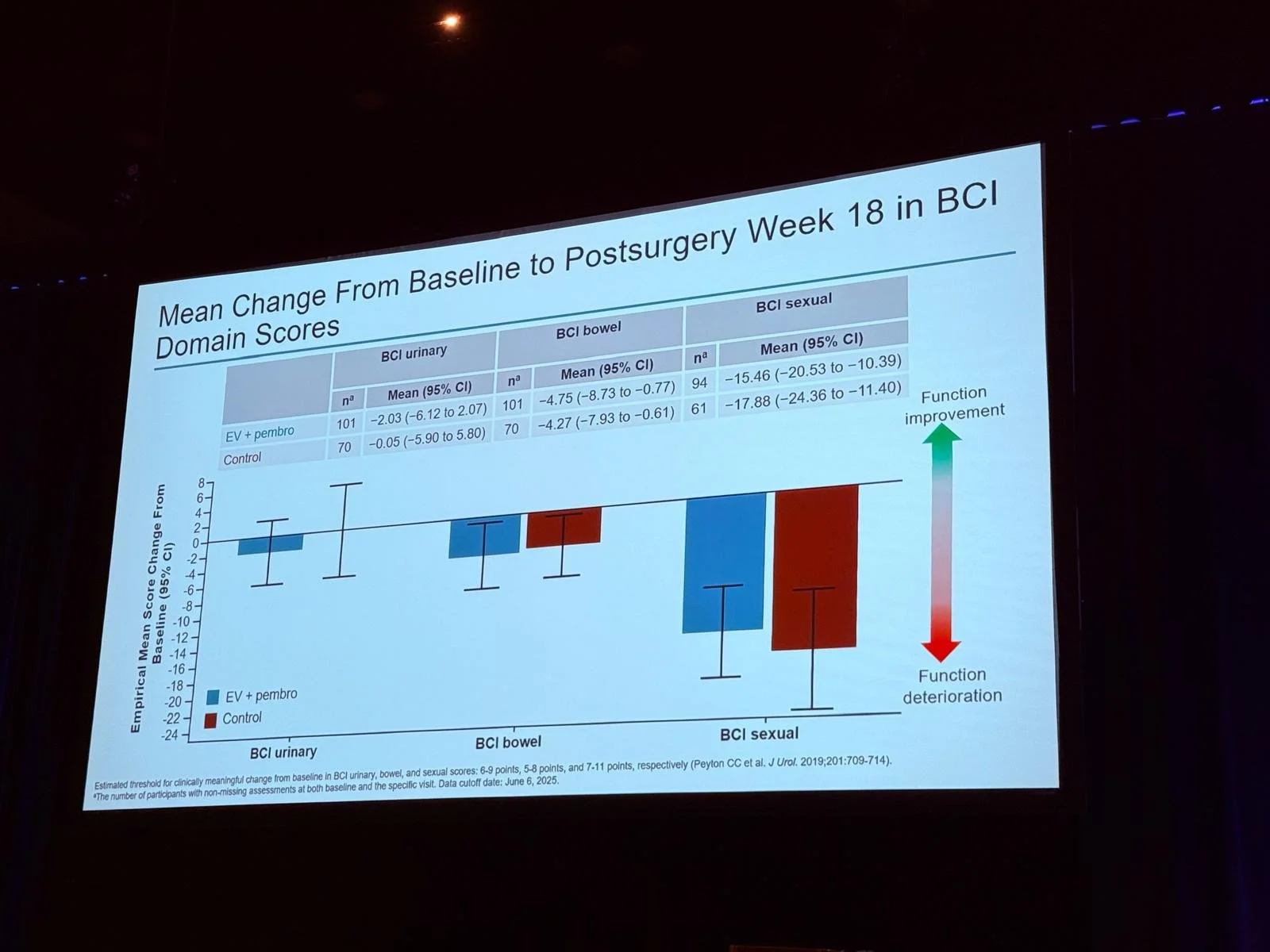
“Day 2 at ASCO26:
Peter O’Donnell presents results from the phase 3 KEYNOTE-905 study, reporting positive outcomes with enfortumab vedotin plus pembrolizumab in patients with muscle-invasive bladder cancer.”

Conquer Cancer
At the ASCO 2026 Annual Meeting, Conquer Cancer, the ASCO Foundation, officially awarded more than $11.7 million in vital funding to accelerate promising cancer research and support the next generation of oncology pioneers. These prestigious grants span multiple competitive categories, including the Young Investigator Awards (YIAs), Advanced Clinical Research Awards (ACRA), Long-term International Fellowships (LIFe), and the Women Who Conquer Cancer Mentorship Awards. Alongside these grants, the highly competitive Merit Awards were presented to outstanding oncology fellows, residents, and medical students who authored top-tier, high-scoring research abstracts. To celebrate the incredible human and scientific impact on the floor this year, here are some of the standout highlights and moments from the inspiring recipients who are shaping the future of global oncology:
Yelena Janjigian
“Look at these shining faces!
The energy, enthusiasm, and drive of our Young Investigator Award Conquer Cancer, the ASCO Foundation recipients, never cease to amaze me. Balancing the demands of fellowship training, research, and my busy GI Onc clinic can’t be easy, yet these two make it look effortless.
In just their first year of dedicated research time, Jeremy Tchack and Charlton Tsai have already brought two innovative investigator-initiated studies to our gastric and esophagus cancer patients at Memorial Sloan Kettering Cancer Center. That kind of early experience creates a trajectory for success that will benefit patients and the field for years to come.”
“I couldn’t be more proud of my mentees and all they have accomplished. Congratulations on this well-deserved recognition. The future is bright”

Ohio State University Comprehensive Cancer Center-James Cancer Hospital and Solove Research Institute
“It’s a great day to honor Ohio State oncology excellence at ASCO26, where we’re celebrating Mateus Trinconi Cunha (Young Investigator Award) and Lingbin Meng (Career Development Award), who were each recognized for their research by Conquer Cancer, the ASCO Foundation.
The prestigious awards will help these talented scientists continue to break new ground in geriatric oncology and immunotherapy evasion.”

Emir Sokolović
“Honored to receive the 2026 International Development and Education Award (IDEA) from ASCO and Conquer Cancer at the 62nd ASCO Annual Meeting in Chicago. The award recognizes commitment to advancing cancer research, education, and international collaboration to improve cancer care worldwide.
Grateful to my family and my team at the Clinic of Oncology, Clinical Center University of Sarajevo, whose support and dedication make achievements like this possible.”

Conquer Cancer
“This week at ASCO26, Dr. Brian Wolpin and Dr. Mark Dickson will demonstrate why bridging the funding gap for early-career researchers is critical.
Both investigators received Conquer Cancer funding early in their journeys, providing the “runway” necessary to develop the Phase 3 clinical trials they will present this week on the ASCO Plenary Stage.”
Explore the pattern of predictable science

Erika Ruiz-Garcia
“My team and I won the International Innovation Grant Award from Conquer Cancer 2026!”
“This is truly the result of great teamwork.”

Gebrekirstos Hagos
“I am delighted to share that I have been honored with the prestigious Conquer Cancer Award. As part of this award”
- I received an International Development and Education Award in Palliative Care (IDEA-PC).
- Attend the 2026 ASCO Annual Meeting in Chicago, which brings together more than 40,000 oncology professionals from around the world.
- Clinical Unit Visit at the Massachusetts General Hospital (MGH) in Boston.
I want to thank the American Society of Clinical Oncology (ASCO) for this incredible opportunity, MGH and my mentor, Dr. Jennifer Shin, for hosting me.
Thank you all my mentors.”

Yan Leyfman
“I’m deeply honored and humbled to receive the 2026 ASCO Conquer Cancer Merit Award and to represent our work at ASCO Breakthrough 2026 in Singapore.”
“But this recognition is not mine alone. It reflects the countless hours, sacrifices, resilience, and belief of the entire MedNews Week family. Behind every milestone are people who chose to build something bigger than themselves – a mission centered on connecting medicine globally through education, collaboration, and innovation.
As MedNews Week celebrates its 4.5-year anniversary, I’m reminded that none of this would have been possible without the extraordinary physicians, researchers, scientists, and global leaders who believed in our vision early on and entrusted us with their voices and stories. To every speaker who has contributed their time, expertise, and passion to educate our global audience – thank you. You helped shape MedNews Week into the platform and community it is today.
Success never happens in a vacuum. I’m incredibly grateful to work alongside a team that has become far more than colleagues over the years. MedNews Week was built through shared vision, trust, and the dedication of individuals across the world committed to advancing global medical education.
I want to especially thank my mentors, Dr. Chandler Park and Dr. Arturo Loaiza-Bonilla, whose guidance, belief, and unwavering support continuously challenged me to dream bigger, work harder, and never stop growing. Your mentorship has shaped not only my career, but the leader and physician I strive to become.
I’m also grateful for the opportunity to collaborate with outstanding colleagues such as Dr. Connor Yoast, whose future in oncology is exceptionally bright, and to the remarkable student and trainee leadership teams whose dedication behind the scenes continues to inspire me every day.
Finally, thank you to Dr. Julie Gralow, Dr. Chua, and the entire ASCO Breakthrough team for creating such a meaningful international platform dedicated to innovation, collaboration, and progress in oncology. I’m honored to be part of this year’s meeting and look forward to learning from and connecting with inspiring global leaders from around the world.
This is only the beginning. Looking forward to continuing to grow together.”

The Yvonne Awards 2026
The Yvonne Awards 2026 by OncoDaily celebrated impactful innovators and dedicated leaders in global oncology. These honors recognized outstanding contributions across prominent categories, including the Young Innovator Award, Global Oncology Leadership, and Mentorship and Advocacy. Highlighting the professionals pushing the boundaries of cancer care and equity worldwide, here are some of the standout moments and social media updates from this year’s award recipients.

Bishal Gyawali
“Exciting news! We are super proud to announce yesterday at the Yvonne Awards OncoDaily party, the partnership between BG Lab and OncoDaily for the Cancer Groundshot Virtual Fellow. We also announced our first BG Lab-Oncodaily virtual fellow, Dr. Elen Baloyan from Armenia.”
“Also on stage, our first virtual fellow, Syeda Mina sponsored by Agenus Inc. Our special thanks to OncoDaily and Agenus Inc for sponsoring the fellows and particularly to Gevorg Tamamyan for his enthusiastic support and collaboration. This is how we dismantle the boundaries in global oncology training and mentorship.
This is how we dismantle the boundaries in global oncology training and mentorship.”

Joanna Metzner-Sadurski
“Such an honor to receive the OncoDaily ASCO 2026 Yvonne Award “Oncology Oscars”. Having the award presented by Susan Dent made the moment even more special.
“This recognition is not just for me – it is a recognition of the importance of CommunityOncology and the physicians, nurses, researchers, navigators, and staff who care for patients every day, often far from major academic centers.”
It is also a recognition of the importance of health literacy. Oncology101.org The best treatments in the world cannot help patients if they do not understand their diagnosis, treatment options, potential side effects, or clinical trial opportunities.
Community oncology matters. Rural oncology matters.
I am grateful to the leaders who helped build and champion this movement, including Wade Swenson , Jasmine Kamboj, MD, FASCO and Ruiling Yuan, MD whose dedication to advocacy, education, and patient care continues to inspire so many of us.
While community oncologists represent only a small percentage of the oncology workforce, they care for the vast majority of patients in rural and underserved communities. Their work ensures that patients can receive high-quality cancer care close to home, surrounded by their families and support systems.
Thank you to OncoDaily, American Society of Clinical Oncology (ASCO), my colleagues, mentors, and most importantly my patients. This award strengthens my commitment to continue advocating for health literacy, clinical trial access, and equitable cancer care for all.”

Emmanuella-Faith Amoako
“This award may bear my name, but it belongs to every child who taught us what courage looks like.”
“Every parent who refused to give up, every nurse who stayed late, every colleague who believed children in Africa deserve the same chance at survival as children anywhere else, to mentors who have held my hands, To my family and friends that pushed me beyond any boundaries!”

Mohammad Hojouj
I am deeply honored and grateful to receive the Yvonne Award for Humanitarian Work 2026 from OncoDaily.
“While we celebrate the remarkable progress of science and medicine, this recognition reflects another reality of our profession – caring for patients under the most challenging and uncertain conditions.”
I accept this award with humility, on behalf of my colleagues and friends who continue to serve patients with courage, resilience, and compassion, especially those working in areas affected by conflict. Their dedication truly defines the spirit of this award.
My sincere thanks to the OncoDaily team for this meaningful recognition.
We will continue to stand, to serve, and to care.

As Chicago clears out, the oncology community leaves with a unified mission: to turn these major data updates into real-world victories for patients everywhere.
You can also read:
25 Posts Not To Miss From ASCO 2026 Day 4

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}