


At the 2026 ASCO Annual Meeting, Darren R. Feldman, MD, from Memorial Sloan Kettering Cancer Center and Weill Cornell Medical College, presented final results from a CaboNivo phase 2 trial evaluating cabozantinib plus nivolumab in patients with non–clear cell renal cell carcinoma.
Non–clear cell RCC accounts for approximately 25% of metastatic kidney tumors and includes multiple distinct tumor histologies. Compared with clear cell RCC, patients with non–clear cell RCC have historically had inferior outcomes, particularly with single-agent VEGFR tyrosine kinase inhibitors.
Cabozantinib plus nivolumab previously improved objective response rate, progression-free survival, and overall survival compared with sunitinib in patients with clear cell RCC in the phase 3 CheckMate 9ER trial. This phase 2 study evaluated the combination in patients with untreated and previously treated non–clear cell RCC subtypes.
How Do Cabozantinib and Nivolumab Work?
Cabozantinib is a tyrosine kinase inhibitor. Cells use tyrosine kinases as signaling switches that help send instructions to grow, divide, and form new blood vessels. In some cancers, these signals can become overactive, allowing tumors to grow and build their own blood supply. Cabozantinib works by blocking several of these overactive switches, including VEGFR, MET, and AXL. By doing this, it may help slow cancer cell growth, reduce the tumor’s blood supply, and limit cancer spread.
Nivolumab is an IgG4 monoclonal antibody that binds to PD-1 receptors on T cells. PD-1 normally helps regulate immune responses. When PD-1 binds to PD-L1 or PD-L2, it can reduce T-cell activity. In cancer, tumor cells or immune cells in the tumor microenvironment may use this pathway to avoid immune detection. By blocking PD-1, nivolumab helps release immune cells from this suppression, allowing them to recognize and fight tumor cells.

Read more about Cabozantinib on OncoDaily.
Study Design
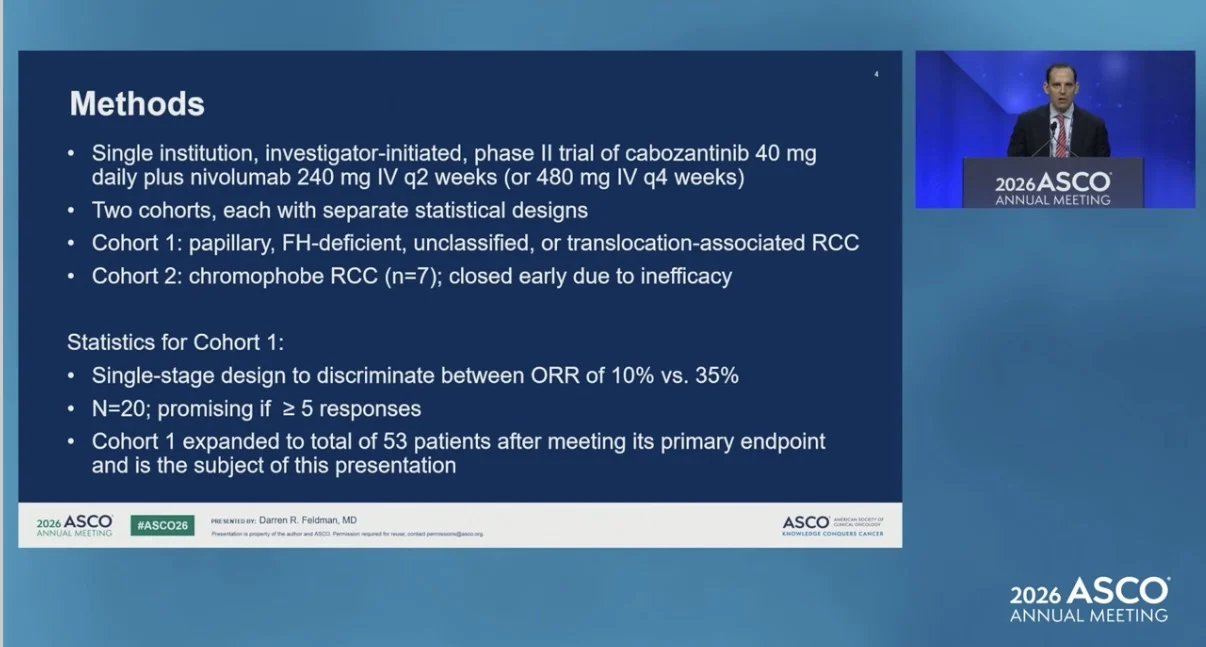
This was a single-institution, investigator-initiated phase 2 trial. Patients received cabozantinib 40 mg daily plus nivolumab 240 mg intravenously every 2 weeks or 480 mg intravenously every 4 weeks.
The study included two cohorts with separate statistical designs. Cohort 1 included patients with papillary, FH-deficient, unclassified, or translocation-associated RCC. Cohort 2 included patients with chromophobe RCC and was closed early due to inefficacy.
For Cohort 1, the study used a single-stage design to distinguish between an objective response rate of 10% and 35%. The study was considered promising if at least 5 responses were observed among 20 patients. After meeting its primary endpoint, Cohort 1 was expanded to a total of 53 patients and was the focus of the final results presented.

Results
Cohort 1 included 53 patients.
Histologies included papillary RCC in 16 patients, unclassified RCC with papillary features in 16 patients, FH-deficient RCC in 8 patients, unclassified RCC in 8 patients, and translocation-associated RCC in 5 patients.
Among all patients in Cohort 1, PR/CR was observed in 23 patients, corresponding to 43%. Stable disease was observed in 27 patients, or 51%, and progressive disease in 3 patients, or 6%.
The PR/CR rate was 46% in the first-line group and 36% in the second-line group. Median progression-free survival was 11 months in all patients, 11 months in the first-line group, and 14 months in the second-line group.

By histology, PR/CR was observed in:
- 5 of 16 patients with papillary RCC
- 13 of 16 patients with unclassified RCC with papillary features
- 7 of 8 patients with FH-deficient RCC
- 4 of 8 patients with unclassified RCC
- 1 of 5 patients with translocation-associated RCC
Median progression-free survival was 11 months in papillary RCC, 10 months in unclassified RCC with papillary features, 16 months in FH-deficient RCC, 8 months in unclassified RCC, and 14 months in translocation-associated RCC.
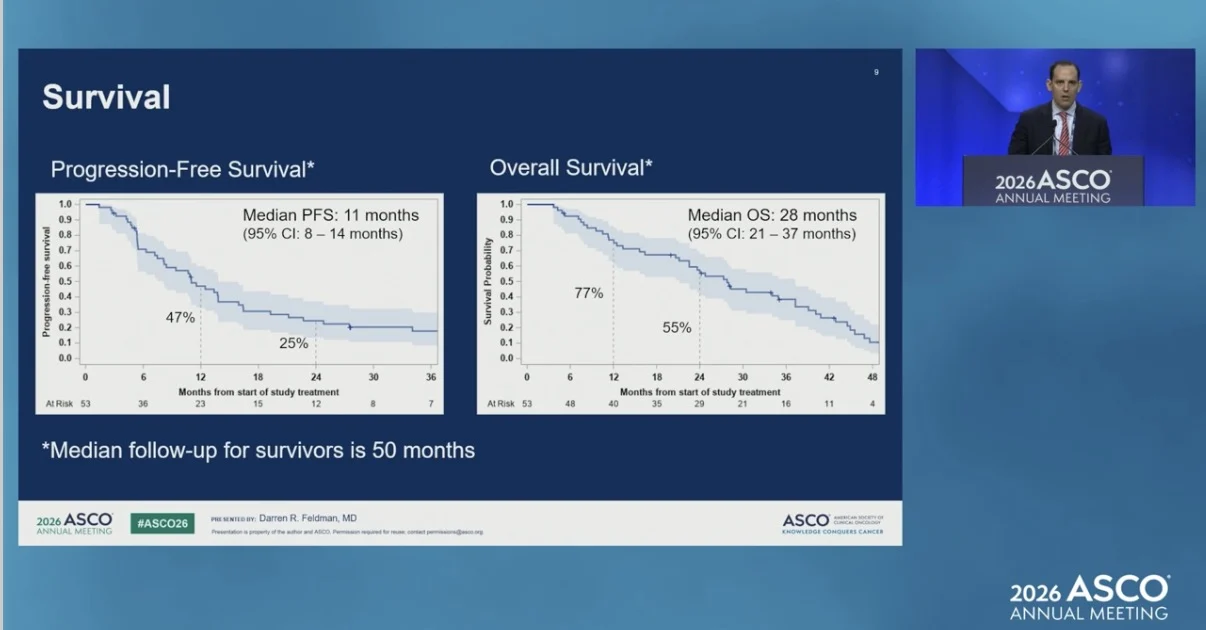
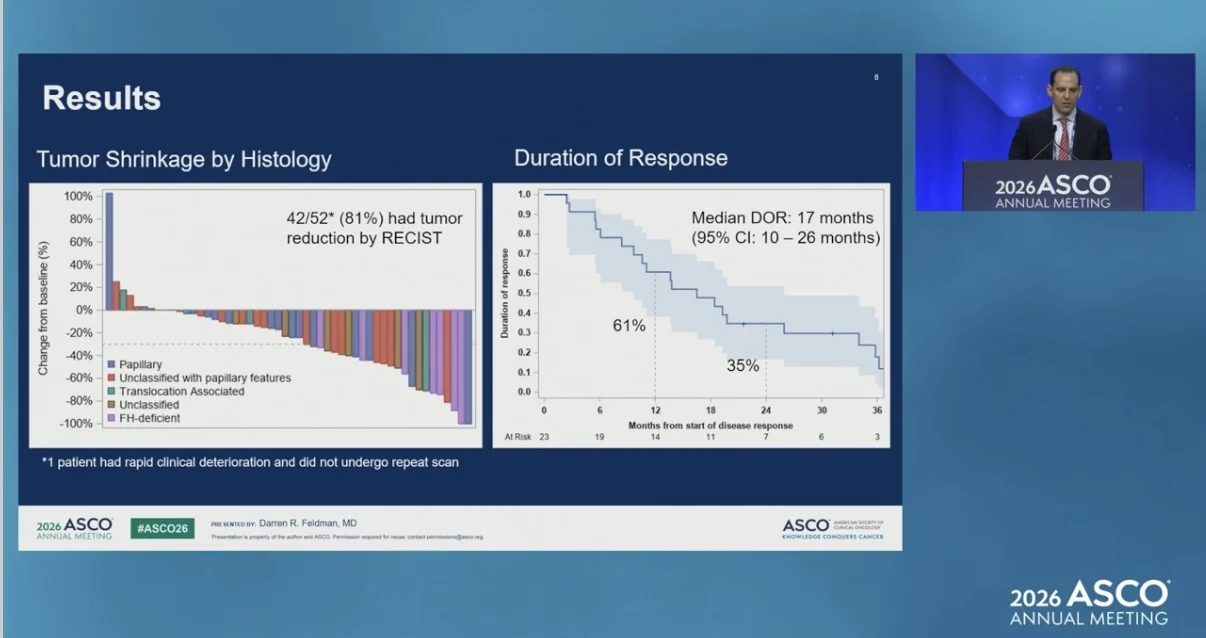
Tumor reduction by RECIST was observed in 42 of 52 evaluable patients. Median duration of response was 17 months. Median progression-free survival was 11 months, with a 95% confidence interval of 8 to 14 months. Median overall survival was 28 months, with a 95% confidence interval of 21 to 37 months. Median follow-up for survivors was 50 months.

Safety
The median treatment duration was 11.5 months. Treatment-emergent adverse events occurred in all 53 patients. Grade 3 or 4 treatment-emergent adverse events occurred in 36 patients, or 68%.
Treatment discontinuation due to adverse events occurred in 23 patients for cabozantinib, 22 patients for nivolumab, and 18 patients for both study drugs. The most common symptomatic adverse events reported in at least 35% of patients were fatigue, hand-foot skin reaction, diarrhea, constipation, pain, dry mouth, hypertension, nausea, oral mucositis, back pain, cough, and headache.
Selected laboratory adverse events included AST increase, ALT increase, platelet decrease, amylase increase, and lipase increase. Amylase and lipase increases were predominantly asymptomatic, and only one patient discontinued study drug for pancreatitis. Adverse events were as previously reported, with no new safety signals.
Conclusion
Final results with approximately 50 months of follow-up and additional patients reaffirmed antitumor activity for cabozantinib plus nivolumab in non–clear cell RCC.

Responses were observed in treatment-naive and previously treated patients, and across all histologies except chromophobe RCC. Seven of 8 patients with FH-deficient RCC achieved an objective response. Adverse events were as previously reported, with no new safety signals. The high response rate and safety profile support cabozantinib plus nivolumab as a treatment option for patients with non–clear cell RCC histologies.
You can find full information about CaboNivo on ASCO.

Read more about POTOMAC at ASCO 2026 on OncoDaily.
{kind=link}
{kind=link}
{kind=link}
{kind=link}