


Zacharoula Sidiropoulou, Senior Consultant Breast Surgical Oncologist at Hospital São Francisco Xavier, shared a post on LinkedIn:
“Day After SIOG Conference
Today I revisited with fresh perspective the excellent paper my former resident Mariana Beja published recently:
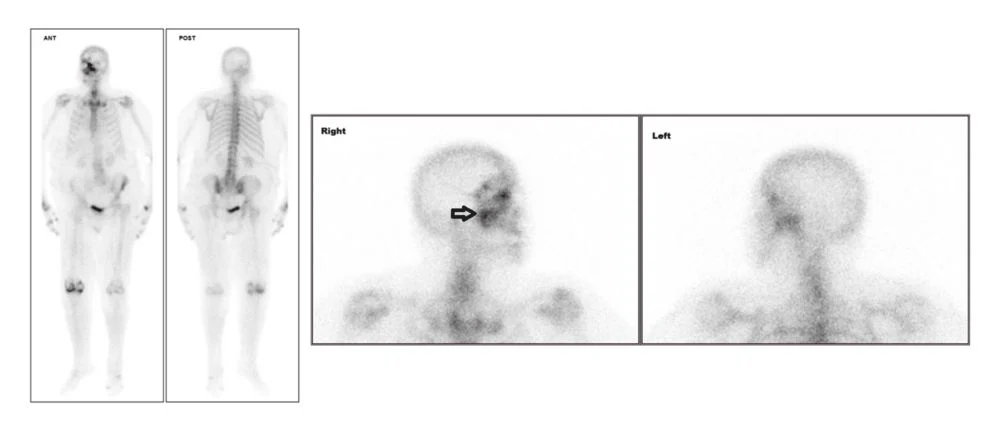
‘Beja M S, Marques J, Cardoso V S, et al. (November 18, 2025) Bone Metastases of Breast Cancer in the Skull Base: An Unusual Metastatic Spread.
An uncommon presentation (roughly 1% of bone-only metastatic cases) with rigorous investigation, appropriate imaging escalation, and multidisciplinary decision-making.
But this case teaches us something even more important, follow me
An 80+ year-old woman, previously autonomous with good performance status, began systemic treatment. Within 18 days, after severe pyelonephritis, she became bedridden. Two months later: brain metastases, then death.
Was this infection, treatment toxicity, aggressive biology, unrecognized frailty, or combined factors?
The Hidden Challenge:
The patient had: Congestive heart failure, Chronic kidney disease, atrial fibrillation, osteoporosis and likely polypharmacy, yet no Comprehensive Geriatric Assessment (CGA) was performed.
Standard Performance Status misses >50% of geriatric vulnerabilities. Functional reserve, cognition, nutrition, mobility, and social support are essential determinants of treatment tolerance.
What CGA Changes:
- Predicts toxicity more accurately than clinical judgment
- Reduces severe complications when used to adjust therapy
- Decreases emergency visits and hospitalizations
- Personalizes treatment by physiological, not chronological, age
CGA may not guarantee different outcomes, but it frequently mitigates rapid deterioration and aligns treatment with patient values.
Despite international recommendations, real-world implementation remains <30%.
We URGENTLY need geriatric-oncology programs to be recognized as high-value care.
As precision oncology advances, precision geriatrics must advance with it. Two patients with identical tumor biology may need entirely different strategies depending on: functional reserve, comorbidity burden, cognitive status, support structure, goals and values.
Treatment tailoring is not ageism—it is good medicine. Rapid decline is often predictable and potentially modifiable.
To Mariana Beja: thank you for this important case highlighting the complexity of cancer care in older adults.
To all of us: every older cancer patient deserves complete assessment, individualized treatment, and proactive supportive care.
This is not about doing less.
It is about doing what is right.”
Title: Bone Metastases of Breast Cancer in the Skull Base: An Unusual Metastatic Spread
Authors: Mariana S. Beja, Joana Marques, Vasco S. Cardoso, Zacharoula Sidiropoulou
Read the Full Article on Cureus

More posts featuring Zacharoula Sidiropoulou.
{kind=link}