


Vincent Rajkumar, Professor of Medicine at the Mayo Clinic in Rochester and Editor‑in‑Chief at Blood Cancer Journal, shared a post on X:
“Daratumumab is the standard of care for high risk smoldering myeloma, and should be considered as Option 1 (if available) after discussing pros and cons. It’s limited duration therapy that is approved by the FDA and in Europe. Observation alone is fraught with risk even in the best of centers.
Patients find it hard to get appointments to see doctors and specialists and get the right monitoring done to prevent end organ damage. So while that option is OK for certain patients, if that option is chosen please watch closely like the control arm of AQUILA (easier said than done) and as with dara, do so after discussing pros and cons. In my experience after doing many chart reviews and reviewing lots of lots of patient records, many physicians are super confident of being able to watch closely and prevent serious end organ damage but the reality is different.
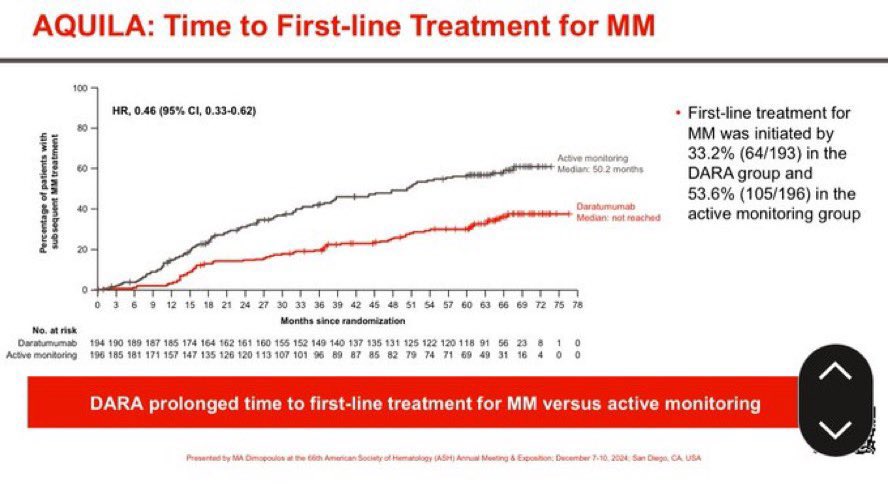
If patients with high risk smoldering myeloma are observed without therapy, ~40% will need full myeloma therapy by 3 years compared to only ~20% with daratumumab. At 6 years of follow up, among patients who are observed without therapy almost 60% will need full myeloma therapy compared to less than 40% who received dara, even though dara therapy stopped at year 3.
Given the complexity and seriousness of full myeloma therapy (quadruplet induction(, stem cell transplant if eligible, and indefinite maintenance), preventing or delaying this is in and if itself an important endpoint and these data should be discussed with the patient.
If progression to active myeloma occurs while on Dara, which may occur in a small proportion (~20%) of patients, almost all when the drug is being given once a month, I’d recommend standard myeloma therapy, including a quad like Dara VRd as induction. If progression occurs when patients are already off dara, it’s the same.
I’d recommend standard myeloma therapy if patients meet criteria for myeloma, including Dara VRd as induction. The induction regimen of choice is whatever is considered standard at the time. Myeloma therapy is rapidly evolving. For now it’s Dara VRd. 5 years from now it may be different.
Time to starting full myeloma therapy data discussed above are very important to consider and the data are shown below.
Full trial data in thread. Smoldering myeloma.
Linking to additional FAQ thread.”
You Can Also Read:
Results of AQUILA Trial: Daratumumab or Active Monitoring for High-Risk Smoldering Multiple Myeloma
FDA Approves Daratumumab and Hyaluronidase-fihj for High-Risk Smoldering Multiple Myeloma

Vincent Rajkumar: Historic and Paradigm Changing – The First Ever Treatment for High-Risk SMM

{kind=link}