


Olubukola Ayodele, Breast Cancer Lead at University Hospitals of Leicester NHS Trust, shared a post on LinkedIn:
“Day 1 ESMO Breast 2026 update.
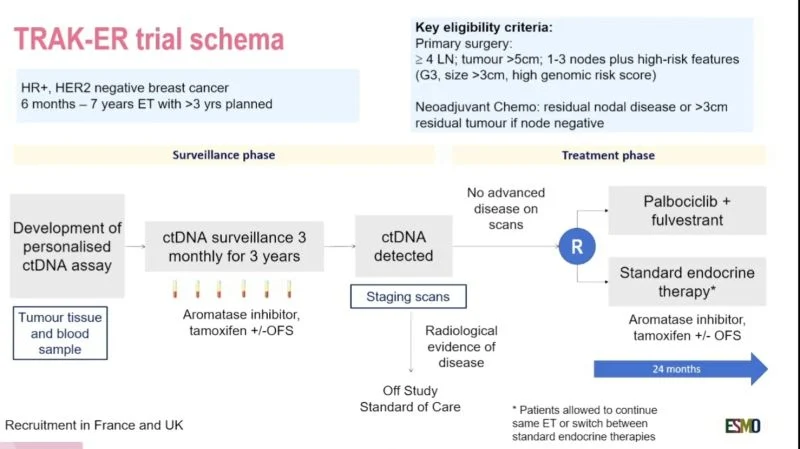
One of the most thought-provoking oral proffered papers for me today at ESMO Breast 2026 was the TRAK-ER study evaluating ctDNA surveillance in high-risk HR+/HER2-negative early breast cancer.
This is an important study exploring whether circulating tumour DNA (ctDNA) can identify molecular relapse earlier during adjuvant endocrine therapy. Precision oncology is evolving rapidly, and studies like this are shaping the future of cancer surveillance.
Key findings included:
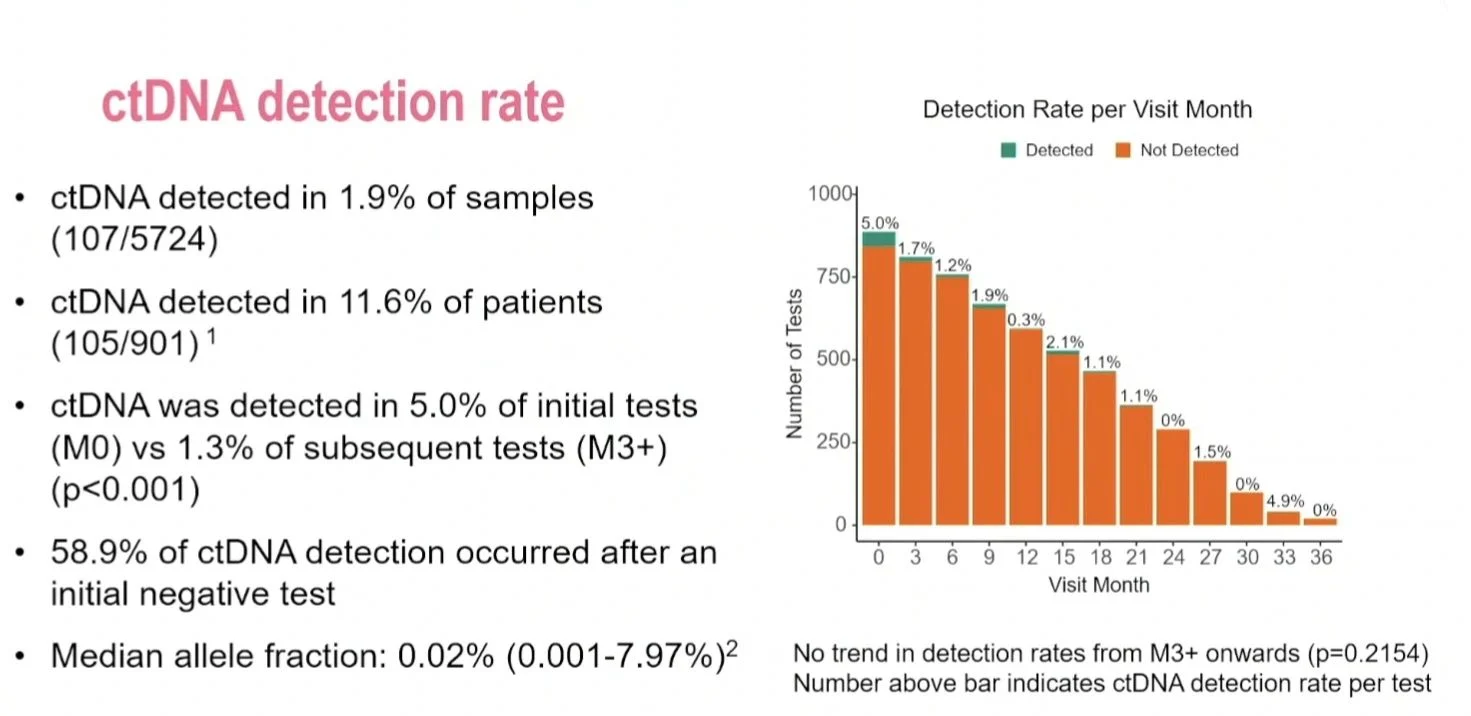
- ctDNA was detected in only 2.6% of surveillance tests
- 11.3% of patients had at least one positive ctDNA result
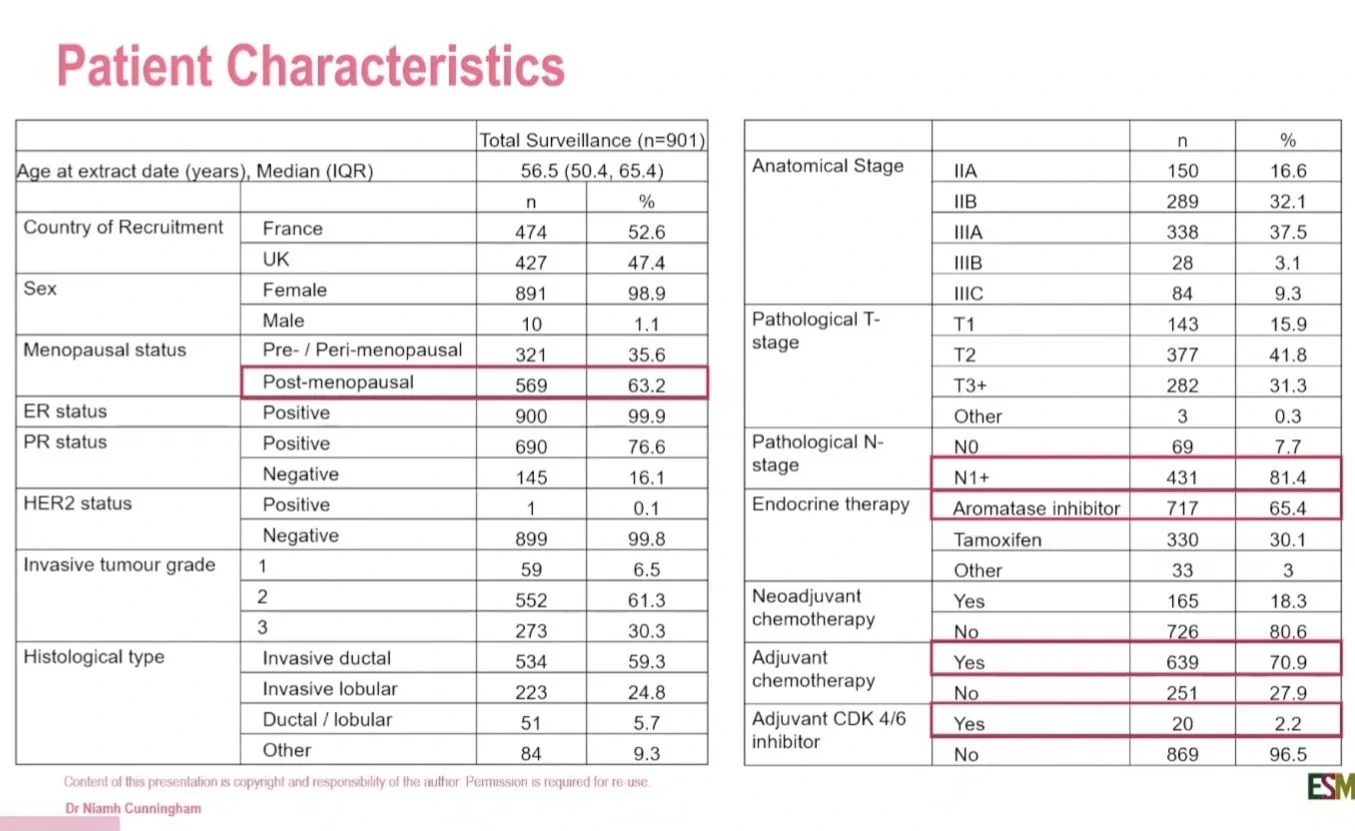
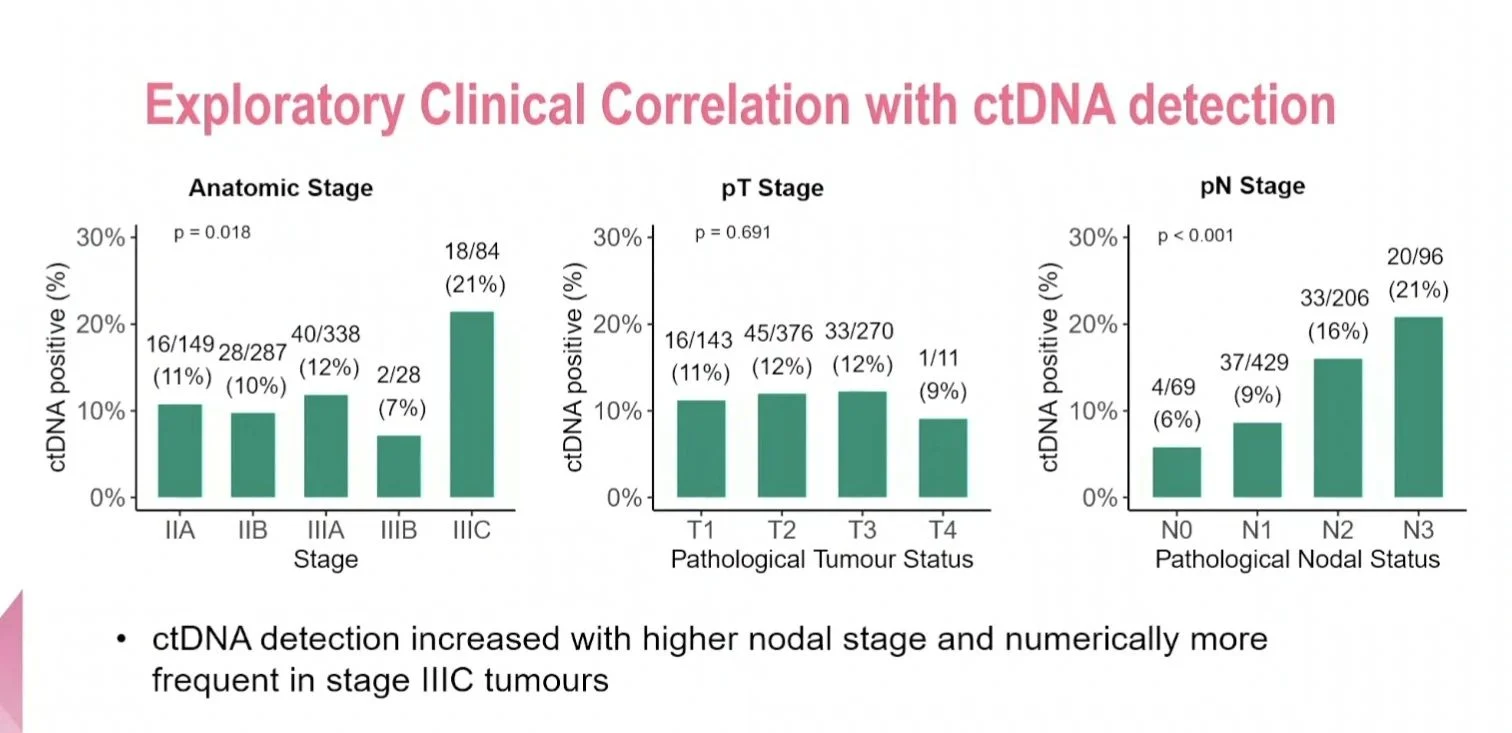
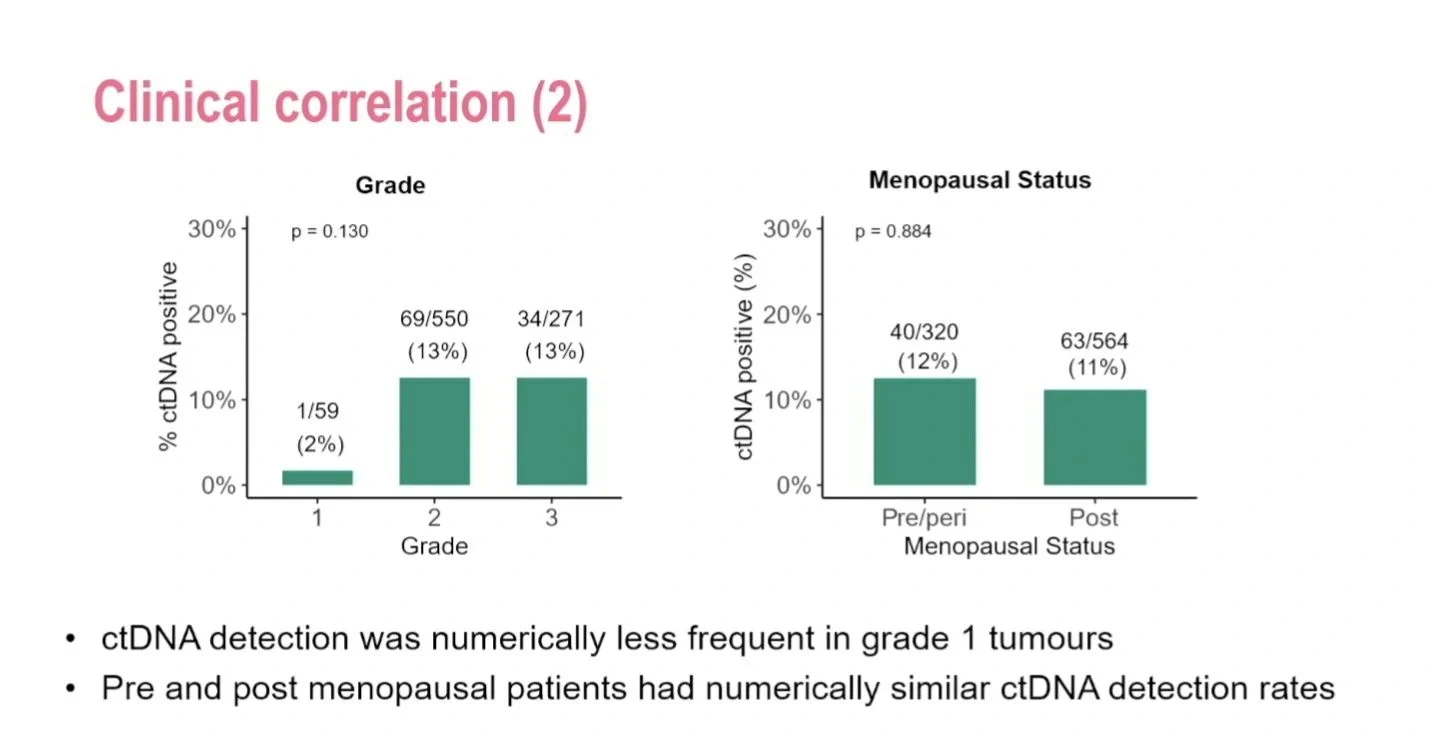
- Detection was more common in higher nodal burden and stage IIIc disease
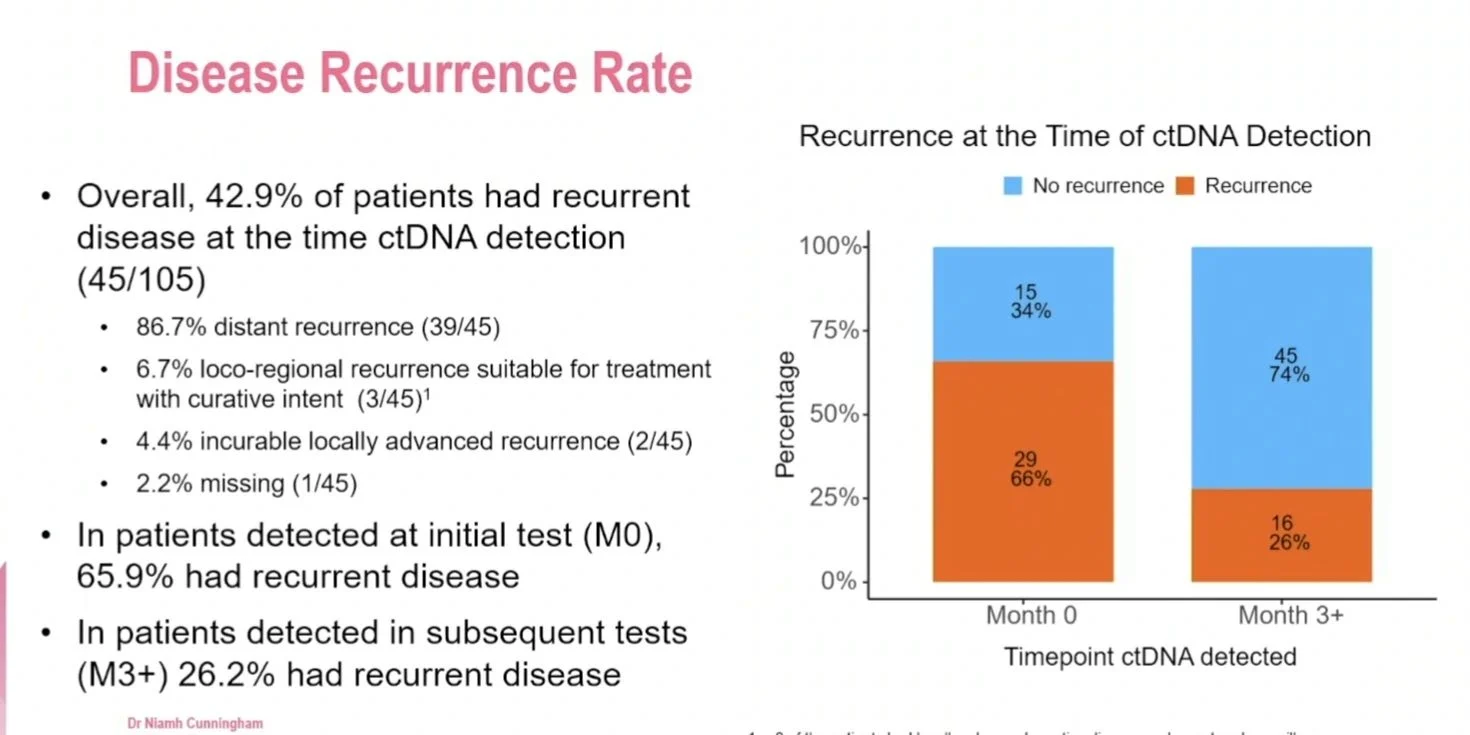
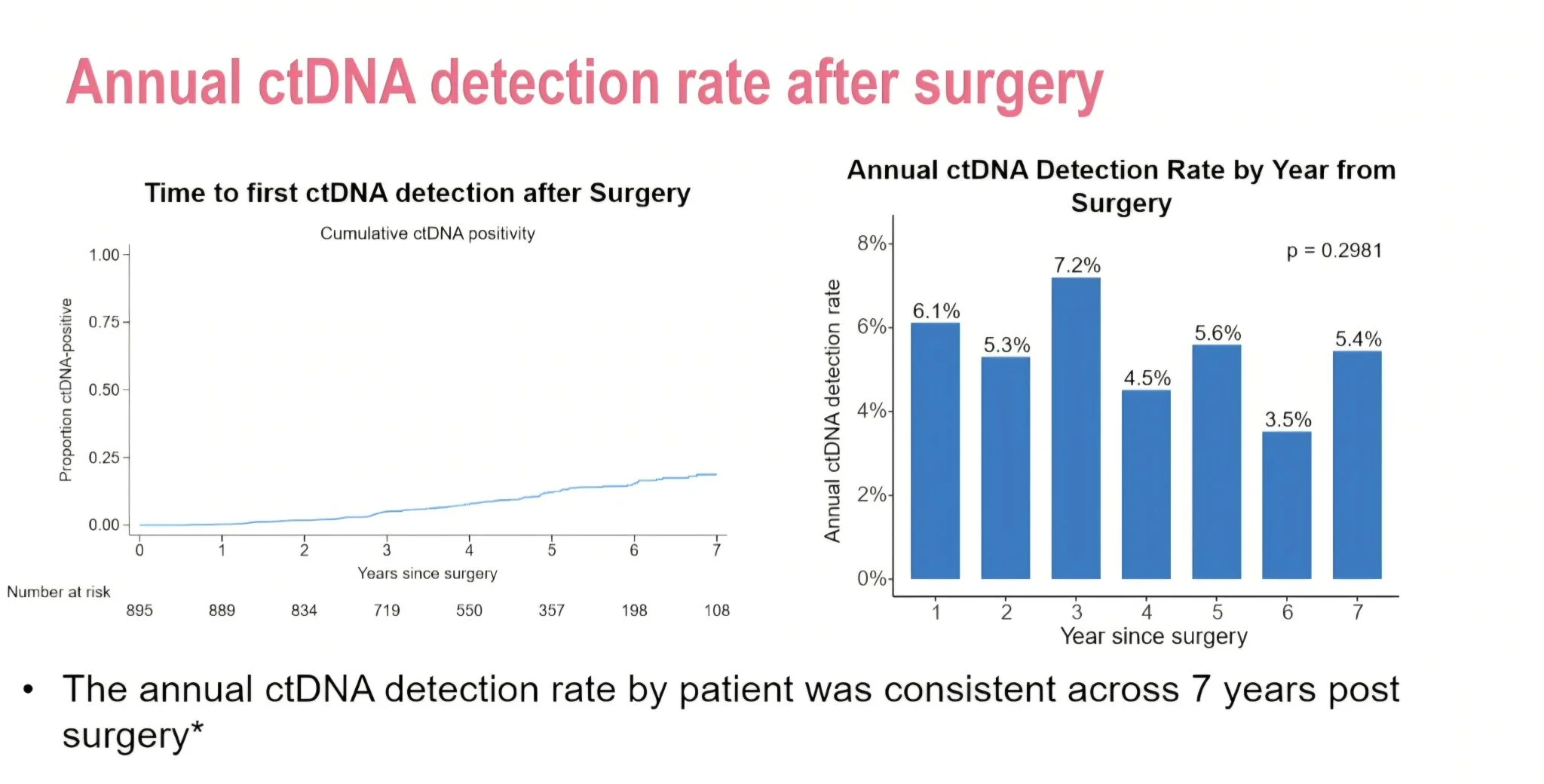
- Detection rates were highest at the first surveillance time point
- Almost 85% of patients with positive ctDNA already had clinically detectable metastatic disease
This raises important questions for oncology.
Patients underwent blood testing every 3 months over several years. While ctDNA surveillance is scientifically exciting, we cannot ignore the psychological burden this creates. For many patients, every blood test becomes another cycle of anxiety and uncertainty.
There is also the financial reality. Tumour-informed ctDNA assays remain extremely expensive, especially when compared with standard imaging such as CT scans.
As precision oncology advances, we risk widening existing inequalities in cancer care. The issue is not whether ctDNA technology is impressive. It is. The question is whether healthcare systems globally can sustainably deliver this kind of surveillance without deepening inequity.
What happens to lower-resource healthcare systems already struggling to provide equitable access to standard cancer treatment?
What happens when innovation becomes available only to those who can afford it?
We are entering a difficult space balancing precision oncology with financial toxicity and psychological demands on patients.
Another reflection for me is that health economics should be taught more explicitly in medical training. As clinicians, we are increasingly working in environments where cost, value, patient benefit, and equity are interconnected. Understanding the economics behind innovation is now part of responsible cancer care.
The future of oncology cannot simply be about what is technologically possible. It must also be about what is clinically meaningful, psychologically acceptable, economically sustainable, and globally equitable.”

Other articles featuring Olubukola Ayodele on OncoDaily.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}