


The 7-year update from the phase 3 CROWN study evaluating lorlatinib versus crizotinib as first-line treatment for advanced ALK+ non-small cell lung cancer continues to generate significant discussion among oncologists on X, with many sharing key takeaways, clinical perspectives, and reactions to the long-term results:
”CROWN 7-Year Update:
Lorlatinib in 1L ALK+ NSCLC: the longest PFS ever reported in advanced NSCLC keeps getting longer! ASCO26 Abstracts!
Presenter: Tony Mok
Key takeaways: ALK Positive
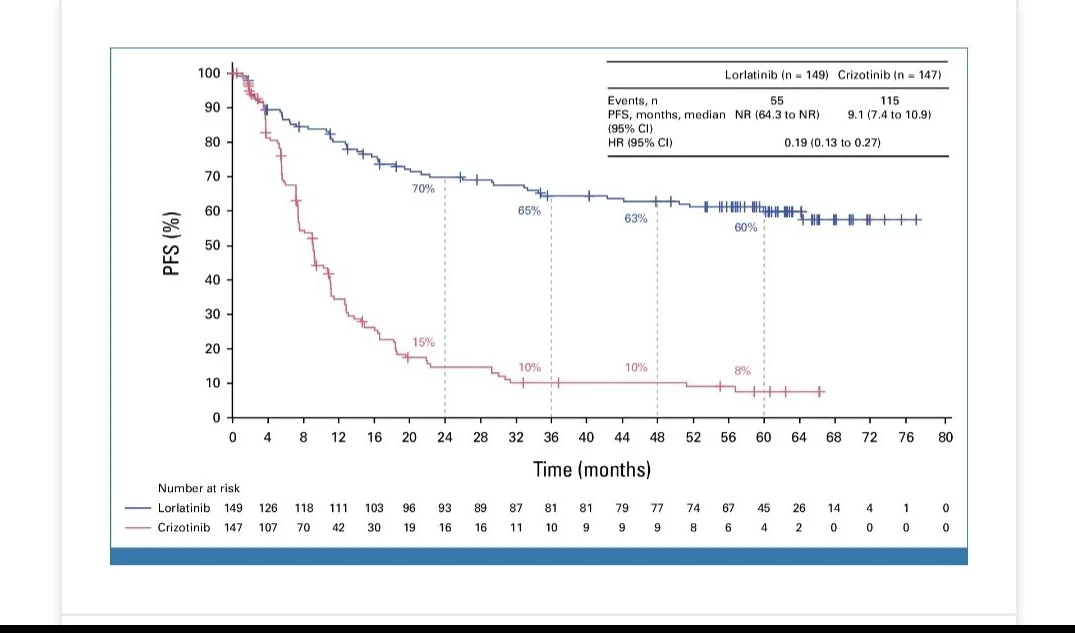
- Median PFS STILL not reached at 7 years.
- 7-yr PFS rate: 55% (lorlatinib) vs 3% (crizotinib), HR 0.19
- 44% of pts STILL on lorlatinib vs just 3% on crizotinib.
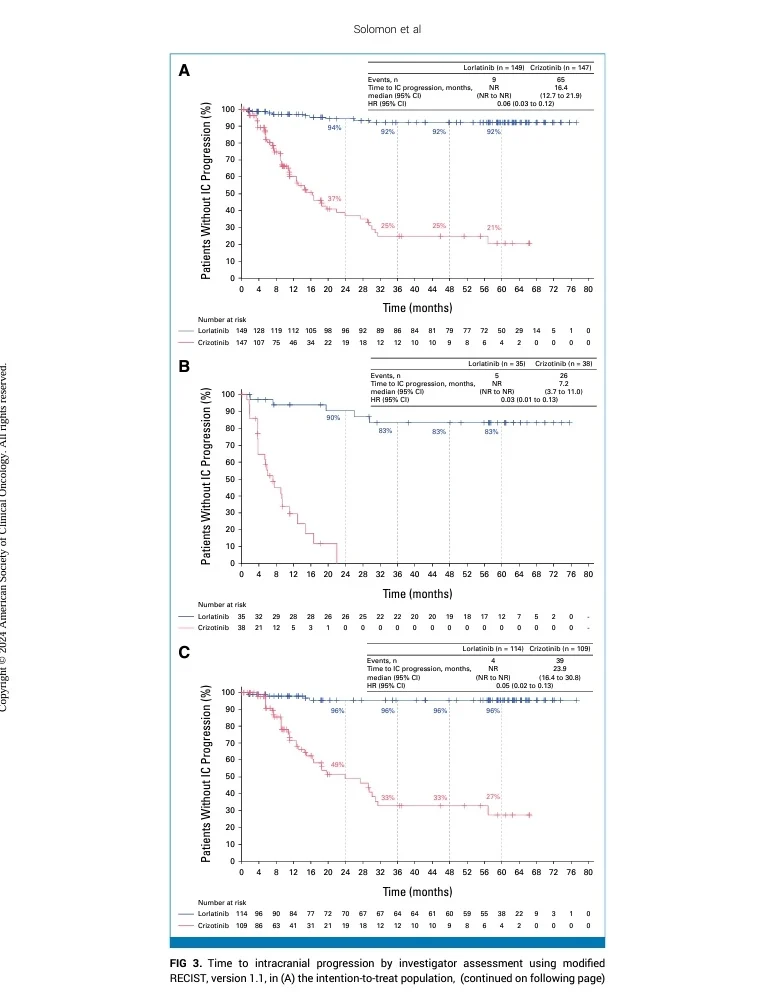
Complete intracranial control:
- ZERO new brain progression events after 30 months on lorlatinib
- HR for time to IC progression: 0.06
- This is arguably the most impressive CNS protection from any targeted therapy in solid tumors!
Durable ‘tail’ effect:
- If you’re event-free at 24 months on lorlatinib – 79% chance you’re still progression-free at year 7
- The KM curve is essentially flat after 2 years.
No new late toxicity signals:
- No new treatment-related discontinuations after 26 months
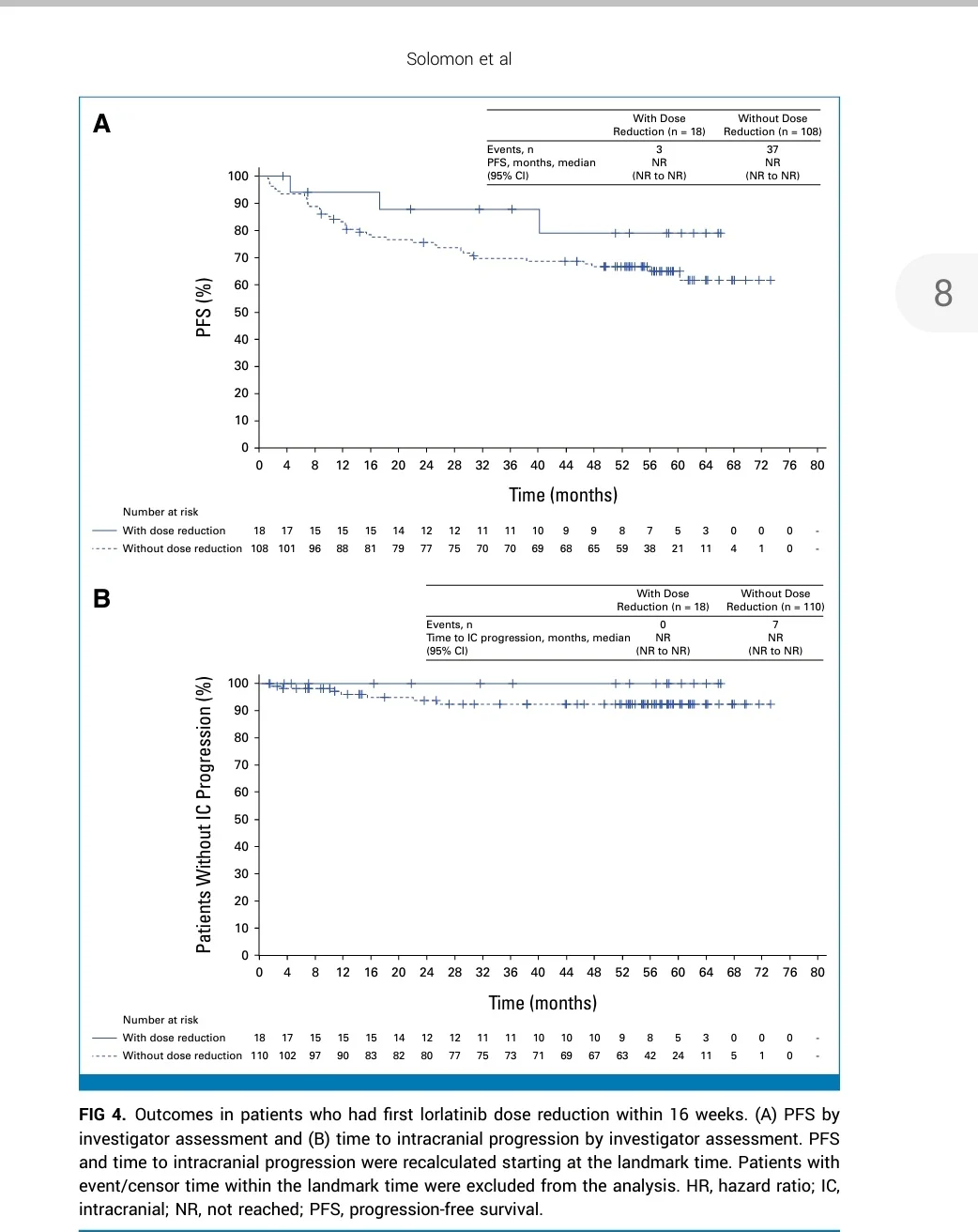
- Dose reductions (34%) did NOT compromise efficacy
- TRAE discontinuation: only 5% – lower than crizotinib (6%)
Bottom line:
Lorlatinib is redefining what’s possible in advanced NSCLC. A majority of ALK+ pts remain progression – free at 7 YEARS on a single oral agent. We may be approaching functional cure territory for some patients!”

“ASCO26 – LCSM Oral
CROWN: Lorlatinib vs Crizotinib in ALK+ NSCLC
- mPFS NR (HR 0.19)
- 7-yr PFS 55% vs 3%
- 44% still on lorlatinib at 7y
- No new IC progression after 30m.”
“The downside: it may also disincentivize further RandD in ALK+ disease. Designing a trial large and long enough to outperform a >7-year median PFS in the control arm with lorlatinib is extraordinarily challenging—especially in a population representing <4% of lung cancers.”
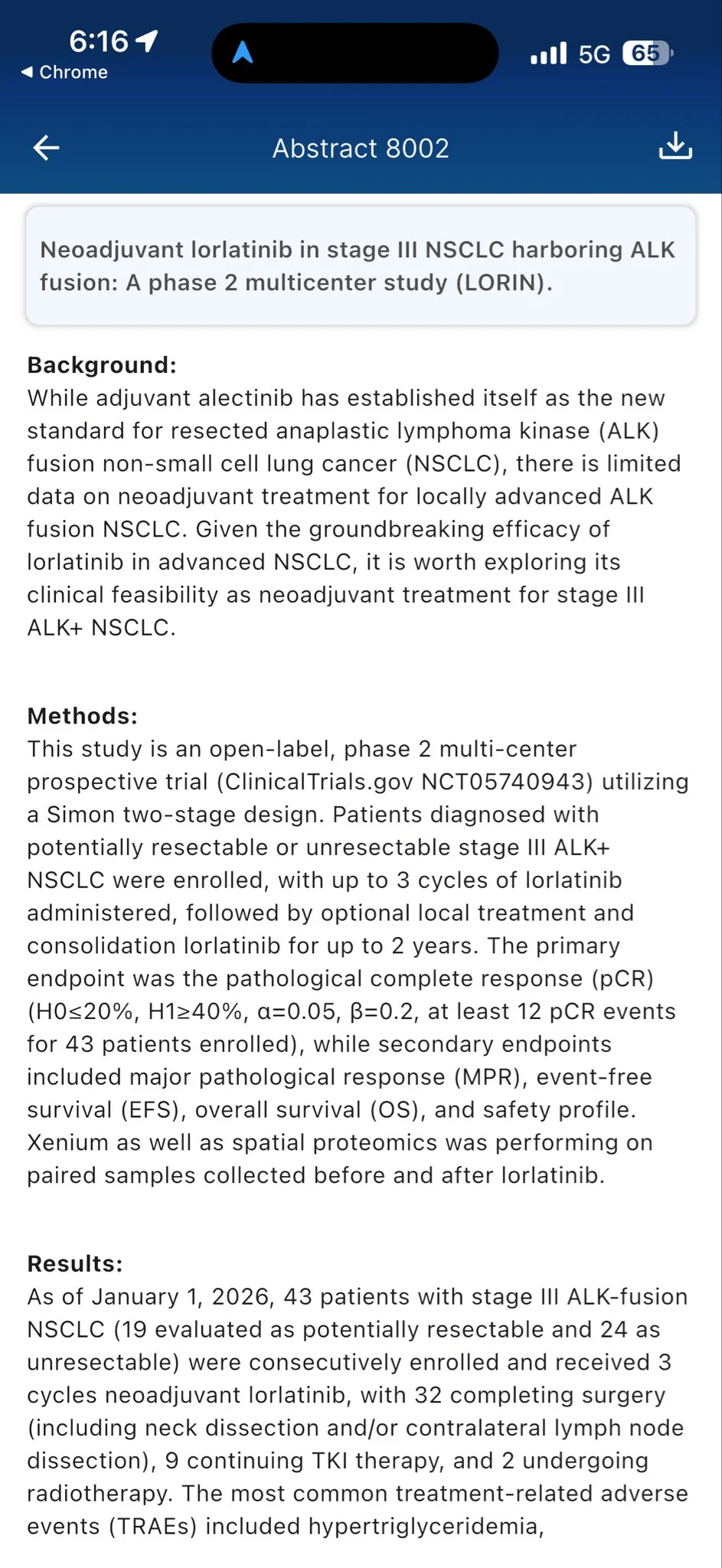
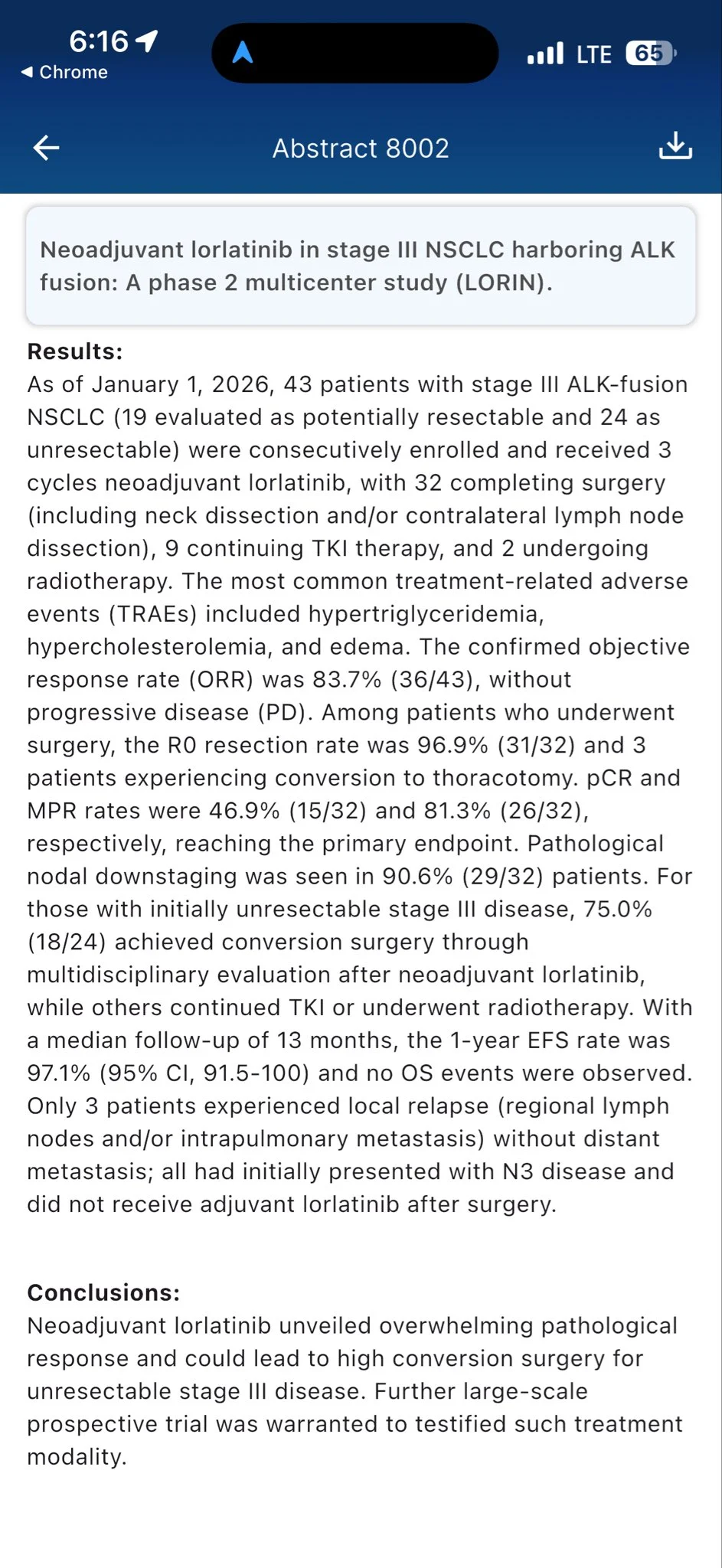
“Pleasant Surprise from ASCO26 Abstract 8002 (LORIN): neoadjuvant lorlatinib in stage III ALK+ NSCLC hits a pCR of 46.9% and MPR of 81.3% — pathologic responses we rarely see with neoadjuvant TKIs. 75% of initially unresectable pts converted to surgery. Targeted neoadj earning its seat.”
“Looks like pCR was named after CROWN – the CROWN jewel of ALK TKIs and path responses alike! But as a real CROWN princess – while lorla is amazing it also requires some extra pampering!”
“It’s astonishing that CROWN 7y update shows mPFS and median time to IC PFS are still NOT REACHED: Surprisingly only 34% needed a DR and 5% TRAE>discontinuation. Current 4th gen trials will be criticised for inadequate control arms.”
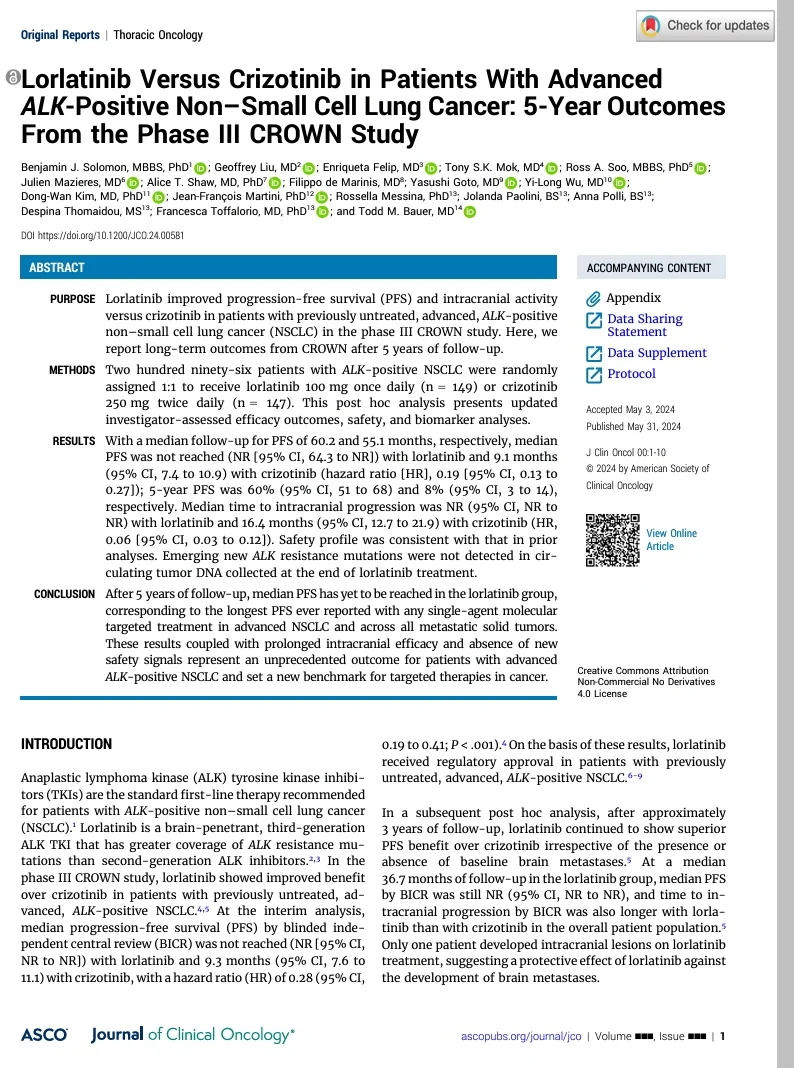
“CROWN: Ph III, n= 296, Lorlatinib vs. Crizotinib ALK+ mNSCLC – mPFS not reached for lorlatinib & 9.1 mos w/ crizotinib (HR:0.19) – 5yr PFS 60% w/ lorlatinib and 8% w/crizotinib. Improved intracranial progression (HR: 0.06) – AEs: w/ lorlatinib: HLD, weight gain.”
“Have u ever seen curves as wide as this for any drug recently? Lorlatinib for metastatic ALK positive NSCLC. Great results . It works With reduced dose also. Let’s hope it becomes more accessible.”
Title: Lorlatinib vs crizotinib as first-line treatment for advanced ALK+ nonsmall cell lung cancer: 7-year update from the phase 3 CROWN study.
Authors: Tony S. Mok, Benjamin J. Solomon, Enriqueta Felip, Todd M. Bauer, Geoffrey Liu, Yasushi Goto, Yi-Long Wu, Ross A. Soo, Julien Mazieres, Filippo de Marinis, Dong-Wan Kim, I-Ming Wang, Jolanda Paolini, Anna Polli, Nada Rifi, Francesca Toffalorio, Alice T. Shaw
Other articles about lung oncology on OncoDaily.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}