


Bhavin Vadodariya, Consultant Surgical Oncologist at SSO Cancer Hospital and Clinics, PSM Hospital, and Shankus Hospitals, shared a post on LinkedIn:
“During a recent extensive infratemporal fossa (ITF) clearance as part of composite resection, I was reminded of an important surgical principle:
The foramen ovale demands respect.
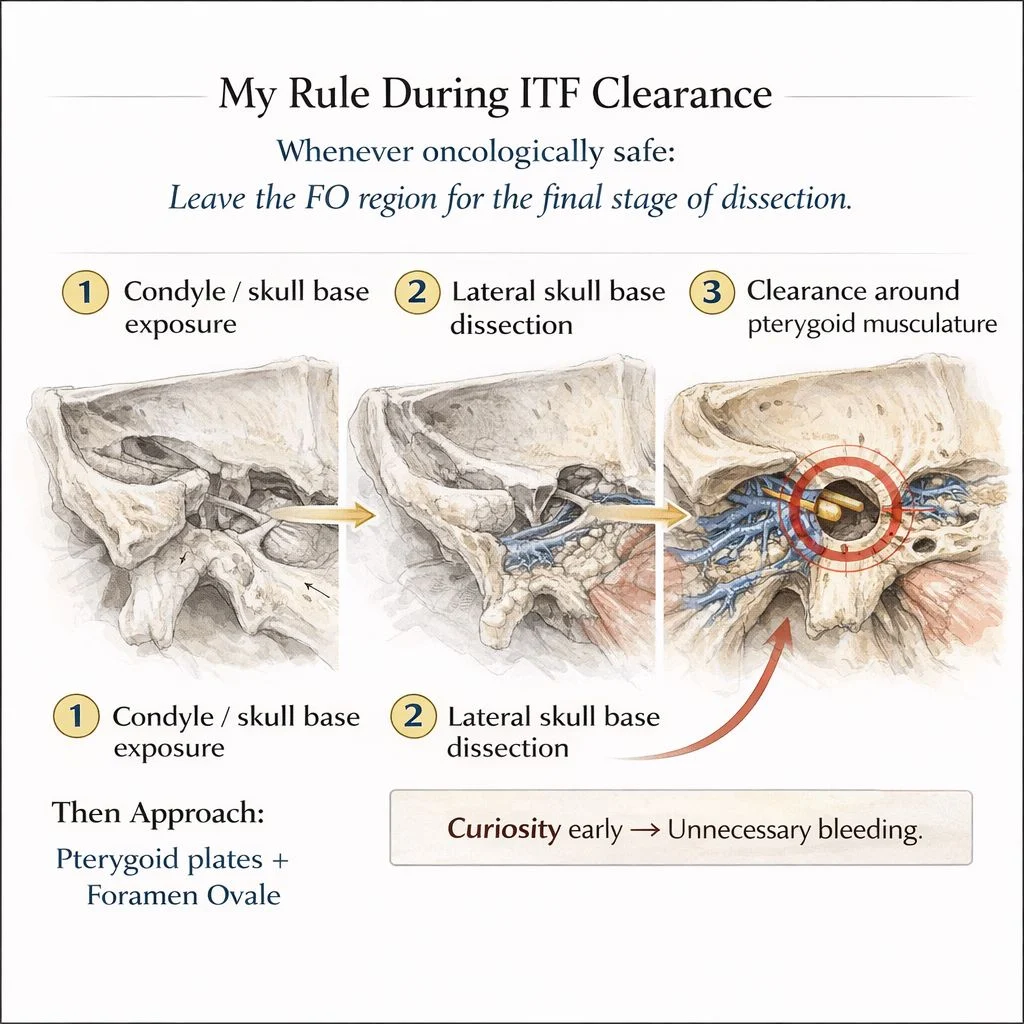
My rule is simple avoid the Foramen O vale region until the very end of dissection whenever oncologically safe.
During ITF clearance I first complete:
- Condyle / skull base exposure
- Clearance around pterygoid musculature
- Lateral skull base dissection
Only then do I approach the pterygoid plates and foramen ovale.
Why?
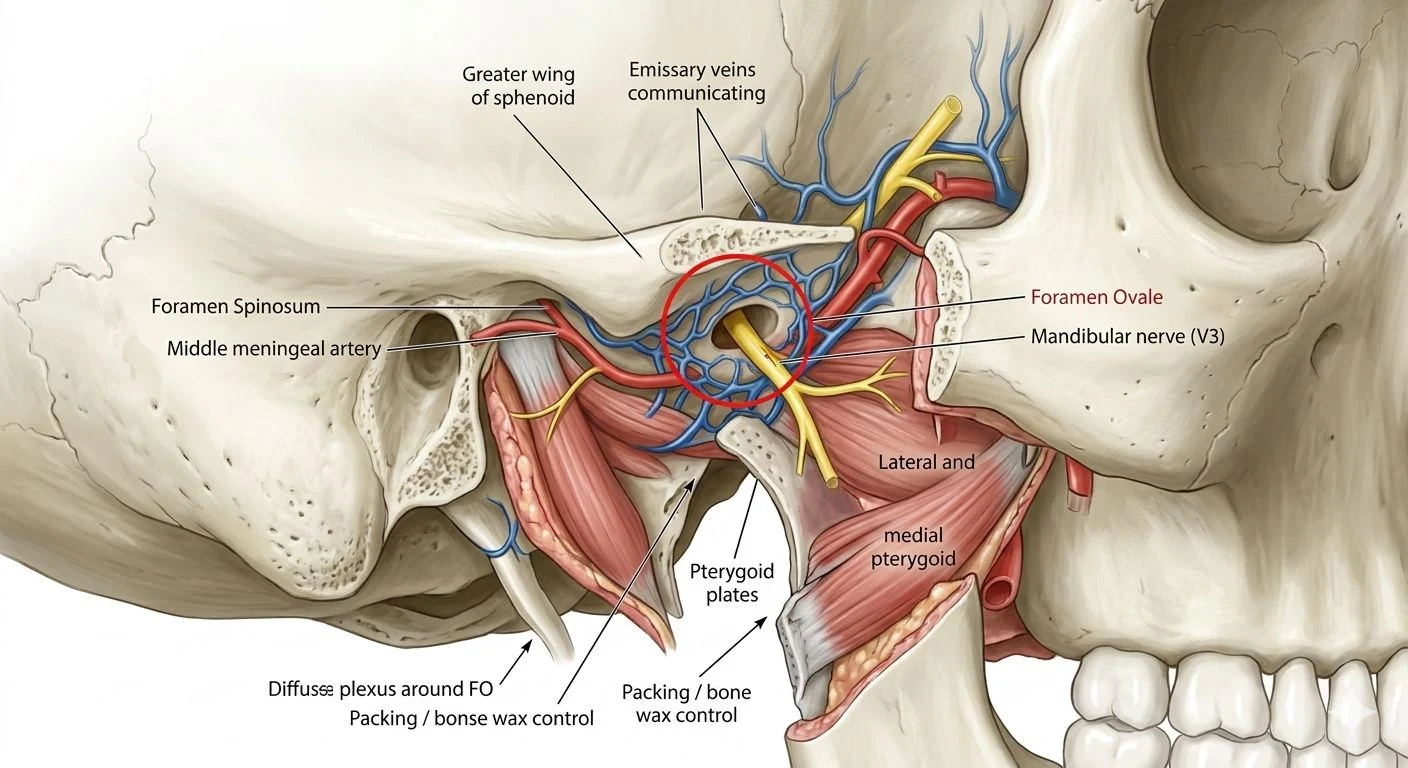
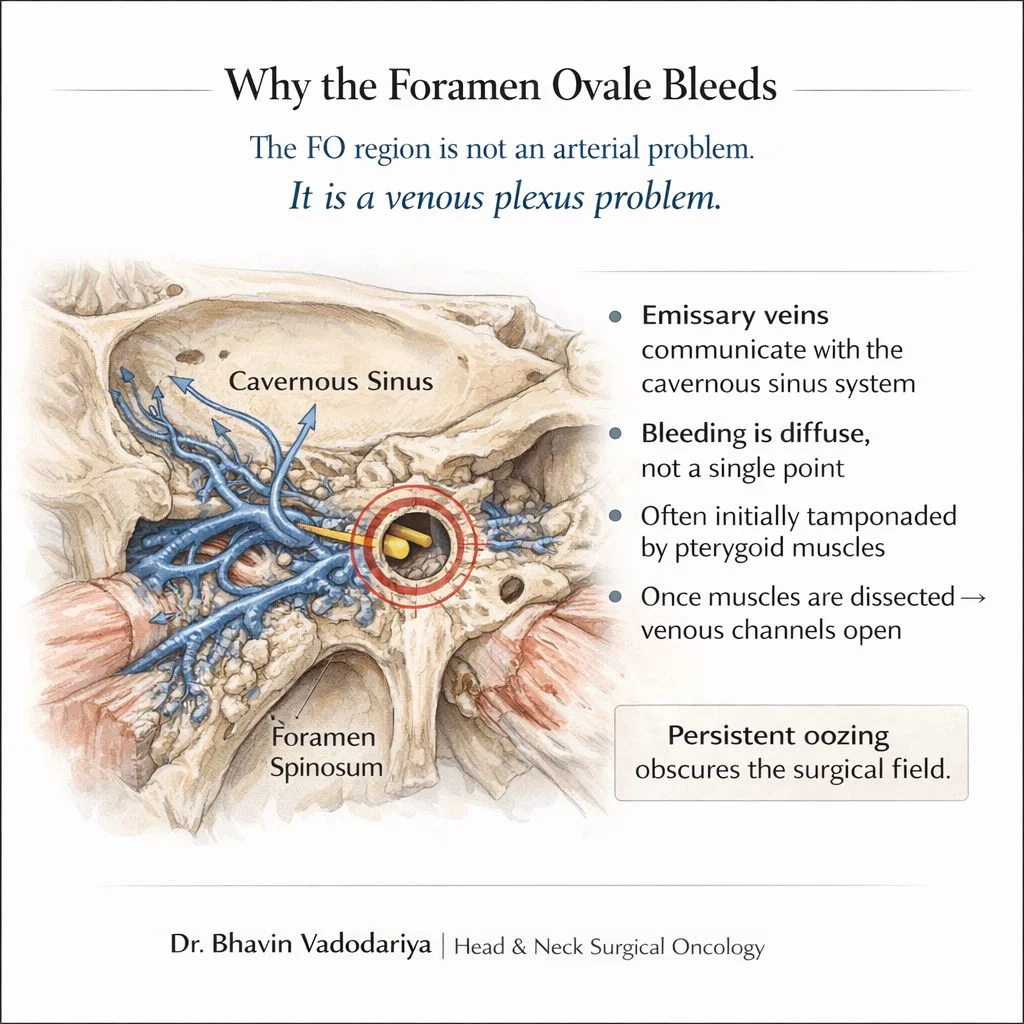
Because FO bleeding is rarely arterial.
It is a venous plexus problem.
Emissary veins communicate with the cavernous sinus system, producing diffuse venous oozing rather than a single bleeding point.
Often the bleeding is temporarily tamponaded by medial and lateral pterygoid muscles, but once these are dissected to achieve oncologic clearance, venous channels open.
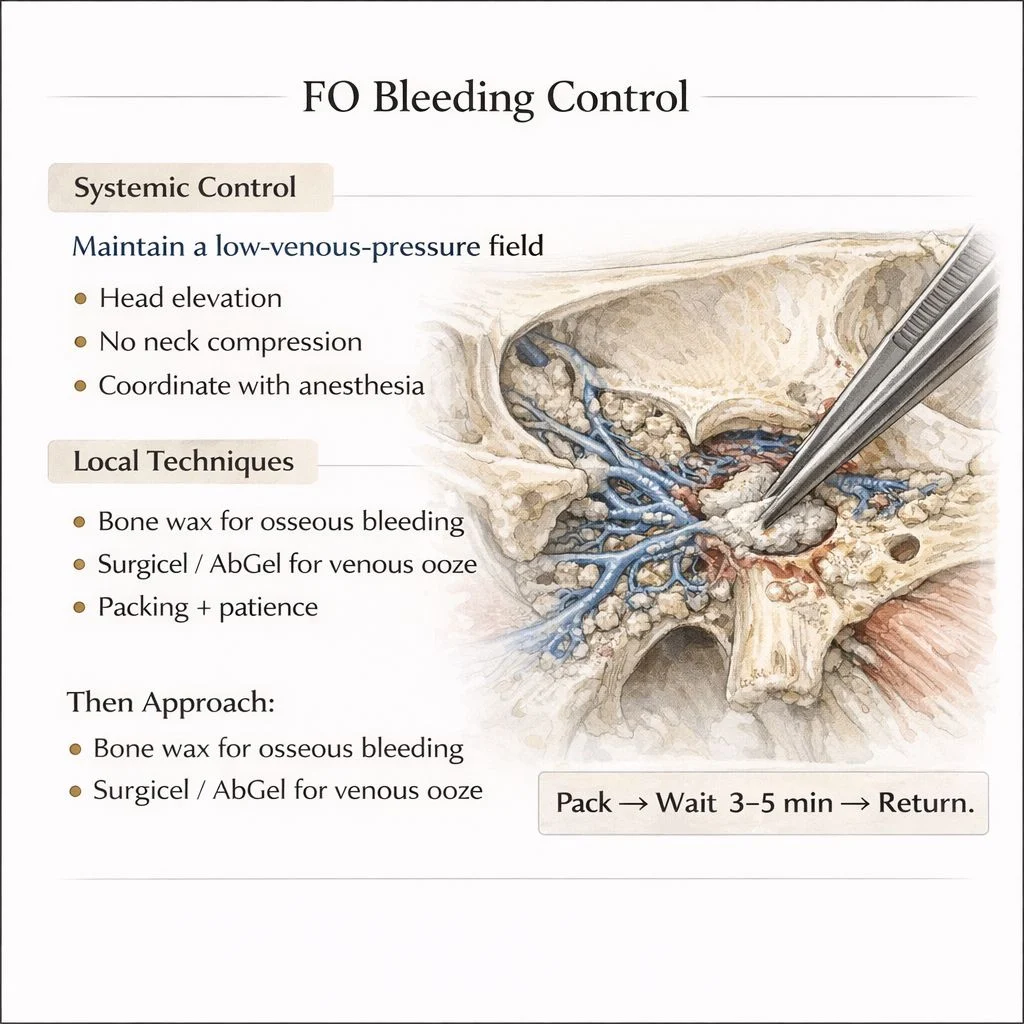
My Playbook:
- Leave Foramen ovale for last whenever possible
- Maintain a low venous pressure field (head elevation, hypotension)
- Gentle tissue handling
- Bone wax for osseous bleeding
- Surgicel / AbGel for venous ooze
- Packing > continuous suction
Pack – wait 3–5 minutes – return.
Continuous suction prevents clot formation and may lead to unrecognized blood loss.
Three Pearls I Tell Trainees:
- If suction is nonstop – strategy is wrong.
- Pack first, chase later.
- Patience is a hemostatic technique.
Sometimes the best surgical control comes from doing less.
What is your best pearl for controlling bleeding near the foramen ovale?”

Other articles featuring Bhavin Vadodariya on OncoDaily.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}