


At the 2026 ASCO Annual Meeting, James M. Larkin presented updated results from RAMPART, an international phase 3 randomized controlled trial evaluating durvalumab-based adjuvant immunotherapy compared with active monitoring in patients with resected primary renal cell carcinoma. The study was presented as Abstract LBA4511.
About the RAMPART Trial
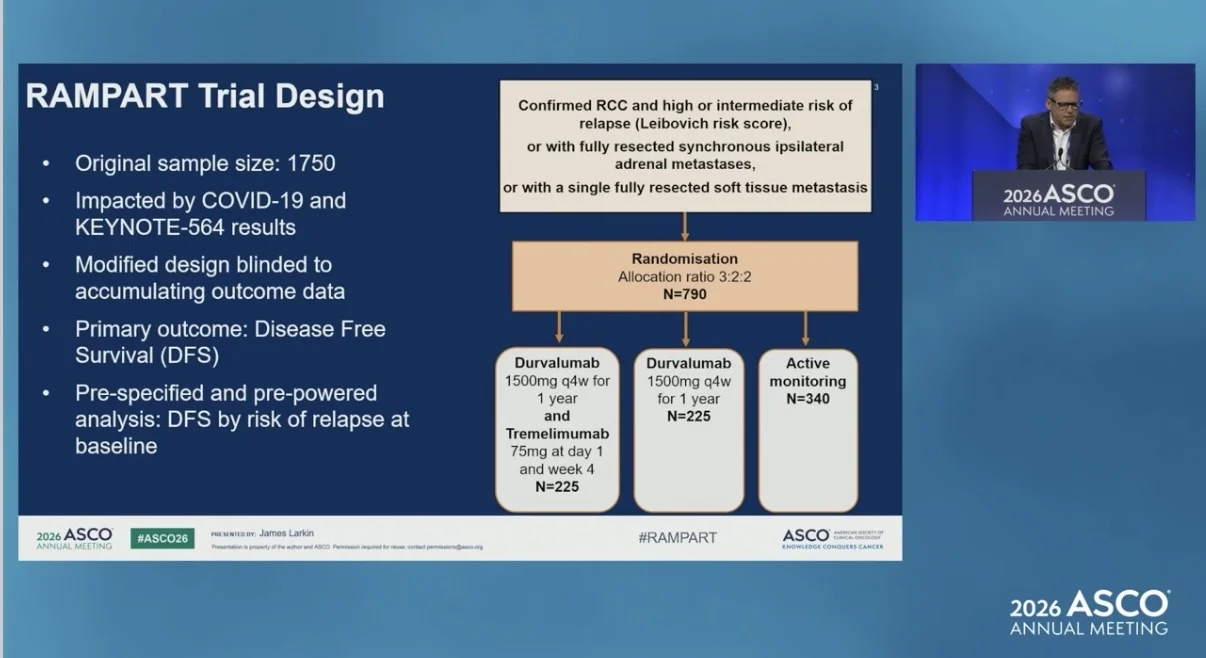
RAMPART evaluated one year of immune checkpoint inhibitor therapy compared with active monitoring in patients with renal cell carcinoma who had intermediate or high risk of recurrence after nephrectomy according to the Leibovich score, or who had undergone complete resection of limited metastatic disease.
Patients were randomized to receive active monitoring, durvalumab monotherapy, or durvalumab plus tremelimumab. Durvalumab was given at 1500 mg every 4 weeks for 1 year. In the combination arm, tremelimumab was given at 75 mg on day 1 and week 4. The primary outcome was disease-free survival in the intention-to-treat population.
Study Design
Participants were recruited from 80 sites and randomized in a 3:2:2 ratio to active monitoring, durvalumab monotherapy, and durvalumab plus tremelimumab.
Following the results of KEYNOTE-564, pembrolizumab became a treatment option for many patients who would have been eligible for RAMPART. The trial was also impacted by COVID-19, and recruitment was stopped earlier than planned.
The RAMPART design was revised without knowledge of the accumulated trial results. In the modified design, the study had 80% power to detect a hazard ratio of 0.60 for disease-free survival with durvalumab versus active monitoring, and 0.55 for durvalumab plus tremelimumab versus active monitoring. The overall familywise type I error rate remained controlled at 2.5% one-sided across all primary analyses.

Disease-Free Survival
At a median follow-up of 3.5 years, durvalumab monotherapy showed a numerical difference in disease-free survival but did not reach statistical significance compared with active monitoring. Three-year DFS was 78% with durvalumab monotherapy and 72% with active monitoring. The DFS hazard ratio was 0.74, with a 95% CI of 0.53 to 1.04 and a one-sided p-value of 0.041. Durvalumab plus tremelimumab significantly improved DFS compared with active monitoring, with HR 0.65, 95% CI 0.45 to 0.93, and p=0.0094.
Results by Risk Group
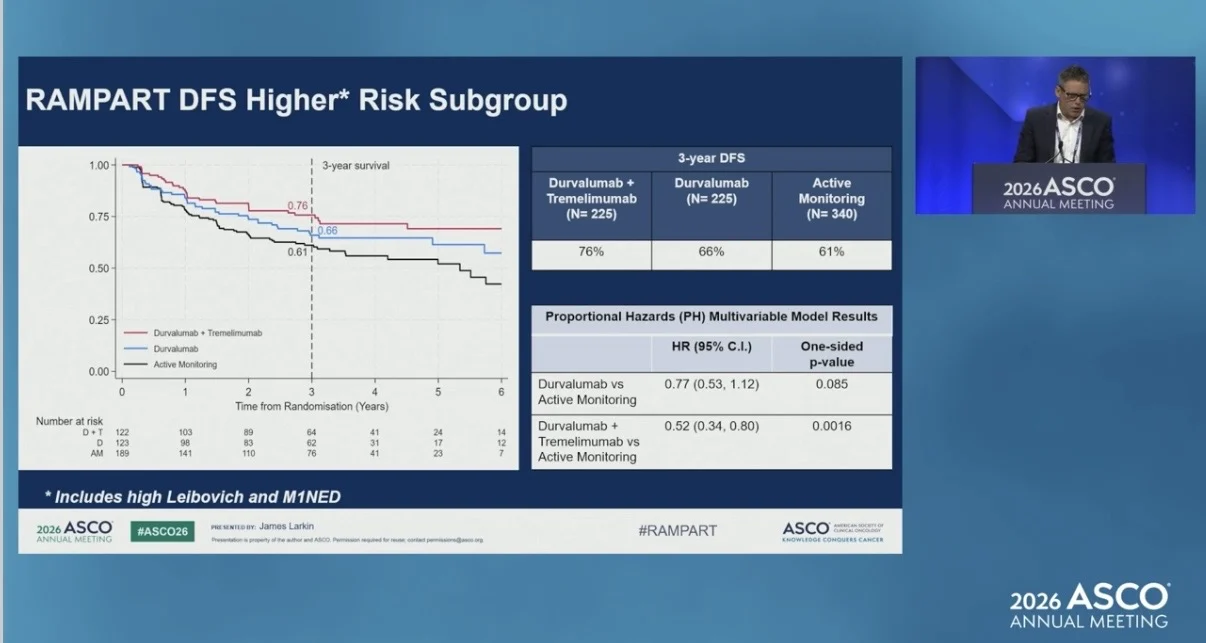
In the higher-risk subgroup, which included patients with high Leibovich risk and M1NED disease, 3-year DFS was 76% with durvalumab plus tremelimumab, 66% with durvalumab monotherapy, and 61% with active monitoring.
In this subgroup, durvalumab plus tremelimumab improved DFS versus active monitoring, with HR 0.52, 95% CI 0.34 to 0.80, and p=0.0016. Durvalumab monotherapy showed HR 0.77, 95% CI 0.53 to 1.12, and p=0.085.

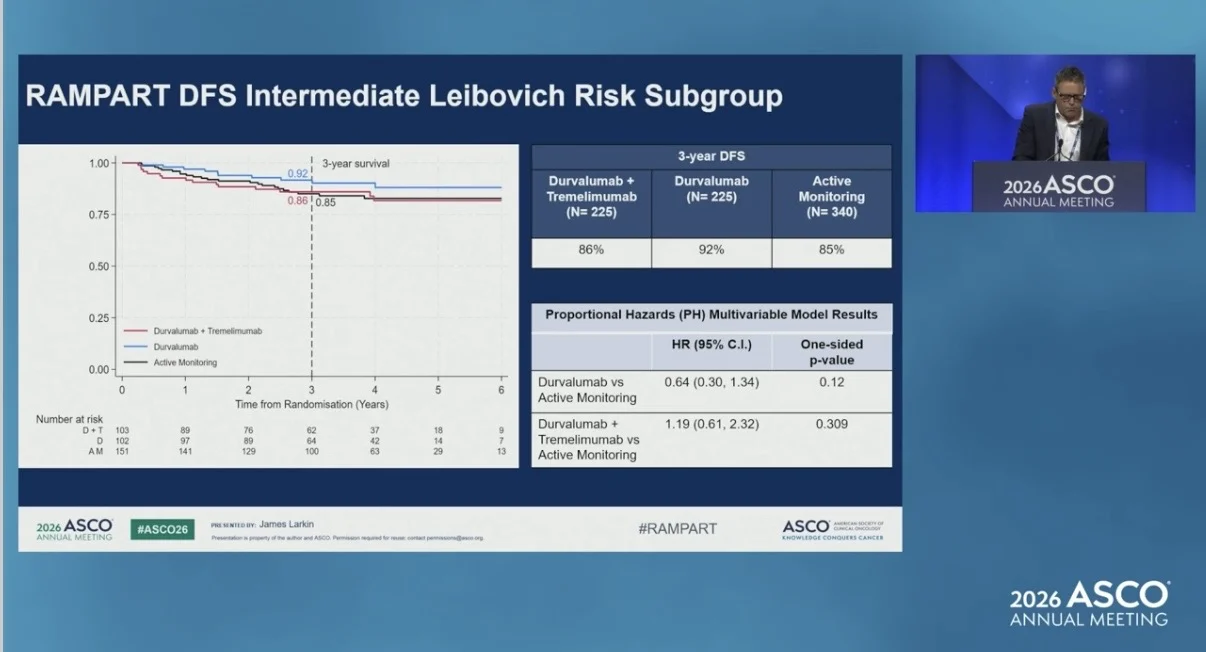
In the intermediate-risk subgroup, 3-year DFS was 86% with durvalumab plus tremelimumab, 92% with durvalumab monotherapy, and 85% with active monitoring. The interaction p-value was 0.019 for durvalumab plus tremelimumab and 0.663 for durvalumab monotherapy.

Overall Survival and Quality of Life
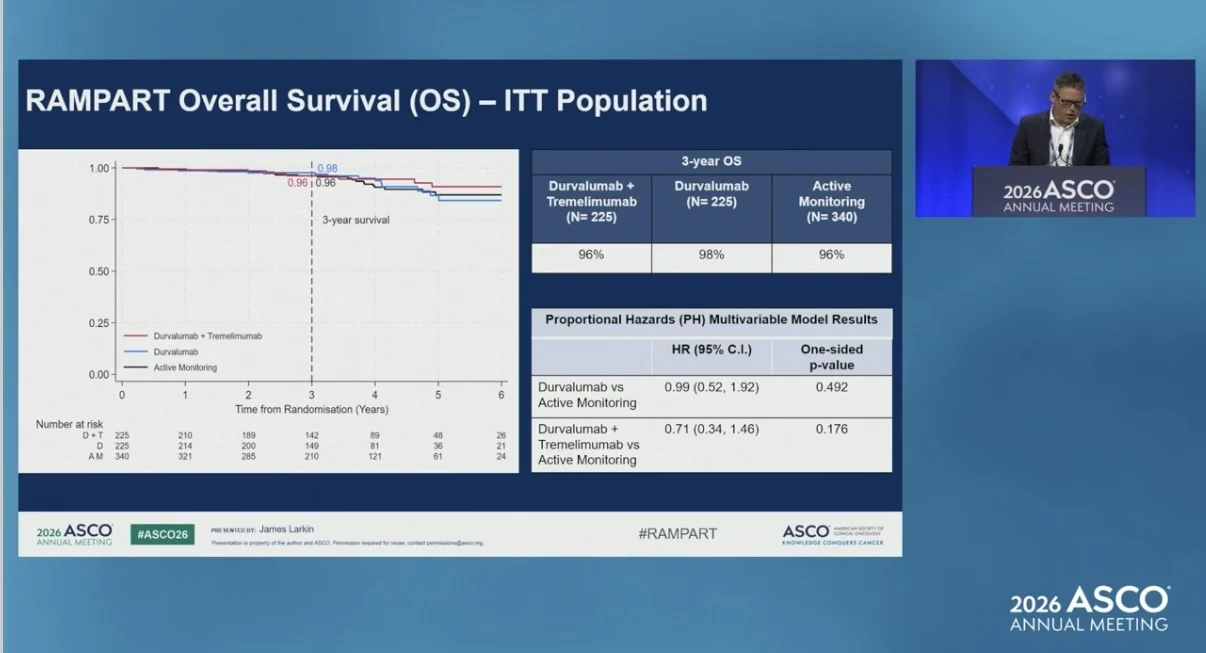
Overall survival did not show a statistically significant difference at this analysis. At 3 years, OS was 96% with durvalumab plus tremelimumab, 98% with durvalumab monotherapy, and 96% with active monitoring. No statistically significant or clinically meaningful difference in overall health and quality of life was observed at month 15 with either durvalumab monotherapy or durvalumab plus tremelimumab compared with active monitoring.

Safety
Safety findings were consistent with the known profiles of durvalumab and tremelimumab, but rare immune-mediated adverse events, including fatal myocarditis and myasthenia gravis, were observed. Grade 3 or 4 adverse events occurred in 41% of patients receiving durvalumab plus tremelimumab, 30% receiving durvalumab monotherapy, and 9% on active monitoring. Serious adverse events occurred in 34%, 19%, and 6%, respectively. Treatment-related deaths were reported in 2 patients receiving durvalumab plus tremelimumab and 1 patient receiving durvalumab monotherapy.
Takeaway
In RAMPART, durvalumab monotherapy did not significantly improve disease-free survival compared with active monitoring after resection of renal cell carcinoma. Durvalumab plus tremelimumab significantly improved disease-free survival compared with active monitoring, with the clearest benefit seen in the higher-risk subgroup. Overall survival was not significantly different at this analysis, and no evidence of a difference in overall health and quality of life was observed at month 15.

The full abstract is available on the official ASCO website.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}