


Zhaohui Su, VP, Strategic Consulting at Veristat, shared Babak Jamshidi’s, Visiting Researcher – Medical Statistician at King’s College London post on LinkedIn, adding:
“Regulators are increasingly accepting fit – for – purpose real-world data (RWD) to support safety monitoring, effectiveness assessments, and even regulatory submissions, provided that methodological rigor is clearly demonstrated. Below is an insightful post by Babak Jamshidi on integrating RCT and RWE.
Veristat provides flexible end-to-end solutions.”
To which Babak Jamshidi added:
“Combining RCTs and Real-World Evidence: Methodological Challenges and Best Practices
As healthcare data evolves – driven by digital health, linked databases, and innovative designs – the need to combine evidence from Randomised Controlled Trials (RCTs) and Non-Randomised Studies of Interventions (NRSIs) is becoming unavoidable.
But this integration is far from straightforward.
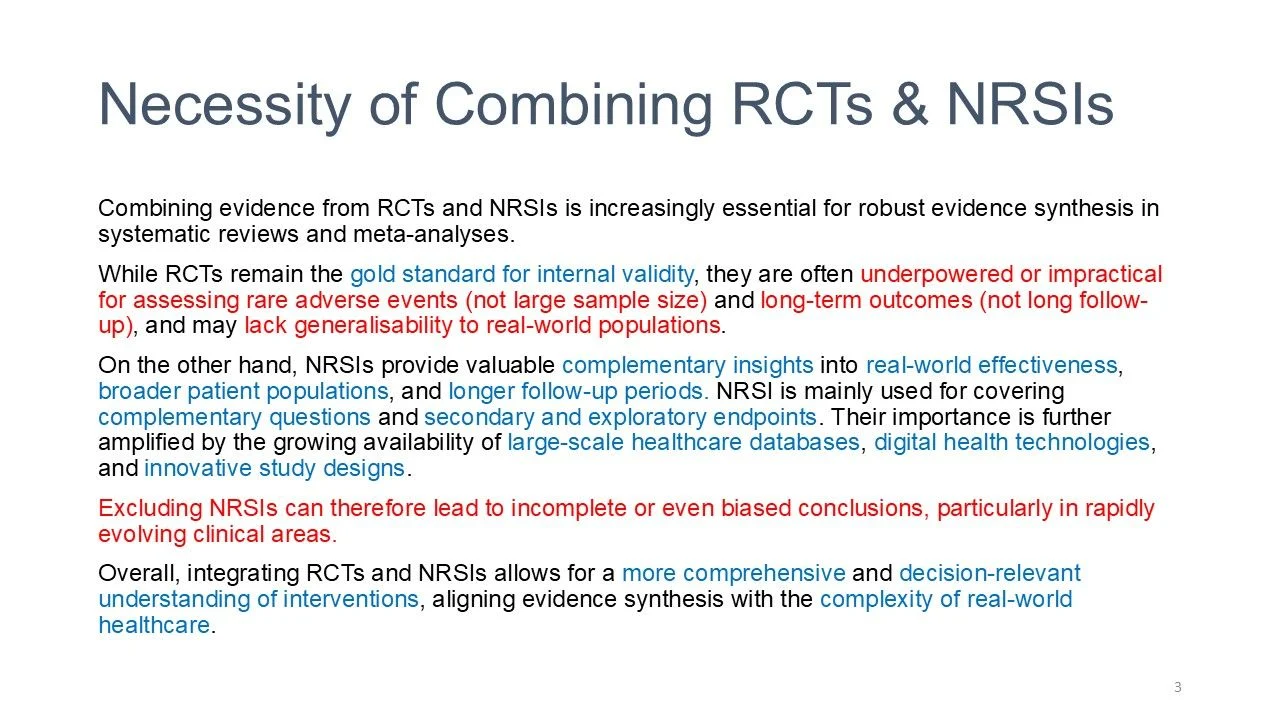
Why combine RCTs and NRSIs?
RCTs – Strong internal validity, but limited by:
- Small samples for rare events
- Short follow-up
- Restricted populations
NRSIs – Provide:
- Real-world effectiveness
- Long-term outcomes
- Broader populations
Excluding either source can lead to incomplete conclusions.
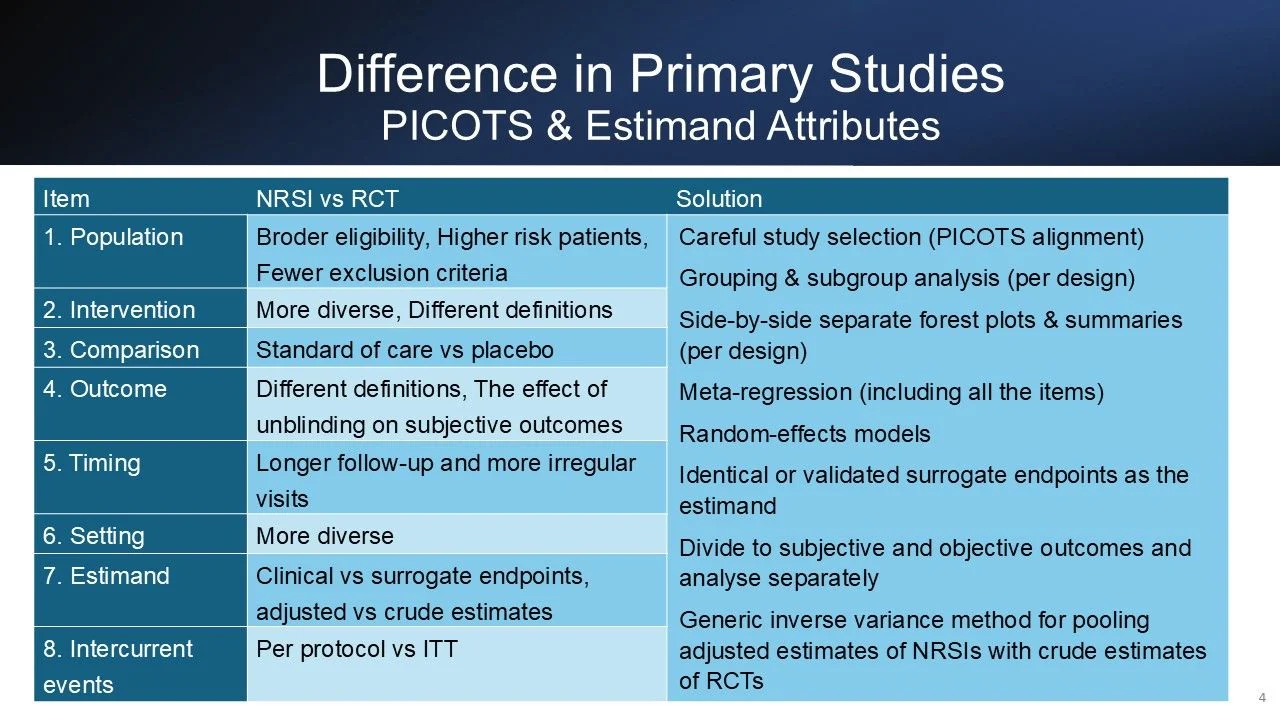
The Core Challenge
- RCTs and NRSIs differ across key dimensions:
- Population, intervention, comparator
- Outcome definitions
- Timing and follow-up
- Study setting
- Estimands (adjusted vs crude, surrogate vs clinical)
These differences drive heterogeneity and bias.
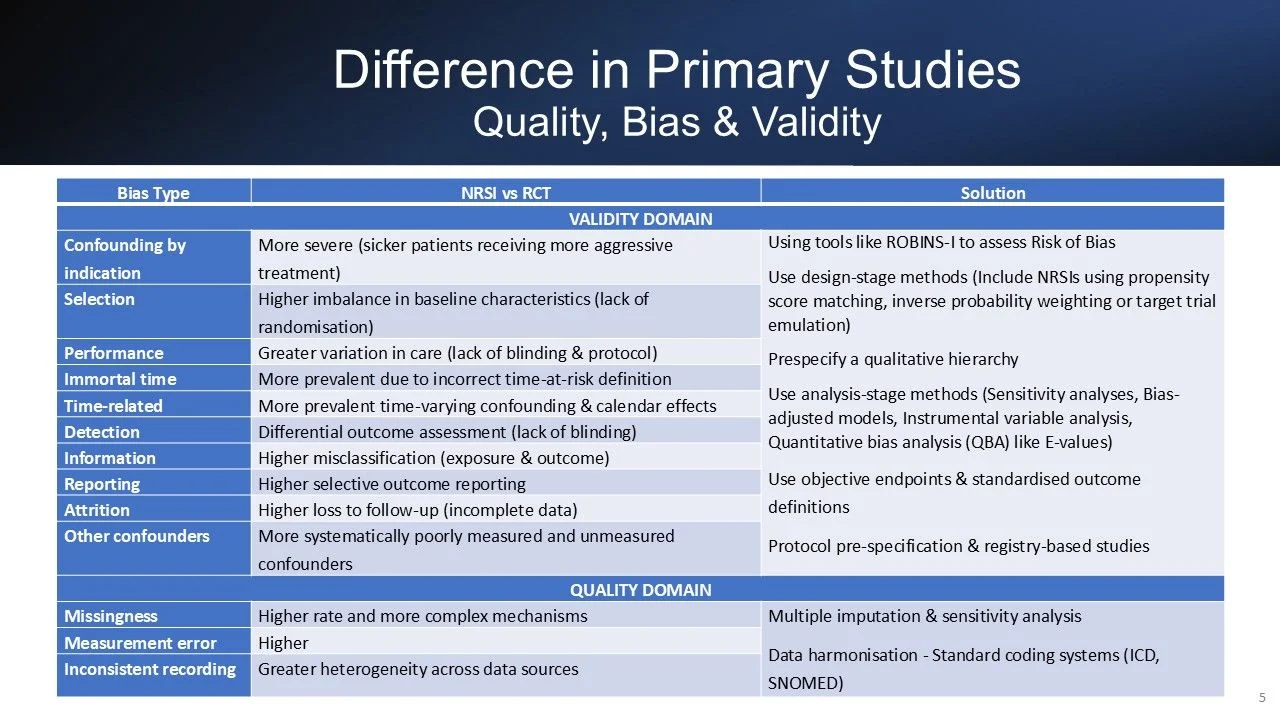
Bias and Quality Challenges
Key risks in NRSIs include:
- Confounding by indication
- Selection bias
- Immortal time bias
- Detection/surveillance bias
- Misclassification and missing data
These can distort effect estimates if not addressed.
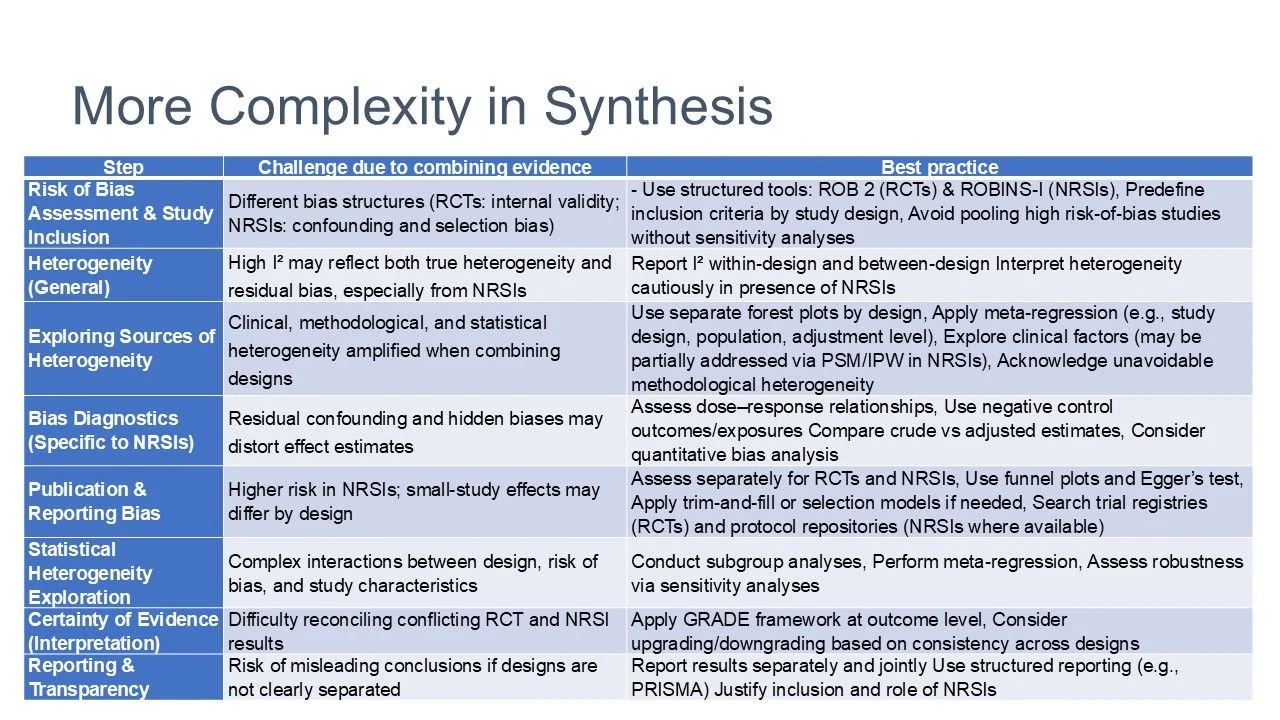
Best Practice
- Use ROB 2 (RCTs) and ROBINS-I (NRSIs)
- Start with design-stratified analyses
- Explore heterogeneity (within and between designs)
- Apply:
Meta-regression
Sensitivity analyses
Subgroup analyses
- Diagnose bias (dose–response, negative controls)
- Assess publication bias separately
- Evaluate certainty using GRADE
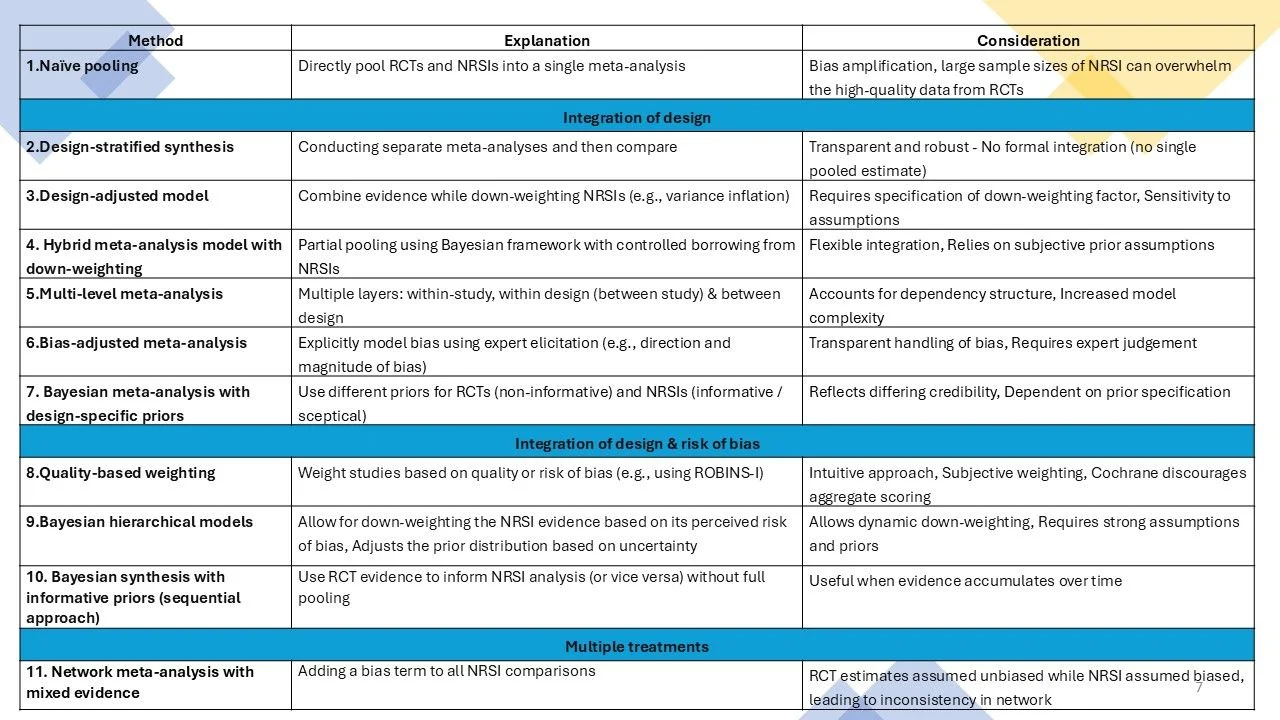
Methods for Combining Evidence
- Naïve pooling – bias amplification
- Design-stratified synthesis – transparency
- Design-adjusted models – down-weight NRSIs
- Bayesian/hierarchical models – controlled borrowing
No one-size-fits-all approach.
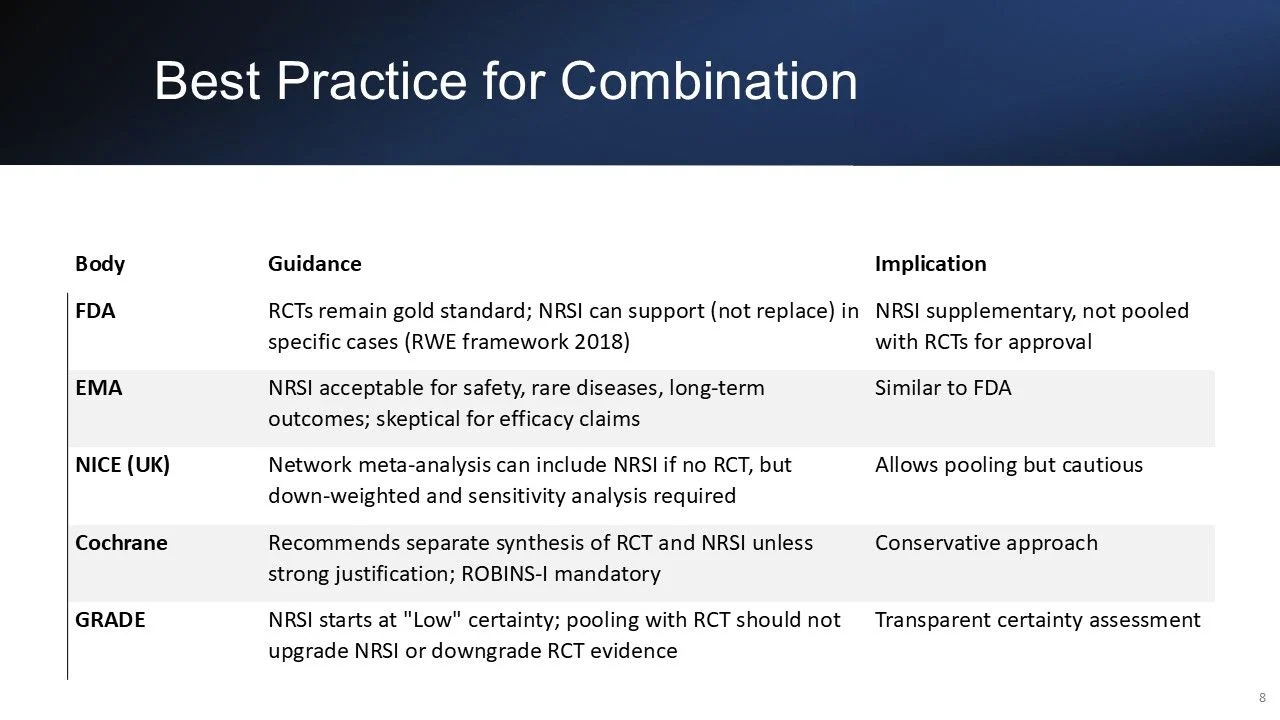
Regulatory Perspective
- FDA/EMA – NRSIs are supportive
- NICE – Allows inclusion with caution
- Cochrane – Prefer separate synthesis
- GRADE – NRSIs start as low certainty
Final Takeaway
‘RCTs provide internal validity, NRSIs provide external validity. High-quality synthesis requires integrating both—carefully and transparently.’
Closing Thought
The future is not choosing between RCTs and RWE…
It is about combining them intelligently while preserving rigour.”

Other articles featuring Zhaohui Su on OncoDaily.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}