


Fabio Ynoe de Moraes, Radiation Oncologist and Associate Professor at Queen’s University, shared a post on LinkedIn about a paper by Yang Xu et al. published in the International Journal of Radiation Oncology, Biology and Physics:
“Geographic access to radiotherapy in Canada – who is left behind, and where to build next
A new population-level study mapped access for 36.9M Canadians across 56,686 census areas and benchmarked eightoptimal build sites.
Key numbers:
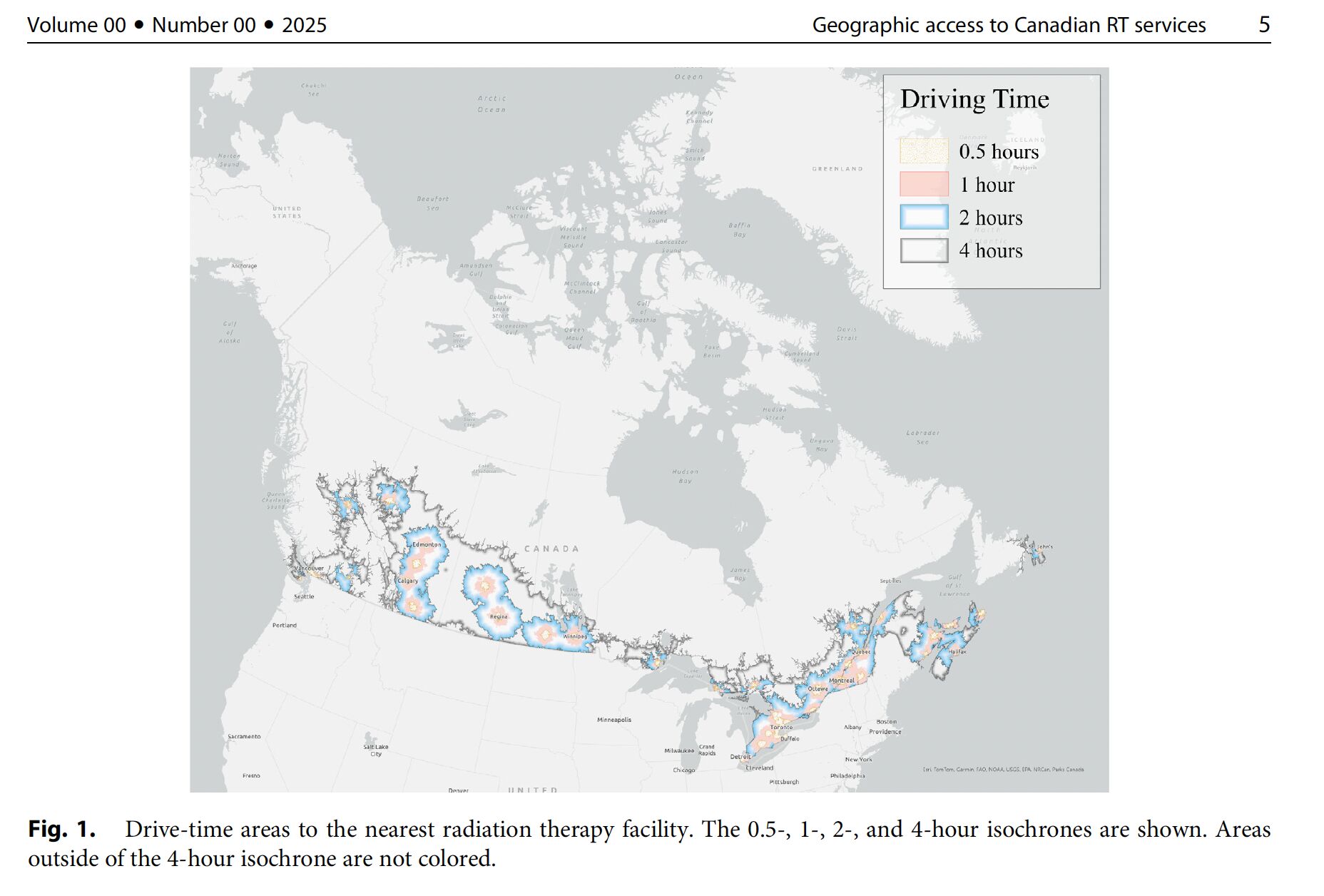
- Median travel to nearest RT: 22.8 min (IQR 12.9–44.9)
- Poor access: 9.3% (3,445,472 people) face >2-hour one-way drives
Provincial inequity
- Ontario: 3.3% vs Newfoundland and Labrador: 47.6% with poor access
- Saskatchewan: 28.5%
- New Brunswick: 28%
Territorial gap
- 0 RT facilities across all three northern territories
System capacity
- 🇨🇦 1.4 RT facilities per million people
- 🇦🇺 4.1 | 🇺🇸 7.1; in the U.S., <2% live >80 km from an RT centre
Who bears the burden (adjusted models)
- Higher odds among seniors (≥55) and men
- Higher with greater Indigenous identity representation in a community
- Lower among visible minorities, immigrants, and post-secondary educated populations
Eight high-impact build clusters
Nanaimo (BC), Rouyn-Noranda (QC), Kamloops (BC), Lloydminster (AB), Bathurst (NB), Medicine Hat (AB), Owen Sound (ON), Castlegar (BC)
- Building all eight could cut poor access by ~1.13M people (−32.7%)
- Nanaimo alone: −243,402 (7.1% of national poor access; 28.5% within BC)
Why this matters (patients and policy)
- Travel time shapes modality choice, adherence, and time/financial toxicity—especially for rural, northern, and
- Indigenous communities. High-volume centres improve throughput, but concentrated siting can amplify travel inequities.
- Targeted expansion = greatest equity gain per dollar.
Action plan (evidence-linked)
- Prioritize the eight sites in provincial capital plans—highest impact and feasibility
- Pair bricks with workforce: fund RTT, physics, RO positions; use hub-and-spoke QA, virtual contour review and tumour boards for quality at satellites
- Reduce avoidable travel: scale hypofractionation where appropriate; formalize travel-lodging support for >2-hour cases
- Track equity: report >2h drive-time and Indigenous-stratified access every census cycle
Bottom line: Canada’s median travel is reasonable, but millions remain beyond a feasible RT commute. A focused build in eight locations could shrink the gap by ~one-third—if coupled with workforce planning and distributed delivery.”
Title: Geographic Access to Radiation Therapy Services in Canada
Authors: Yang Xu, Oluwaseun Davies, Shaun K. Loewen
You can read the Full Article in the International Journal of Radiation Oncology, Biology and Physics.

More posts featuring Fabio Ynoe de Moraes.
{kind=link}
{kind=link}