


Amol Akhade, Senior Consultant at Fortis Hospitals Mumbai, shared a post on LinkedIn:
“EGFRm NSCLC at WCLC25: Two Curves, Two Stories
We now have two positive OS trials challenging the old dogma of osimertinib monotherapy as the first-line standard for EGFR-mutant NSCLC. Both MARIPOSA and FLAURA2 demonstrate clear survival gains — but with very different strategies.
- MARIPOSA (Amivantamab + Lazertinib vs Osimertinib) Median OS: Not Estimable vs 36.7 mo with osi HR for death: 0.75 (95% CI 0.61–0.92; p=0.005) 3-yr OS: ~60% vs 51%. Curves continue to separate, tail looks stronger
Biologic strategy: upfront dual EGFR + MET blockade Chemo-free regimen, but IV amivantamab (infusion reactions, skin/GI toxicity) + oral lazertinib (not yet globally available). Represents a future-looking approach with potential durability.
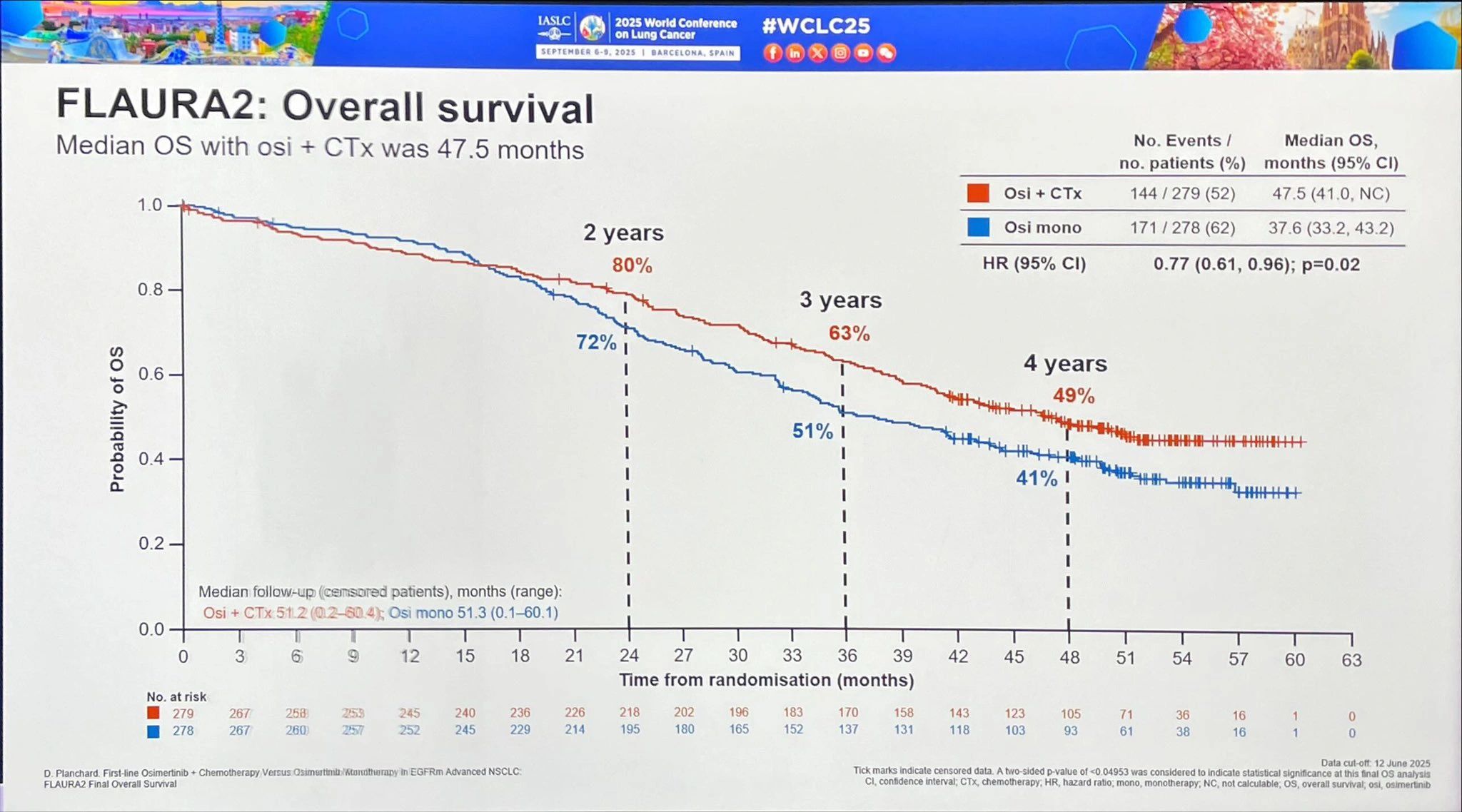
FLAURA2 (Osimertinib + Chemotherapy vs Osimertinib) Median OS: 47.5 vs 37.6 mo HR for death: 0.77 (95% CI 0.61–0.96; p=0.02) 3-yr OS: 63% vs 51% 4-yr OS: 49% vs 41%. Chemo backbone well known and globally available (pemetrexed maintenance is the trade-off). Represents the pragmatic present, accessible and already practice-changing in guidelines
How do we interpret this?
Both trials show ~10-month OS gain vs osimertinib alone.
MARIPOSA: Attractive curve — OS not reached, widening separation, chemo-free life. Feels like the biologic future. FLAURA2: Grounded, reproducible, implementable in today’s practice — especially in real-world settings and LMICs where chemo is easier to access than novel antibodies. If you were the patient, which curve would you want to be on? MARIPOSA → durability, biologic elegance, no chemo. FLAURA2 → proven, available, with defined survival medians.
The truth is: both represent progress. The question is less about ‘which is better’ and more about how we bring these advances into the clinic in a way that balances efficacy, toxicity, access, and patient preference.
Takeaway: EGFRm NSCLC is no longer a monotherapy story. Combination is the new paradigm — whether via biologics or chemotherapy. The era of osimertinib alone is behind us.”

More posts featuring Amol Akhade on OncoDaily.
{kind=link}