


Comprehensive genomic profiling has changed lung cancer care.
But a new analysis in JCO Oncology Practice shows that many patients still wait weeks before genomic results are available — and the largest delay may occur before the test is even ordered.
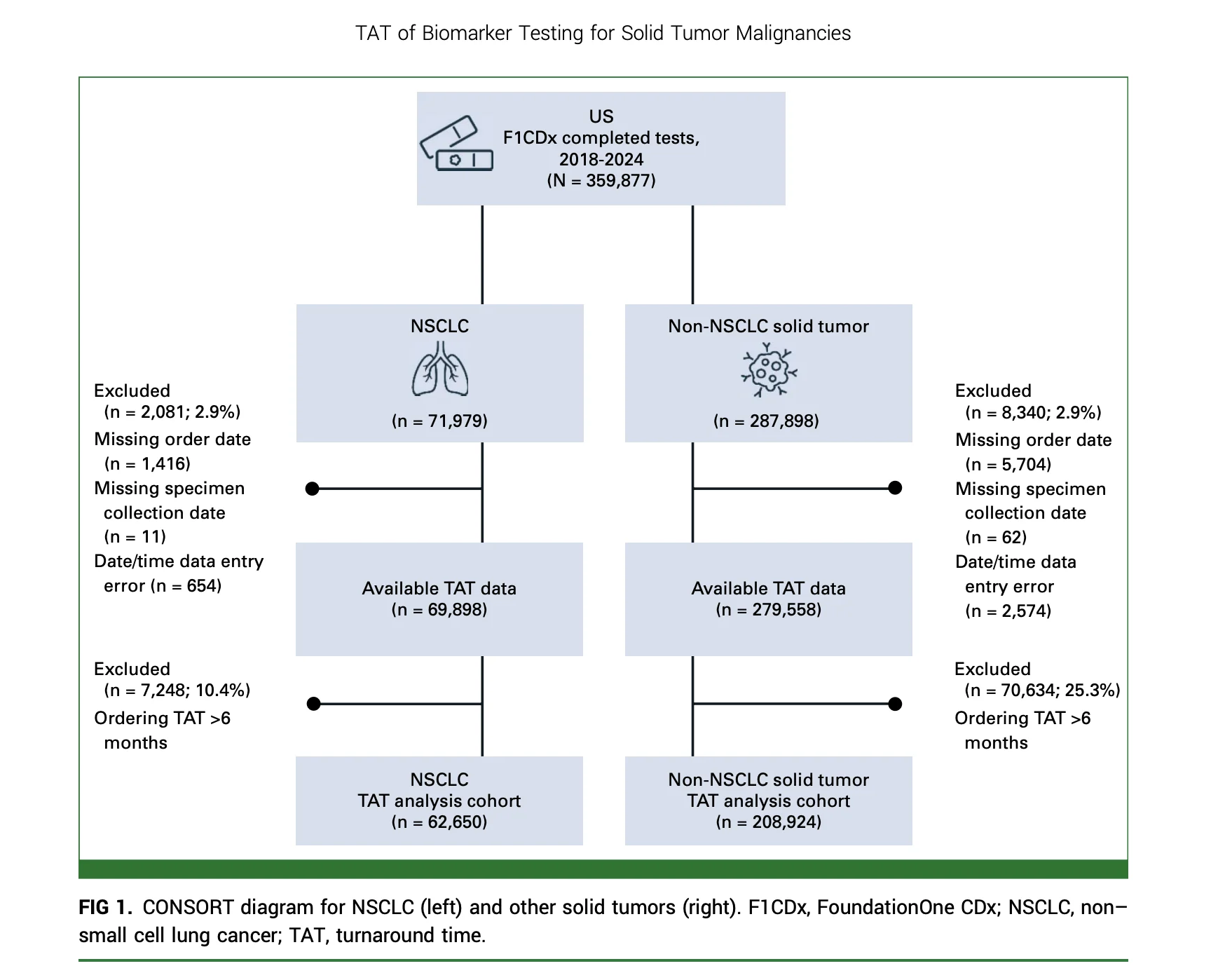
The study by Fox and colleagues analyzed tissue-based comprehensive genomic profiling turnaround time across 271,574 solid tumor samples from 5,497 clinical sites in the United States between 2018 and 2024.
The investigators found that overall turnaround time improved over the study period. However, the time from biopsy to ordering genomic testing did not meaningfully improve and remained the largest contributor to delay.
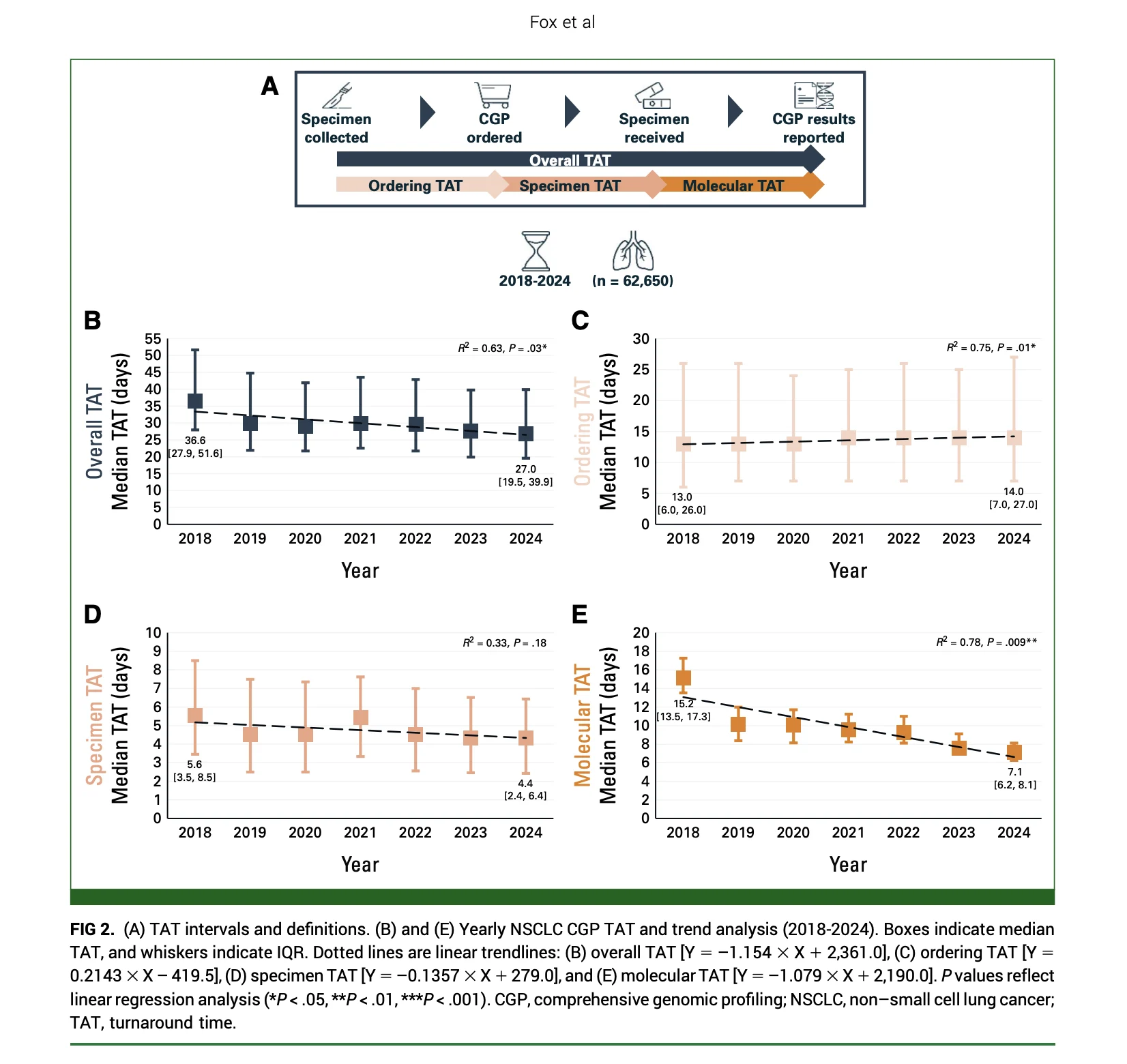
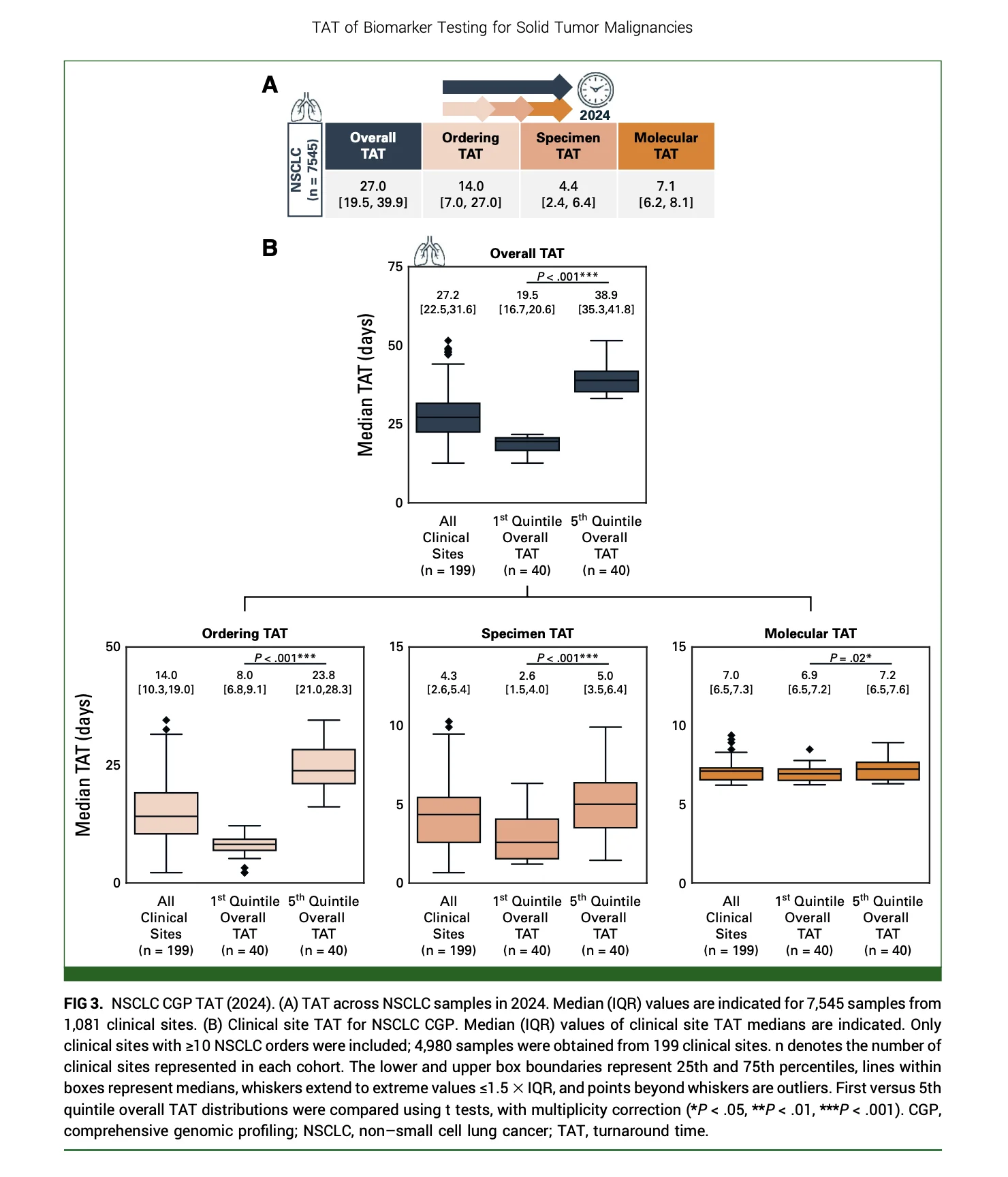
For non-small cell lung cancer, the median overall turnaround time in 2024 was 27.0 days. The median time from specimen collection to CGP order was 14.0 days, compared with 4.4 days for specimen transfer and 7.1 days for molecular laboratory processing.
In other words, for many patients, the slowest part of precision oncology was not the sequencing itself.
It was getting the test ordered.

Why Timing Matters in Lung Cancer
Lung cancer is one of the clearest examples of why genomic testing must be fast.
In advanced non-small cell lung cancer, first-line treatment decisions often depend on biomarkers such as EGFR, ALK, ROS1, BRAF, MET, RET, NTRK, KRAS, HER2, PD-L1, tumor mutational burden, and other molecular features.
The same principle is increasingly important in earlier-stage disease.
Biomarkers can influence the choice between adjuvant targeted therapy, neoadjuvant chemoimmunotherapy, perioperative approaches, and post-chemoradiotherapy strategies.
The authors note that in NSCLC, treatment choice and timing are largely dependent on timely biomarker testing. When results are delayed, clinicians may face pressure to start treatment before the complete molecular picture is available.
That can lead to missed targeted therapy opportunities, less precise treatment selection, avoidable toxicity, patient anxiety, and potentially worse outcomes.
A Large Real-World Dataset
The study included U.S. solid tumor samples successfully profiled with FoundationOne CDx tissue-based comprehensive genomic profiling from 2018 through 2024.
FoundationOne CDx interrogates 324 cancer-associated genes and complex biomarkers, including microsatellite instability and tumor mutational burden.
The final analysis included:
- 271,574 solid tumor malignancies
- 62,650 NSCLC samples
- 208,924 other solid tumor samples
- 5,497 clinical sites
Among the NSCLC cohort, 61.5% had lung adenocarcinoma, 21.3% had squamous cell carcinoma, and 14.5% were classified as NSCLC not otherwise specified.
The study focused on four turnaround time intervals:
- Ordering turnaround time — specimen collection to CGP order
- Specimen turnaround time — CGP order to specimen receipt at the laboratory
- Molecular turnaround time — specimen receipt to CGP report
- Overall turnaround time — specimen collection to CGP result reporting
This structure allowed the investigators to identify where delays actually occurred.

Overall Turnaround Time Improved, but Ordering Did Not
Across all solid tumors, the median overall turnaround time decreased from 43 days in 2018 to 32 days in 2024.
For NSCLC specifically, overall turnaround time decreased from 36.6 days in 2018 to 27.0 days in 2024.
This improvement was largely driven by faster molecular laboratory processing.
In NSCLC, molecular turnaround time decreased from 15.2 days in 2018 to 7.1 days in 2024.
That is an important operational achievement.
However, ordering turnaround time did not improve. In fact, for NSCLC, median ordering time was 13.0 days in 2018 and 14.0 days in 2024.
This is the core finding of the study.
The laboratory became faster.
The clinical ordering pathway did not.
The Biggest Variation Was Between Clinical Sites
The study also showed major differences between clinical sites.
For NSCLC in 2024, among sites with at least 10 NSCLC orders, the shortest overall turnaround time quintile had a median overall TAT of 19.5 days, while the longest quintile had a median overall TAT of 38.9 days.
The biggest difference was ordering time.
The shortest quintile had a median ordering TAT of 8.0 days.
The longest quintile had a median ordering TAT of 23.8 days.
That means the least efficient sites could potentially save more than two weeks by improving the biopsy-to-order workflow.
For a patient with newly diagnosed advanced lung cancer, two weeks is not a small delay.
It is two more weeks of uncertainty.
It may also be the difference between starting biomarker-informed therapy and starting empiric treatment because results are not yet available.

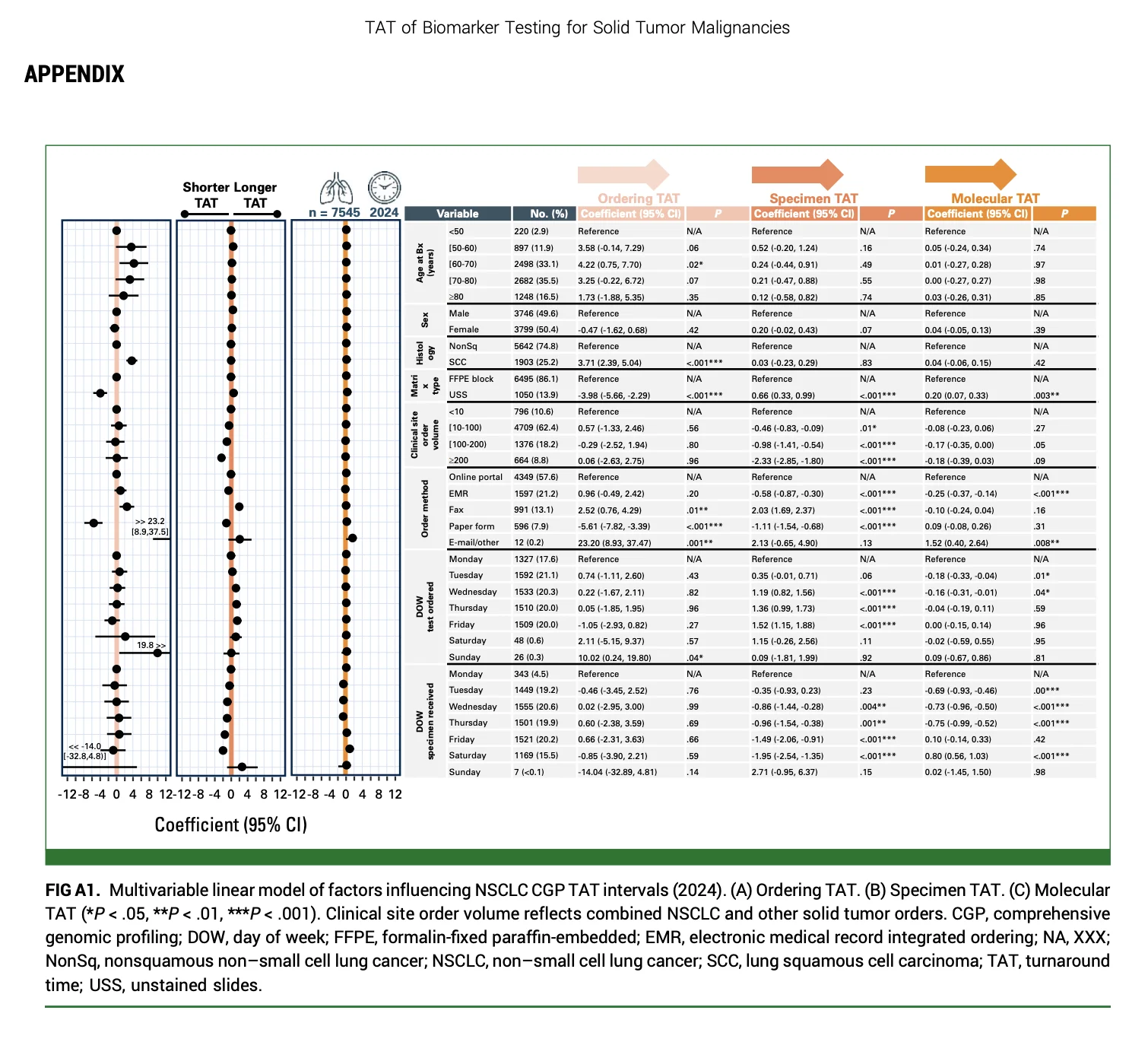
What Factors Were Linked to Faster Testing?
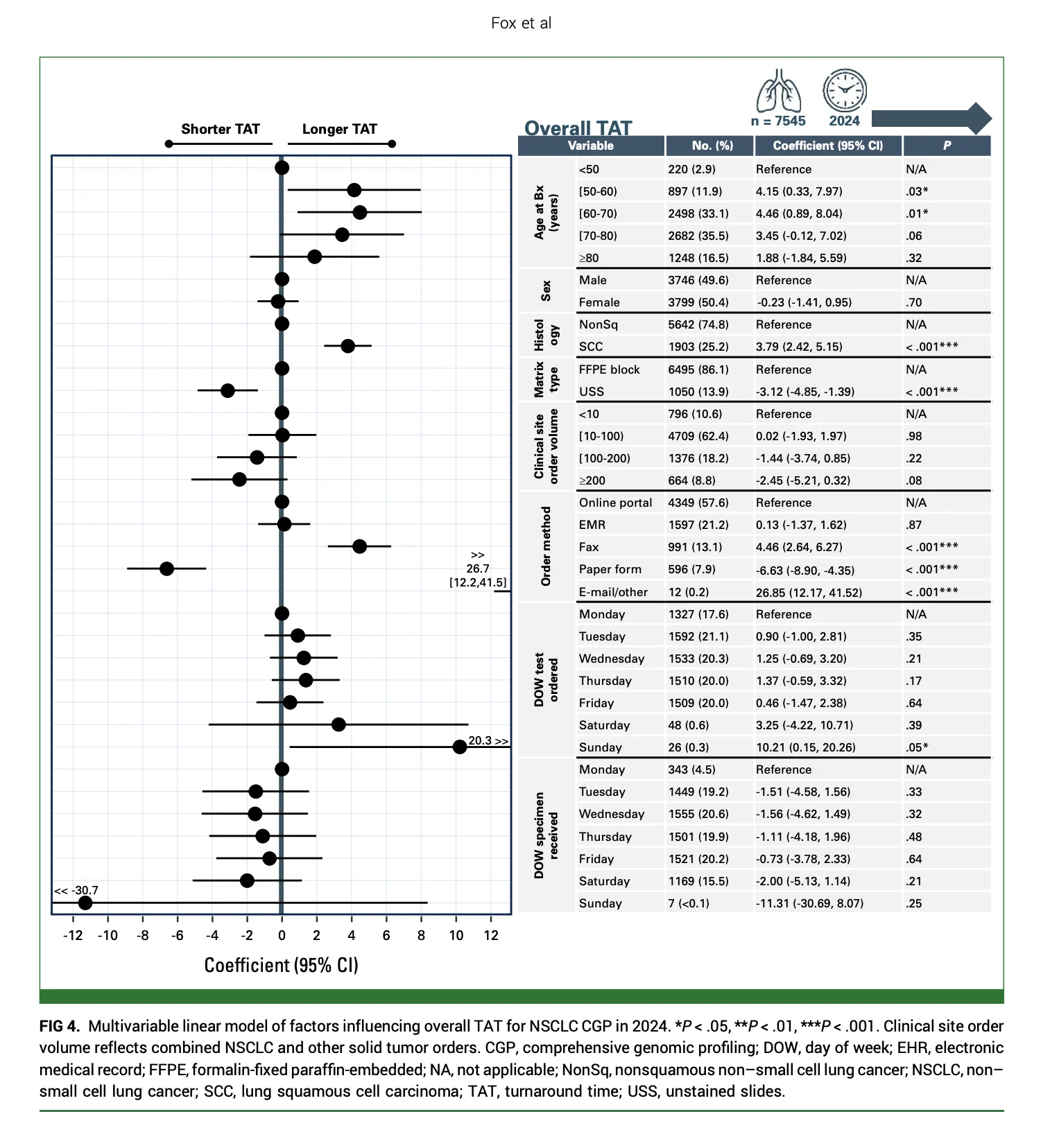
Several factors were associated with shorter turnaround time.
In the NSCLC cohort, younger patient age, nonsquamous histology, testing of unstained slides, higher clinical site ordering volume, and ordering method were associated with shorter overall TAT.
Ordering through an electronic health record, online portal, or paper form was associated with shorter TAT compared with fax orders.
Fax and email or other manual processes were associated with longer delays.
This finding is practical.
Precision oncology is not only a scientific issue. It is also a workflow issue.
Electronic ordering, clear responsibility for test initiation, specimen tracking, pathology coordination, and high-volume familiarity with testing processes can all influence how quickly patients receive results.
NSCLC Was Faster Than Other Solid Tumors
In 2024, the median overall TAT for NSCLC was 27.0 days.
For other solid tumors, it was 33.5 days.
The difference was mainly driven by longer ordering TAT in non-NSCLC solid tumors.
In 2024, median ordering TAT was:
14.0 days for NSCLC
20.0 days for other solid tumors
The authors suggest that cancer type may influence urgency. Because NSCLC treatment often depends immediately on biomarker results, clinicians may prioritize testing more quickly than in some other malignancies.
Still, the delay remains clinically relevant even in lung cancer, where testing is already considered essential.
Reflex Testing May Help, but Implementation Is Not Simple
One potential solution is reflex testing.
Reflex testing means that molecular testing is automatically initiated based on predefined clinical and pathology criteria, rather than waiting for a treating oncologist to order it after the first consultation.
This can reduce the time between biopsy and final results.
The authors note that single-center reflex testing studies have reported shorter turnaround time and higher rates of biomarker-informed care.
However, reflex testing has barriers.
Cost is a major concern. Reflex testing also requires clear institutional agreement about which tumor types, stages, and specimens should trigger testing. It requires coordination between pulmonology, interventional radiology, pathology, oncology, surgery, radiation oncology, molecular laboratories, and administrative teams.
But the current study makes a strong case that clinical systems must address the ordering step.
Waiting for the first oncology visit to order CGP may be too slow for many patients.

The Patient Experience Is Often Longer Than the Measured Timeline
The study measured turnaround time from specimen collection to report.
But for patients, the waiting period often begins earlier.
It may begin when an abnormal scan is found, when cancer is suspected, or when a biopsy is scheduled.
This means the real-world patient experience of waiting for a treatment plan may be longer than the measured CGP turnaround time.
The authors also note that the study did not include plasma-based CGP, which can sometimes provide faster results and may complement tissue testing.
This is important because tissue-based testing can be affected by specimen adequacy, tissue transfer, pathology processing, and send-out logistics.
A combined tissue-plus-plasma strategy may be useful in selected patients when rapid treatment decisions are needed, but this study focused only on tissue-based CGP.
Study Limitations
The study has important limitations.
The data came from a single commercial laboratory, so the findings may not fully apply to other laboratories, in-house testing platforms, or different institutional workflows.
Only completed tissue-based CGP tests were included. Plasma-based testing was not analyzed.
The study did not include detailed patient-centered timing, such as time from imaging detection to biopsy or time from diagnosis to treatment initiation.
It also lacked granular institutional details, including whether sites used reflex testing, how pathology workflows were organized, and how insurance or stage affected timing.
The study also does not directly show that longer CGP turnaround time caused worse outcomes.
Still, the size and national scope of the dataset make the findings difficult to ignore.

What This Means for Lung Cancer Programs
The study points to a practical quality-improvement target.
Cancer centers should measure their own CGP turnaround time by step:
How long from biopsy to test order?
How long from order to specimen shipment?
How long from specimen receipt to molecular report?
How long from report to treatment decision?
Without this breakdown, delays may be blamed on the laboratory when the main bottleneck is actually the ordering process.
For lung cancer programs, the findings support earlier biomarker testing workflows, pathologist-initiated or protocol-based reflex testing, electronic ordering, specimen tracking, multidisciplinary ownership, and rapid communication between diagnostic and treatment teams.
The goal is not simply to order more tests.
The goal is to make sure the right test is ordered early enough to guide the first treatment decision.
The Bottom Line
This large U.S. analysis shows that tissue-based comprehensive genomic profiling turnaround time has improved, but delays remain substantial.
For NSCLC in 2024, the median overall turnaround time was 27.0 days.
The largest contributor was the time from biopsy to CGP order, with a median of 14.0 days.
Molecular laboratory processing was faster and more stable, with a median of 7.1 days.
The message for lung cancer care is direct: precision oncology cannot depend only on better tests.
It needs better systems.
For patients with lung cancer, the clock starts before the sequencing run begins.
References
- Fox AH, Keller-Evans RB, Huang RSP, Silvestri GA. Turnaround time of comprehensive genomic profiling in lung cancer and other solid tumors. JCO Oncology Practice. Published June 18, 2026. doi:10.1200/OP-25-01191.
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Non-Small Cell Lung Cancer. Version 2.2025.
- Mok T, Camidge DR, Gadgeel SM, et al. Updated overall survival and final progression-free survival data for patients with treatment-naive advanced ALK-positive non-small-cell lung cancer in the ALEX study. Annals of Oncology. 2020;31:1056–1064.
- Forde PM, Spicer J, Lu S, et al. Neoadjuvant nivolumab plus chemotherapy in resectable lung cancer. New England Journal of Medicine. 2022;386:1973–1985.
- Wu YL, Tsuboi M, He J, et al. Osimertinib in resected EGFR-mutated non-small-cell lung cancer. New England Journal of Medicine. 2020;383:1711–1723.
- Lu S, Kato T, Dong X, et al. Osimertinib after chemoradiotherapy in stage III EGFR-mutated NSCLC. New England Journal of Medicine. 2024;391:585–597.
- Roy-Chowdhuri S, Mani H, Fox AH, et al. The American Cancer Society National Lung Cancer Roundtable strategic plan: methods for improving turnaround time of comprehensive biomarker testing in non-small cell lung cancer. Cancer. 2024;130:4200–4212.
- Gosney JR, Paz-Ares L, Jänne P, et al. Pathologist-initiated reflex testing for biomarkers in non-small-cell lung cancer: expert consensus on rationale and implementation. ESMO Open. 2023;8:101587.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}