


At the 2026 ASCO Annual Meeting, Bas Groot Koerkamp, MD, PhD, from Erasmus MC Cancer Institute, presented results from the PUMP trial, a randomized phase 3 study evaluating adjuvant hepatic arterial infusion pump chemotherapy with floxuridine in patients with resectable colorectal liver metastases and a low clinical risk score.

You can also read about Results From the PUMP-2 Trial on OncoDaily.
Background
Recurrence after local treatment for colorectal liver metastases occurs in up to 70% of patients, and around 50% recur in the liver. Dutch national guidelines do not recommend adjuvant chemotherapy after colorectal liver metastasis resection, as previous randomized trials have not shown an overall survival benefit with perioperative systemic chemotherapy in this setting.
Hepatic arterial infusion pump chemotherapy delivers floxuridine directly to the liver. The PUMP trial evaluated whether adjuvant HAIP chemotherapy with floxuridine could improve outcomes compared with resection alone in patients with resectable colorectal liver metastases and a low clinical risk score.
Study Design
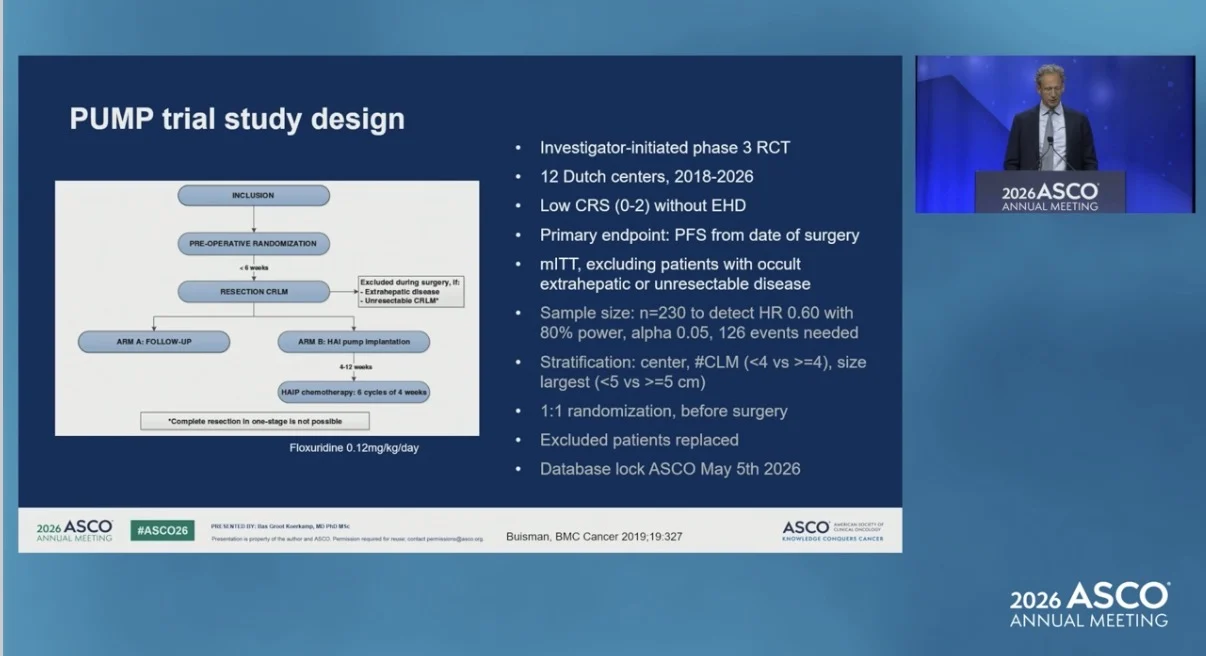
The PUMP trial was an investigator-initiated, multicenter, randomized phase 3 trial conducted across 12 Dutch centers between 2018 and 2026. Patients with resectable colorectal liver metastases, no extrahepatic disease, and a clinical risk score of 0–2 were randomized 1:1 before surgery to resection followed by adjuvant HAIP chemotherapy with floxuridine or resection alone.
Both groups received no adjuvant systemic chemotherapy. Preoperative systemic chemotherapy before randomization was allowed. Patients assigned to the HAIP group were scheduled to receive 6 cycles of floxuridine chemotherapy at 0.12 mg/kg/day after placement of a subcutaneous pump. The primary endpoint was progression-free survival from the date of surgery. Secondary endpoints included hepatic progression-free survival, overall survival, and 90-day mortality.

Results
A total of 241 patients were randomized. After exclusion of patients with occult extrahepatic disease, unresectable colorectal liver metastases, or benign liver lesions at surgery, 220 patients were included in the modified intention-to-treat analysis: 111 in the resection plus HAIP group and 109 in the resection-alone group. In the HAIP group, 108 of 111 patients, or 97%, had a pump placed, and 100 of 111 patients, or 90%, started HAIP chemotherapy. The median number of administered cycles was 5, with an interquartile range of 4 to 6 cycles. Overall, 45 patients, or 41%, completed all 6 scheduled cycles.
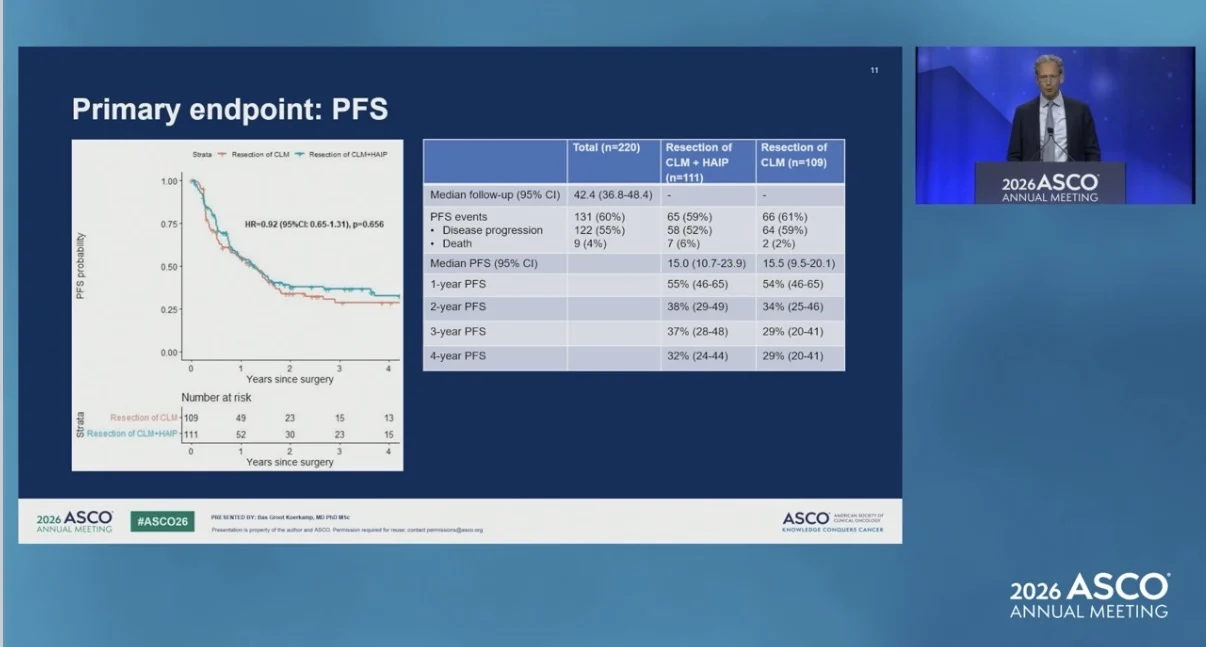
Median progression-free survival was 15.0 months in the HAIP group and 15.5 months in the resection-alone group. The hazard ratio was 0.92, with a 95% confidence interval of 0.65 to 1.31, and a p value of 0.656.

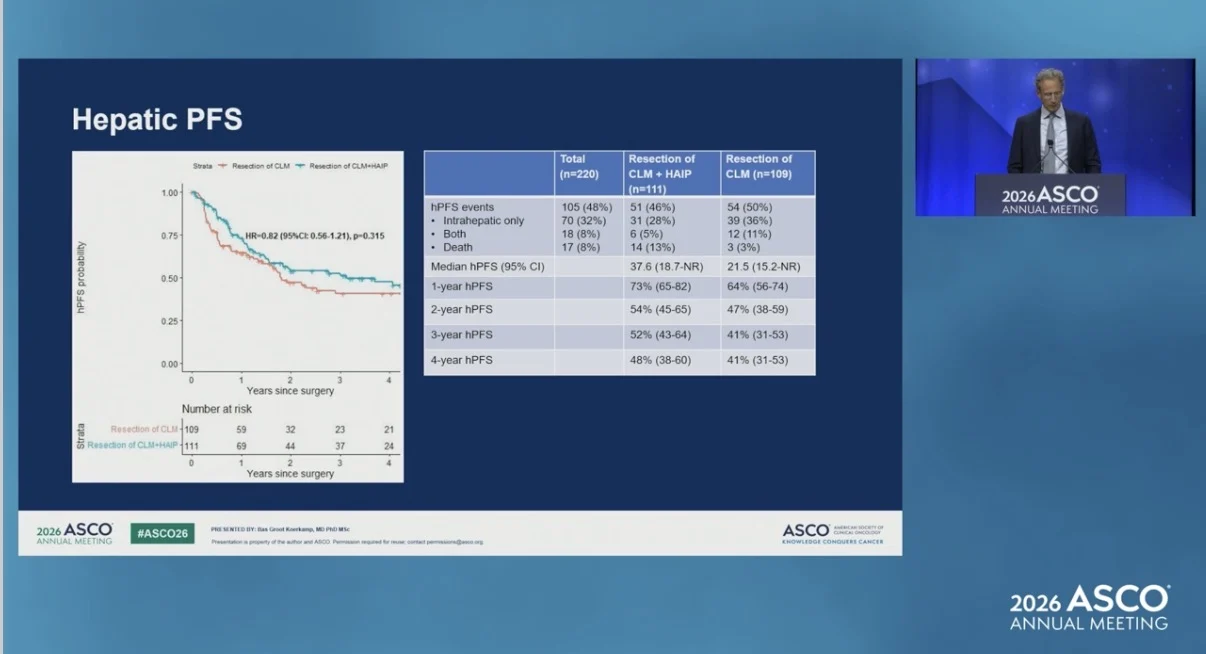
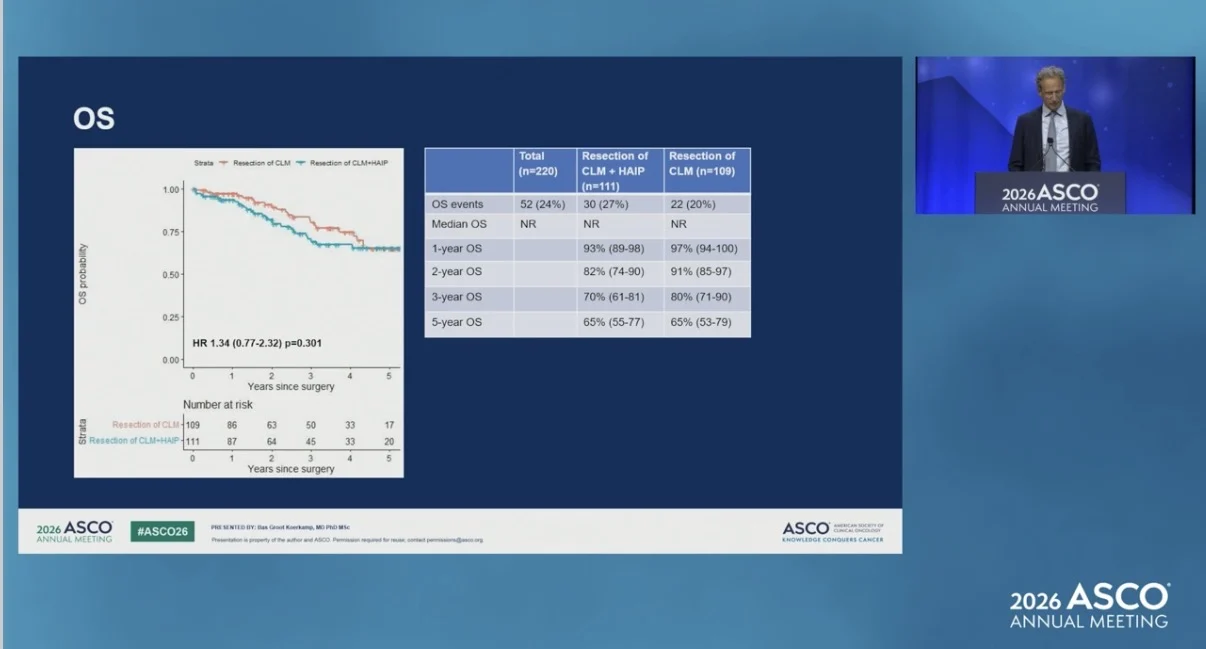
Median hepatic progression-free survival was 37.6 months with HAIP chemotherapy and 21.5 months with resection alone. The hazard ratio was 0.82, with a 95% confidence interval of 0.56 to 1.21, and a p value of 0.315. Median overall survival was not reached in either group. The overall survival hazard ratio was 1.34, with a 95% confidence interval of 0.77 to 2.32, and a p value of 0.301.

Safety and Mortality
Ninety-day postoperative mortality occurred in 4 patients, or 3.6%, in the HAIP group and in 1 patient, or 0.9%, in the resection-alone group. No treatment-related mortality was reported.
HAIP-related grade 3 complications occurred in 19 patients, or 17%. These included pocket infection, pump dysfunction, catheter-pump dislodgement, catheter-artery dislodgement, arterial dissection, hepatic artery thrombosis, bowel strangulation by catheter, and biliary sclerosis.
Conclusion
In patients with resectable colorectal liver metastases and a low clinical risk score, adjuvant hepatic arterial infusion pump chemotherapy with floxuridine did not improve progression-free survival compared with resection alone. HAIP placement and chemotherapy were feasible in a Dutch multicenter setting, with low complication rates and no treatment-related mortality.

The study suggests that future research on adjuvant intra-arterial treatment should focus on better patient selection and additional drugs for intra-arterial delivery.
The study was registered under EudraCT number 2018-001696-21.
The full abstract is available on the official ASCO website.

Read more about BREAKWATER at ASCO 2026 on OncoDaily.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}