


Breast cancer incidence is increasing rapidly among Asian American, Native Hawaiian, and Pacific Islander women in the United States, with especially concerning trends in early-onset disease, distant-stage diagnosis, and aggressive molecular subtypes.
A new population-based study published in JAMA Network Open examined invasive breast cancer incidence trends from 2000 to 2022 across disaggregated Asian American, Native Hawaiian, and Pacific Islander ethnic groups.
The study included 148,608 Asian American, Native Hawaiian, and Pacific Islander females diagnosed with invasive breast cancer using National Cancer Institute SEER Program data from 14 US states.
The findings challenge the older assumption that breast cancer incidence is uniformly lower among Asian American populations. They also show why grouping Asian American, Native Hawaiian, and Pacific Islander communities into one category can hide important differences in risk, stage, and subtype.
Why This Study Matters
Asian American, Native Hawaiian, and Pacific Islander populations include more than 40 ethnic groups, with different immigration histories, cultures, health care access patterns, reproductive factors, diets, socioeconomic profiles, and screening barriers.
Yet cancer statistics often report them as one combined group.
That approach can obscure clinically meaningful differences.
In this study, the authors examined 7 Asian American groups and 2 Native Hawaiian or Pacific Islander groups:
Asian Indian or Pakistani, Chinese, Filipino, Japanese, Korean, Laotian or Kampuchean, Vietnamese, Guamanian, Chamorro, Samoan, and Native Hawaiian populations.
This level of detail matters because breast cancer incidence varied widely across groups.
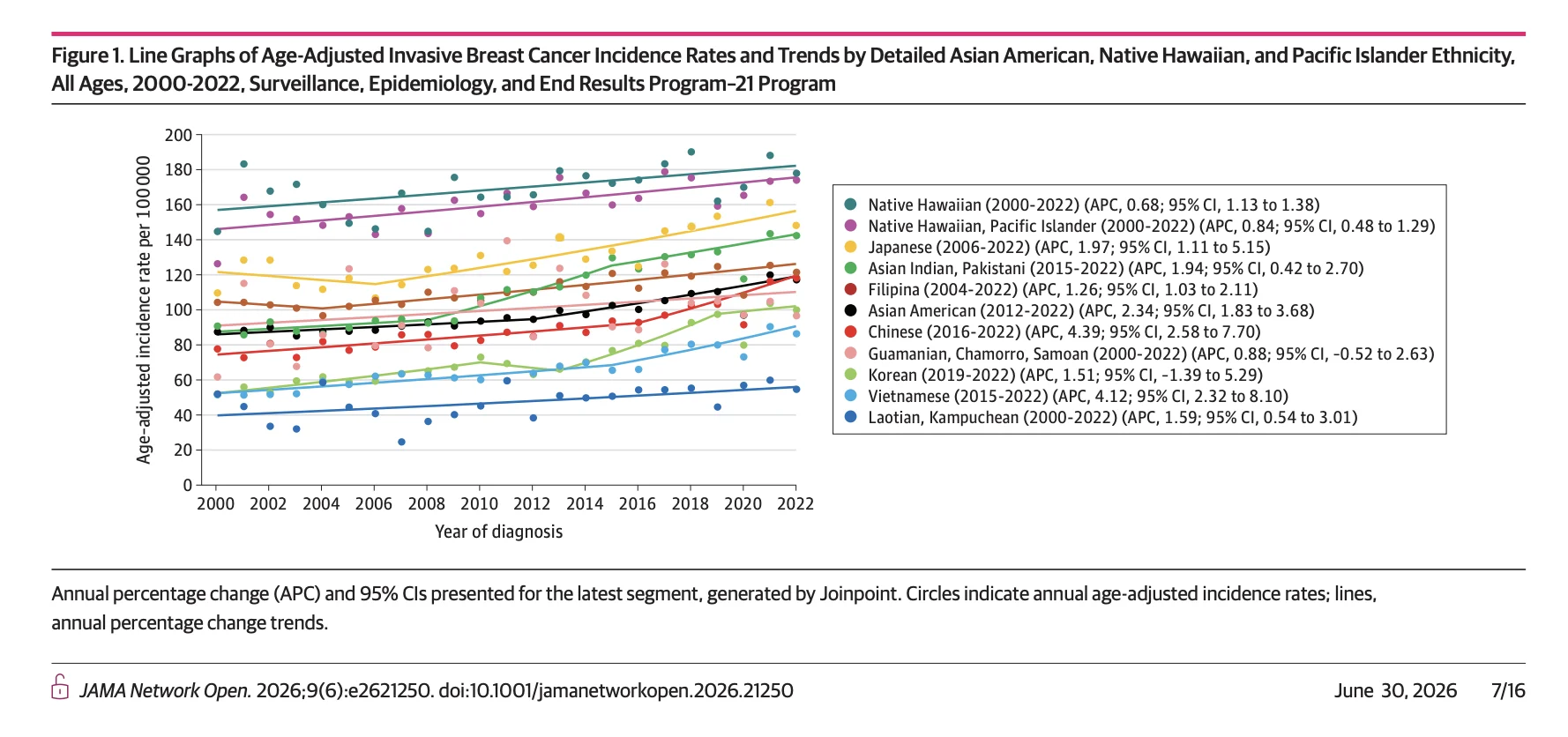
For 2018 to 2022, age-adjusted incidence rates ranged from 54.1 per 100,000 among Laotian or Kampuchean females to 177.2 per 100,000 among Native Hawaiian females.
That is more than a threefold difference.
A Large SEER-Based Analysis
The study used SEER-21 data from 2000 to 2022, covering 14 states and approximately 66.4% of the Asian American, Native Hawaiian, and Pacific Islander population in the United States.
Among the 148,608 patients included:
- 44,234 were younger than 50 years at diagnosis
- 104,374 were aged 50 years or older
- 138,808 were Asian American
- 9,800 were Native Hawaiian or Pacific Islander
Overall, 63.9% were diagnosed with localized-stage disease, and 66.6% had hormone receptor-positive, ERBB2-negative breast cancer.
The investigators evaluated trends by age, stage, and breast cancer subtype using joinpoint regression.
Asian American Women Had the Fastest Recent Increase
From 2012 to 2022, breast cancer incidence among Asian American females increased by 2.34% per year.
This rise surpassed trends seen in other racial and ethnic groups.
Native Hawaiian and Pacific Islander females also had a steady increase from 2000 to 2022, with an annual percentage change of 0.84%.
The most rapid recent increases were seen in several Asian American groups.
Among Chinese females, incidence increased by 4.39% per year from 2016 to 2022.
Among Vietnamese females, incidence increased by 4.12% per year from 2015 to 2022.
Among Asian Indian and Pakistani females, incidence increased by 4.17% per year from 2008 to 2015, followed by a slower but still significant increase of 1.94% per year thereafter.
These trends suggest that the rise is not limited to one community or one age group.
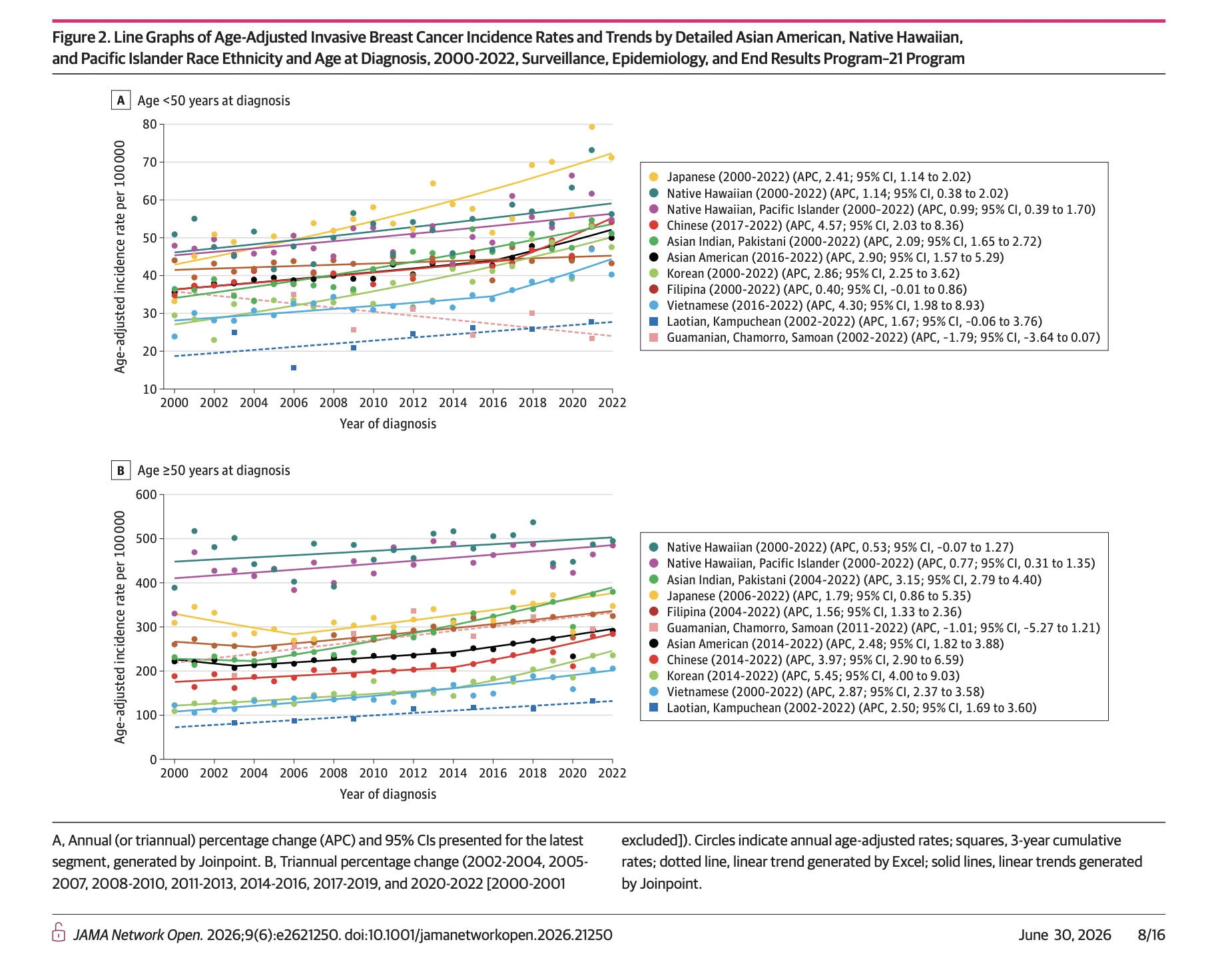
Early-Onset Breast Cancer Is a Major Warning Signal
One of the most concerning findings was the increase in breast cancer diagnosed before age 50.
Among Asian American, Native Hawaiian, and Pacific Islander females younger than 50 years, incidence increased by approximately 2.90% per year from 2016 to 2022.
By 2021 and 2022, early-onset breast cancer incidence in the aggregated Asian American, Native Hawaiian, and Pacific Islander population became comparable with the rate among non-Hispanic White females.
Several groups showed particularly steep early-onset increases:
- Chinese females had an annual percentage change of 4.57% from 2017 to 2022.
- Vietnamese females had an annual percentage change of 4.30% from 2016 to 2022.
- Korean females had an annual percentage change of 2.86% from 2000 to 2022.
- Asian Indian and Pakistani females had an annual percentage change of 2.09% from 2000 to 2022.
Japanese females had an annual percentage change of 2.41% from 2000 to 2022.
These findings are important because breast cancer screening policies and risk prediction models may not fully capture risk patterns in younger Asian American, Native Hawaiian, and Pacific Islander women.

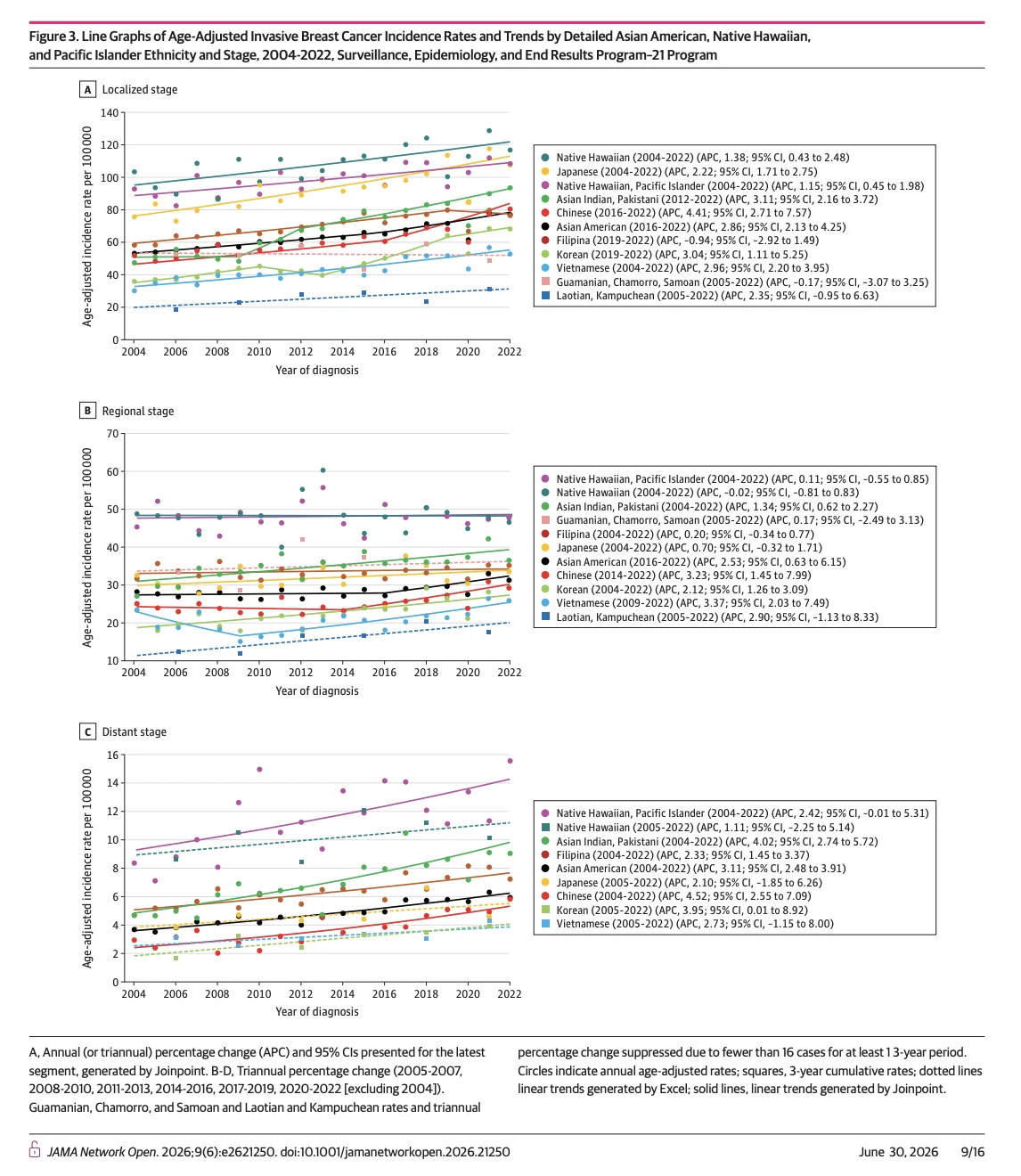
Distant-Stage Disease Is Also Increasing
The study also found increases across localized, regional, and distant-stage disease.
This is important because a rise only in localized disease could suggest more screening and earlier detection.
But the increase in distant-stage disease suggests that the trend cannot be explained by screening alone.
Among Asian American, Native Hawaiian, and Pacific Islander females overall, distant-stage breast cancer increased by 3.04% per year from 2004 to 2021.
Several Asian American groups had significant increases in distant-stage disease:
- Asian Indian and Pakistani females: 4.02% per year
- Chinese females: 4.52% per year
- Filipina females: 2.33% per year
- Korean females: 3.95% per 3 years
The increase in distant-stage disease raises concern about delayed diagnosis, screening gaps, barriers to follow-up after abnormal imaging, or underlying shifts in disease biology and risk factors.
HR-Positive, ERBB2-Negative Disease Remains Common
Hormone receptor-positive, ERBB2-negative breast cancer remained the most common subtype.
All Asian American groups except Laotian and Kampuchean females had increasing trends in HR-positive, ERBB2-negative breast cancer.
The largest increases were seen among:
- Korean females: 6.00% per year from 2010 to 2022
- Vietnamese females: 5.01% per year from 2010 to 2022
- Chinese females: 4.04% per year from 2010 to 2022
- Asian Indian and Pakistani females: 3.61% per year from 2010 to 2022
These patterns may reflect changing reproductive, metabolic, environmental, and lifestyle risk factors, but the authors emphasize that more research is needed to understand the drivers.

Triple-Negative Breast Cancer Is Rising in Several Groups
The study also found increases in triple-negative breast cancer, an aggressive subtype with fewer targeted treatment options than hormone receptor-positive disease.
Among Asian American, Native Hawaiian, and Pacific Islander females overall, TNBC incidence increased by 4.35% per year from 2016 to 2022.
Nearly all Asian American groups experienced increases in TNBC.
The largest increases included:
- Chinese females: 6.17% per year from 2017 to 2022
- Filipina females: 4.00% per year from 2016 to 2022
- Vietnamese females: 3.86% per year from 2010 to 2022
- Asian Indian and Pakistani females: 3.06% per year from 2010 to 2022
This is clinically important because rising TNBC incidence may have future implications for mortality, treatment needs, genetic counseling, clinical trial enrollment, and community-level awareness.
Native Hawaiian Women Had the Highest Incidence
Native Hawaiian females had the highest overall incidence rate among the groups studied.
From 2018 to 2022, the incidence rate among Native Hawaiian females was 177.2 per 100,000.
The authors noted that this burden was consistently high across age, stage, and subtype.
Native Hawaiian females also had high rates of HR-positive, ERBB2-negative breast cancer, with a rate of 131.7 per 100,000.
The study notes that established breast cancer risk factors may not fully explain the elevated burden among Native Hawaiian females. Potential contributors may include early-life exposures, hormonal factors, cultural factors, and structural and social determinants of health.
Screening and Awareness Must Be Culturally Specific
The findings have practical implications for public health.
The authors highlight that breast cancer screening rates and follow-up after abnormal mammography may be lower among some Asian American, Native Hawaiian, and Pacific Islander groups compared with other populations.
Cultural stigma, language barriers, immigration-related barriers, insurance access, health literacy, and lack of culturally tailored outreach may all affect timely screening and diagnosis.
This study supports the need for breast cancer awareness and screening programs that are not only translated, but also culturally adapted for specific communities.
A single “Asian American” or “Pacific Islander” outreach strategy is not enough.

What This Study Cannot Prove
This was a descriptive, population-based cross-sectional study.
It shows incidence trends but does not prove why breast cancer rates are increasing.
The study also had limitations related to race and ethnicity classification, incomplete specificity for some Asian American and Pacific Islander subgroups, and possible underestimation of rates in defined ethnic categories because some cases were coded as not otherwise specified.
The SEER registries included approximately two-thirds of the Asian American, Native Hawaiian, and Pacific Islander population, so results may not fully represent every US region.
The authors also noted the potential influence of the COVID-19 pandemic on cancer incidence data, although 2020 rates were excluded from joinpoint analyses according to standard methods.
The Bottom Line
This JAMA Network Open study found rapid increases in invasive breast cancer incidence among Asian American, Native Hawaiian, and Pacific Islander women over more than two decades.
The increase was especially concerning for early-onset breast cancer, distant-stage disease, HR-positive and ERBB2-negative breast cancer, and triple-negative breast cancer.
The findings call for more detailed research into distinct Asian American, Native Hawaiian, and Pacific Islander populations, rather than relying on broad aggregated categories.
They also point to an urgent need for culturally and linguistically tailored screening, awareness, and follow-up strategies.
For breast cancer prevention and early detection, disaggregation is not just a data issue.
It is a clinical equity issue.
References
- Gomez SL, McKinley M, Chan M, Lin K, Yu M, Scoppa S, Gibson T, Miyagi K, Hernandez BY, Noone AM, Kurian A, Cheng I, Shariff-Marco S. Breast cancer incidence in Asian American, Native Hawaiian, and Pacific Islander populations, 2000-2022. JAMA Network Open. 2026;9(6). doi:10.1001/jamanetworkopen.2026.21250.
- Sherman RL, Firth AU, Henley SJ, et al. Annual report to the nation on the status of cancer, featuring state-level statistics after the onset of the COVID-19 pandemic. Cancer. 2025;131(9). doi:10.1002/cncr.35833.
- Sung H, Rosenberg PS, Chen WQ, et al. Female breast cancer incidence among Asian and Western populations: more similar than expected. Journal of the National Cancer Institute. 2015;107(7). doi:10.1093/jnci/djv107.
- Tuan AW, Davis Lynn BC, Chernyavskiy P, et al. Breast cancer incidence trends by estrogen receptor status among Asian American ethnic groups, 1990-2014. JNCI Cancer Spectrum. 2020;4(2). doi:10.1093/jncics/pkaa005.
- Li NHY, Li CI. Incidence rate trends of breast cancer overall and by molecular subtype by race and ethnicity and age. JAMA Network Open. 2025;8(1). doi:10.1001/jamanetworkopen.2024.56142.
- Sohn YJ, Chang CY, Miles RC. Current gaps in breast cancer screening among Asian and Asian American women in the United States. Journal of the American College of Radiology. 2021;18(10):1376-1383. doi:10.1016/j.jacr.2021.06.002.
- Chawla N, Breen N, Liu B, Lee R, Kagawa-Singer M. Asian American women in California: a pooled analysis of predictors for breast and cervical cancer screening. American Journal of Public Health. 2015;105(2). doi:10.2105/AJPH.2014.302250.
- Nguyen KH, Pasick RJ, Stewart SL, Kerlikowske K, Karliner LS. Disparities in abnormal mammogram follow-up time for Asian women compared with non-Hispanic White women and between Asian ethnic groups. Cancer. 2017;123(18):3468-3475. doi:10.1002/cncr.30756.
{kind=link}
{kind=link}
{kind=link}