


Shankar Siva, Radiation Oncologist at the Peter MacCallum Cancer Centre, shared a post on X:
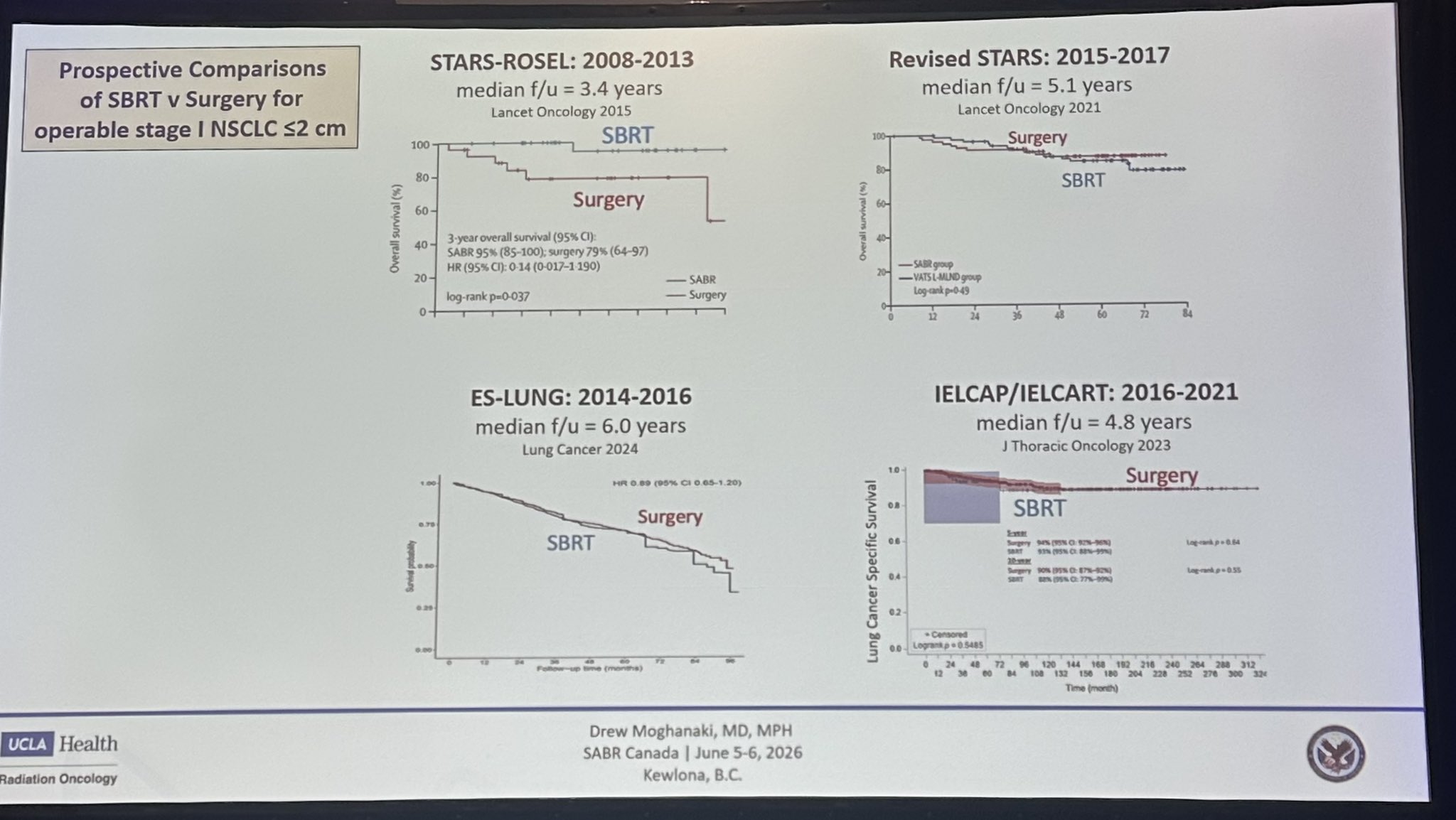
“Drew Moghanaki’s ‘Possibility VALOR phIII RCT of surgery vs SABR will show no difference in stage I lung cancer’ at SABR 2025
Several studies show no diff
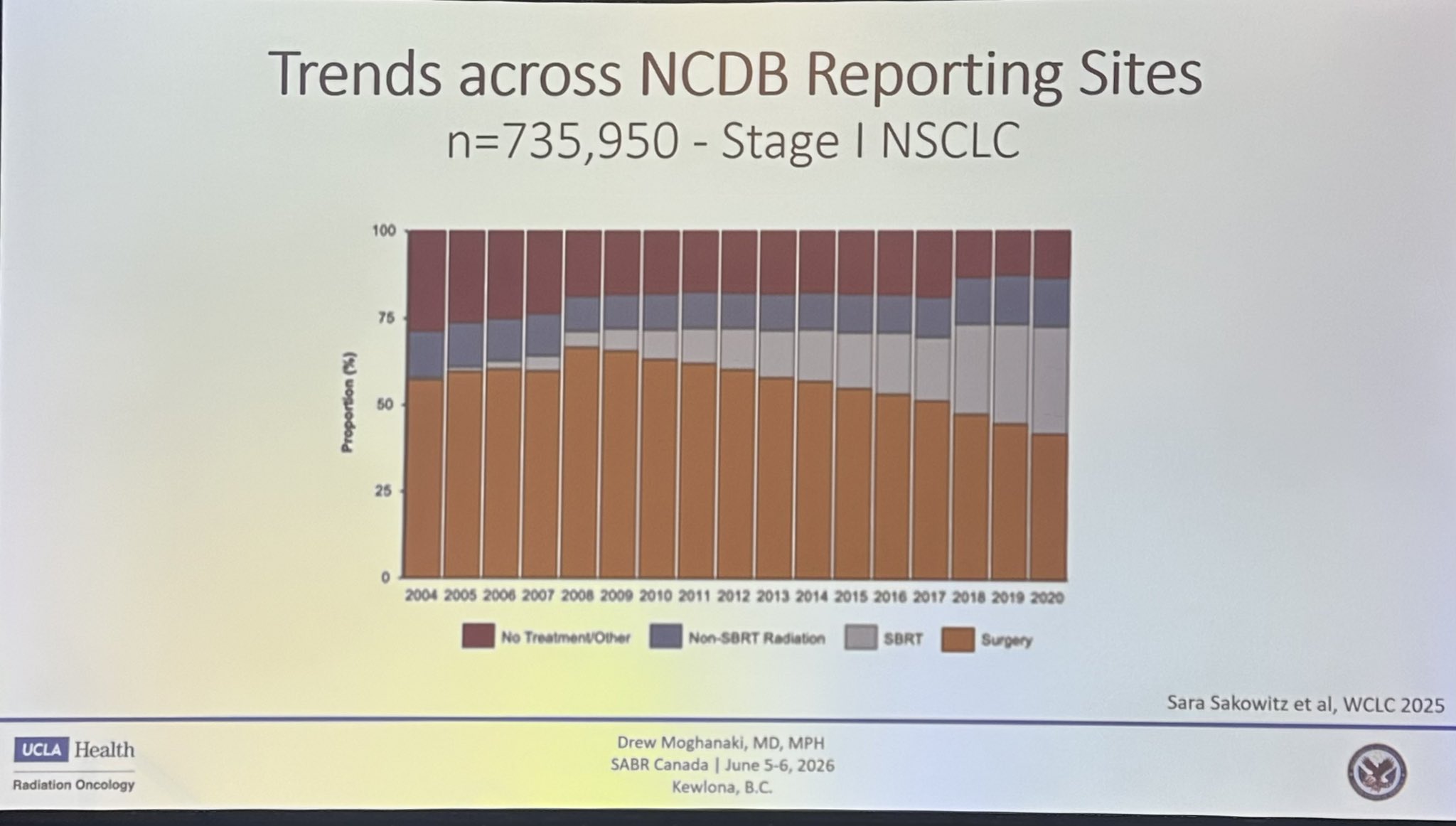
Trends for surgery in the US
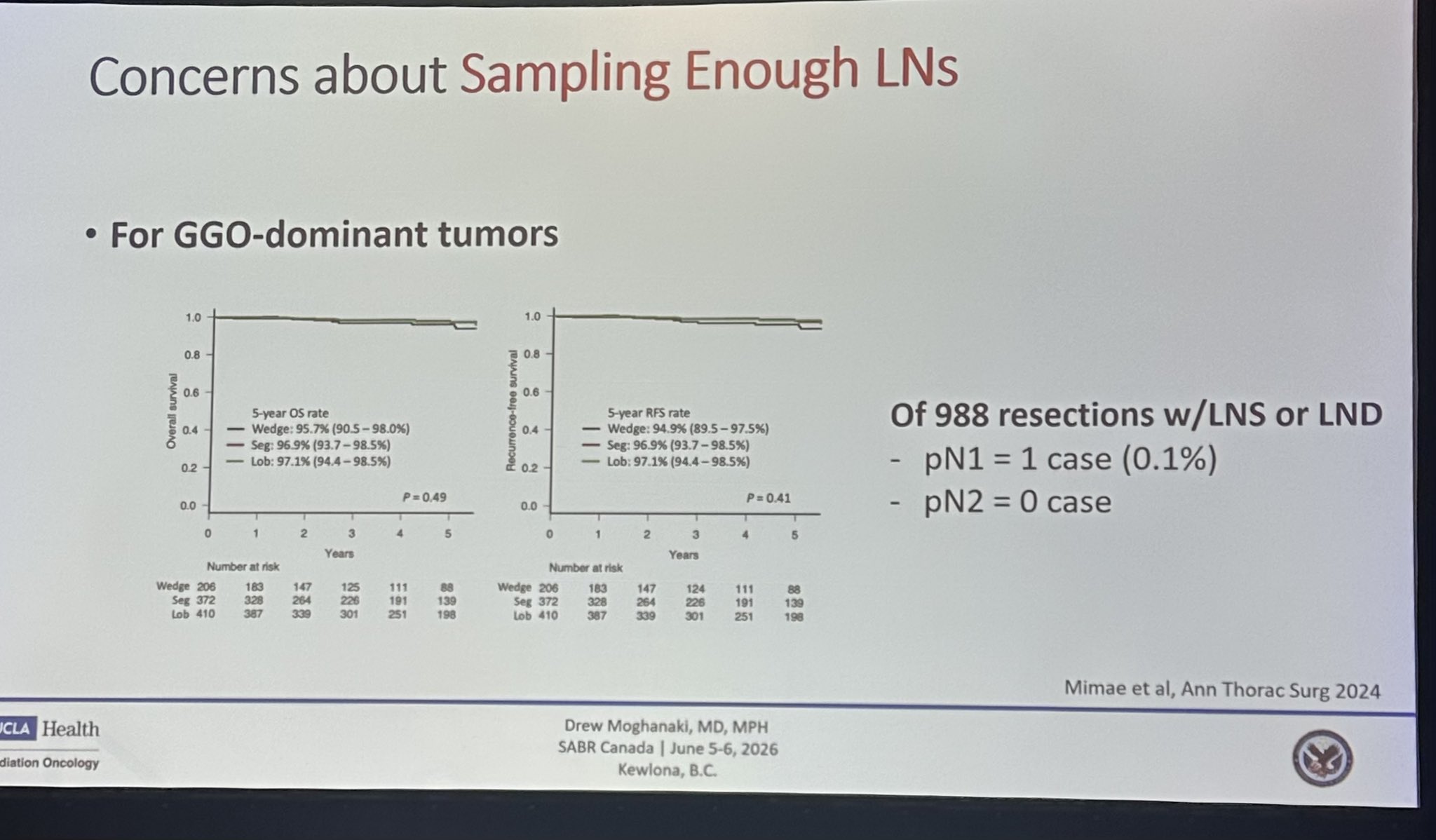
Sampling LNs in solid dom GGO are not needed
Benefit of lobectomy, Nasser Altorki.”
Biniam Kidane, Thoracic Surgeon and Associate Professor at the University of Manitoba, shared this post, adding:
“I’ll admit freely that I’ve always been biased towards SBRT and organ preservation because of this type of utility-based framework. I’ve spent a lot of time talking to patients about these complex decisions in the context of clinical care and unique collaborative trials. Thread on what I’ve learned.
Prior to SABR-BRIDGE, my assumption had been that SBRT is always highly tolerable and has fewer complications than surgery. Following all these patients long-term (all of whom were resectable/operable) in tandem with my surgical patients has taught me that my assumptions are not universally true.
Central to the idea of the trade-off framework to weigh risks and benefits is that all the inputs must be accurate. A lot of the risks of ‘thoracotomy’ are as historical and overstated as the term itself. The reality is that surgical techniques and outcomes have evolved substantially and so should our risk estimates. As a surgical community, we have tried to improve both reporting and outcomes.
The Society of Thoracic Surgeons, ESTS, and Canadian Association of Thoracic Surgeons databases are prime examples.
In my case, I knew very well what the complication risk/profile was for surgery, but not so much for SBRT, so I always strongly suggest that patients hear about it from my radonc colleagues. I think we need this kind of collaborative data input into the trade-off framework.
Fast forward 5 years after SABR BRIDGE, I was surprised about some of the QOL issues patients were having that we never saw with surgery.
This has changed my perspective. In patients with small peripheral lung cancers, uniportal sublobar resection can be done as a day surgery and likely has less medium to long-term pain than even SF SBRT
I would never have thought this prior to following all these patients. Our patients teach us. The more we listen, the better we will do. The more we listen together, the best we will do!
Good segue into OPERA RADIO, which shows that surgical context matters. This is a trial developed with my radonc and med onc colleagues, Julian Kim, Shantanu Banerji. It was a purely patient-driven question. We used organ-preserving ESD followed by radiotherapy and ICI in patients who were ineligible for or who declined esophagectomy.
Avoiding surgery and organ preservation have increasing utility for patients and health systems as the morbidity of the surgery rises.
Being able to avoid esophagectomy or APR with TNT or SANO or OPERA RADIO comes with some inherent risks of reduced overall long-term survival, but as Ralph Weichselbaum aptly said, more people tend to choose organ preservation when taking a cold, hard look at the trade-offs.
I honestly don’t think this is the case with lung surgery vs radiation-based therapies for resectable lung cancer…and my position on the matter is informed by patient-centered utilities rather than necessarily the assumption that surgery is always better.”
Shankar Siva shared these posts, answering on Biniam’s comment:
“Hi Biniam Kidane – you are talking about lived experiences with patients having two curative treatments, and comparing them to your lived experience of patients having surgery alone. Are you sure this reflects outcomes of SABR vs surgery? The decision regret algorithms that started this thread were not designed to deal with combination treatments… and honestly, it would be truly surprising if a general anaesthetic and major surgery would be less toxic than outpatient 1-3 visits of SABR.”
More posts featuring Shankar Siva.
{kind=link}
{kind=link}
{kind=link}
{kind=link}