


Updated results from the phase 3 SUNMO (NCT05171647), evaluating Mosun-Pola vs R-GemOx in R/R Large B-cell lymphoma, were presented by L. Elizabeth Budde.
At the primary analysis, Mosun-Pola demonstrated superiority over R-GemOx, including improved response rates and PFS, alongside infrequent low-grade CRS events. Here, longer follow-up findings are reported, including analyses in the second-line and third-line or later subgroups.
Clinical Context
Large B-cell lymphoma is the most common aggressive non-Hodgkin lymphoma. Patients with R/R LBCL who are unable to undergo potentially curative approaches such as CAR T-cell therapy or ASCT continue to have poor outcomes. While salvage regimens such as R-GemOx can induce responses, durability of benefit remains limited.
The combination of mosunetuzumab, a CD20×CD3 BsAb, and polatuzumab vedotin, a CD79b-directed ADC, represents a chemotherapy-free strategy that targets malignant B cells through complementary mechanisms.
SUNMO Study Design
ASCT-ineligible patients were randomized 2:1 to receive either subcutaneous Mosun-Pola or R-GemOx. At the August 8, 2025 data cutoff, 208 patients had been enrolled, including 91 treated in the 2L and 117 in the 3L+ setting. A total of 138 patients were assigned to Mosun-Pola and 70 to R-GemOx. Baseline characteristics were generally balanced between treatment arms within both treatment-line subgroups.
DLBCL represented the predominant histology (~78-80%), with HGBCL accounting for approximately 18-23% of cases. Most patients had advanced-stage disease (Ann Arbor stage III-IV), and more than half had primary refractory disease. Refractoriness to the last prior therapy was particularly common in the 3L+ subgroup. Bulky disease (≥10 cm) and ECOG PS 2 were observed more frequently in the Mosun-Pola arm.
Dual primary endpoints included independent review committee-assessed PFS and objective response rate. Secondary endpoints included CR rate, DOR, DOCR, and safety outcomes.
Results
After a median follow-up of 28.3 months, Mosun-Pola continued to demonstrate durable improvements:
- Median PFS improved from 3.8 months with R-GemOx to 11.6 months with Mosun-Pola (HR 0.41; 95% CI 0.28-0.60)
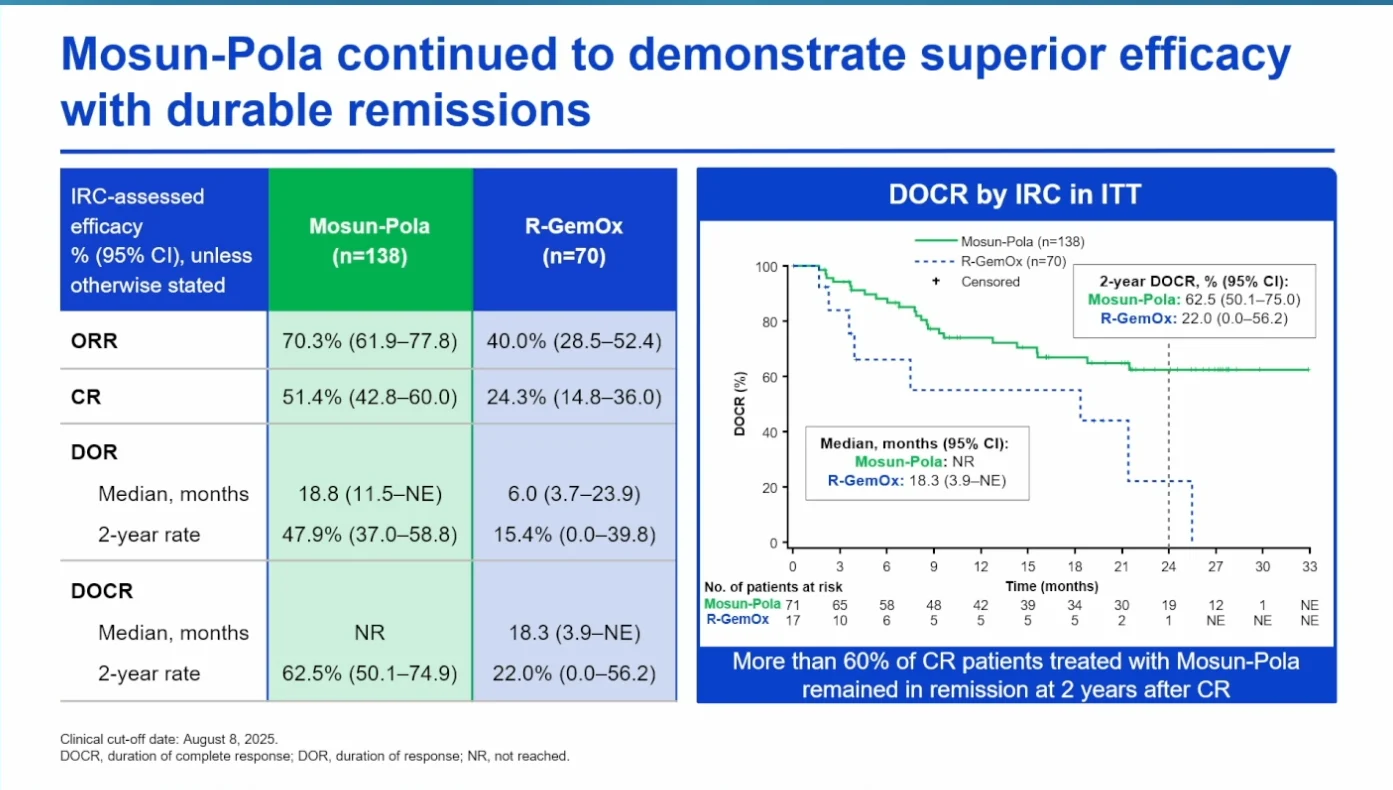
- Objective response rate increased from 40.0% to 70.3%
- Complete response rates more than doubled: 24.3% to 51.4%

Outcomes by Treatment Line
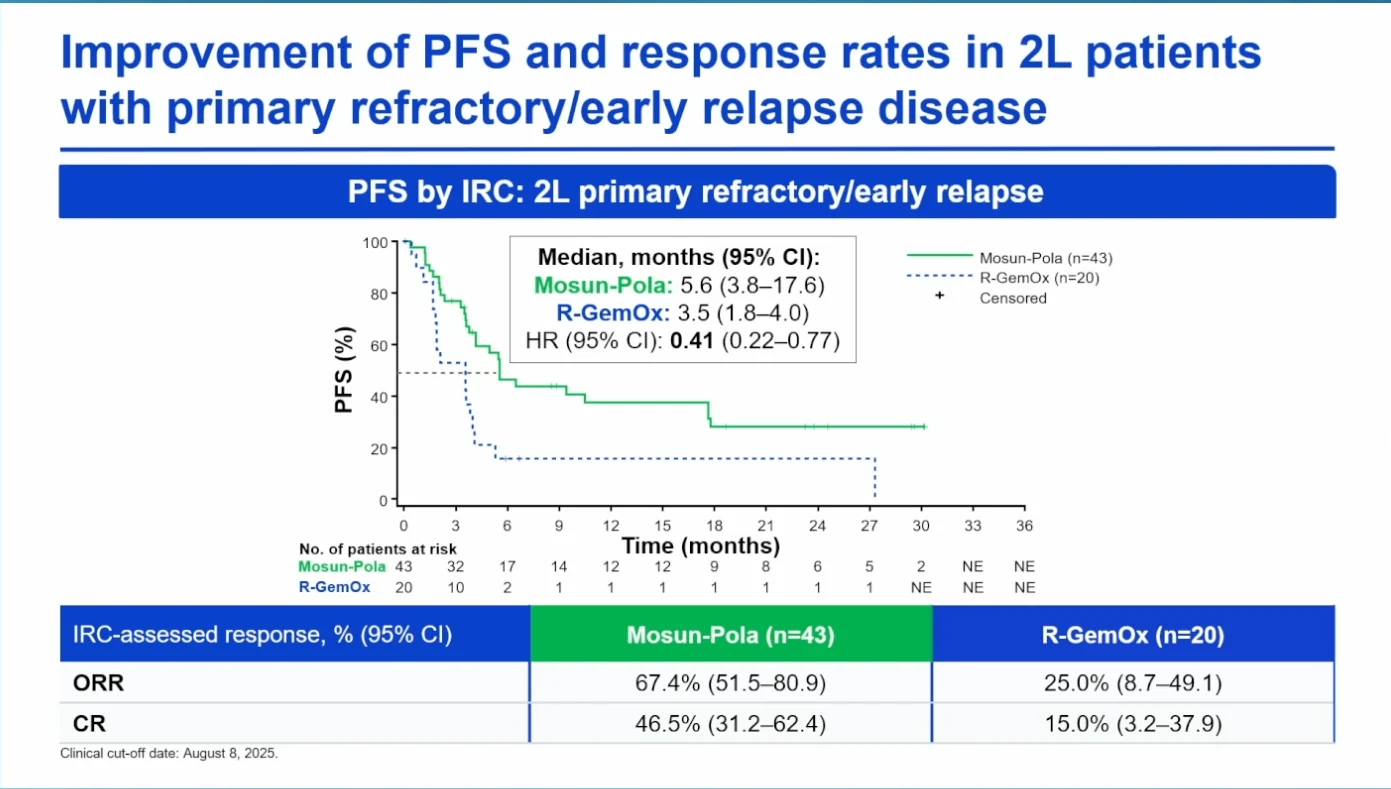
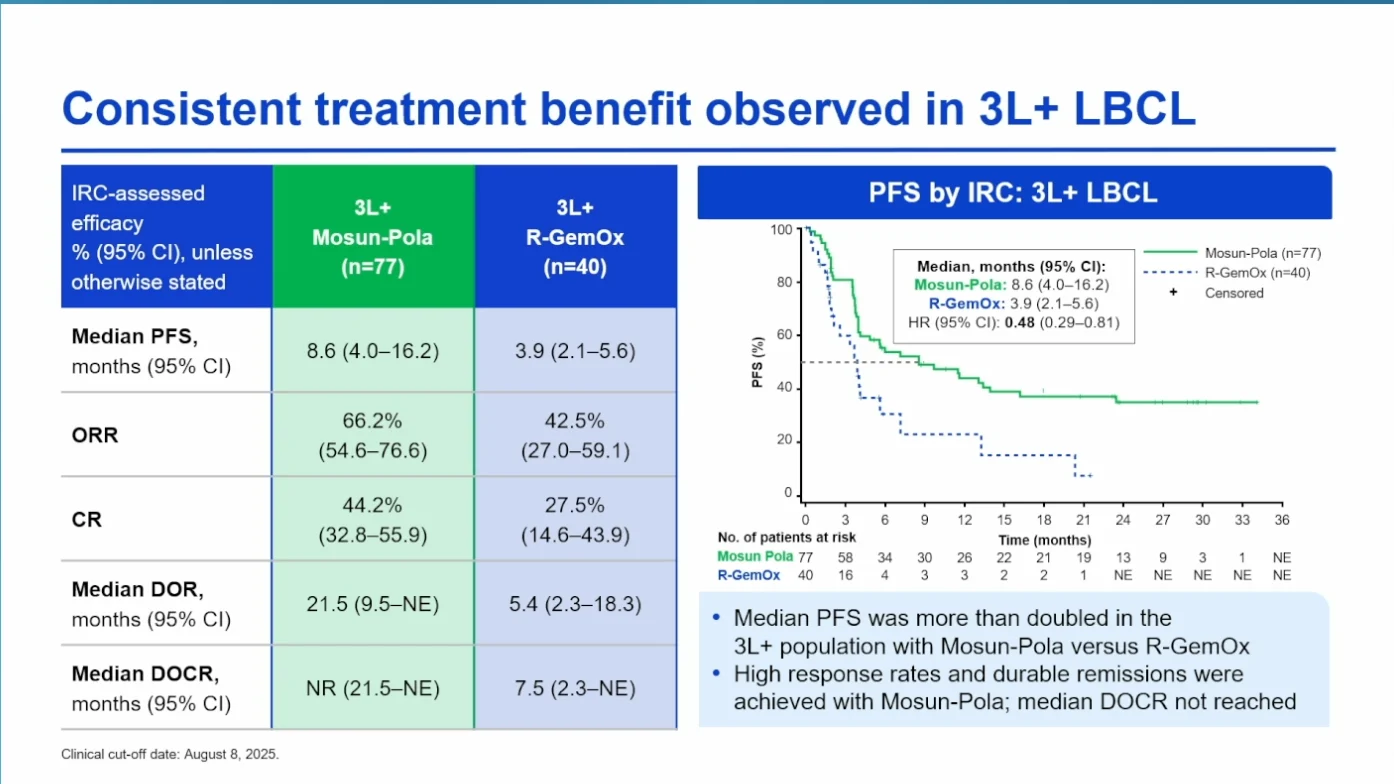
In the 2L subgroup, median PFS improved from 3.6 to 17.6 months, while CR rates increased from 20.0% to 60.7% with Mosun-Pola vs R-GemOx. Benefit was also maintained in the 3L+ setting, where median DOR reached 21.5 months and CR rates were 44.2% vs 27.5%, respectively.
Response durability favored Mosun-Pola, with median DOR improving from 6.0 to 18.8 months, while median DOCR was not reached with Mosun-Pola. PFS benefit was consistent across treatment lines, with similar HRs in both 2L and 3L+ subgroups. OS data remain immature at the current data cutoff.
Safety Analysis
Safety remained consistent with prior analyses, with no new safety signals.Grade ≥2 CRS was reported in 4% of patients treated with Mosun-Pola, and no ICANS events. In the 2L subgroup, grade 2 CRS occurred in 3% of patients, with no grade ≥3 CRS events reported.

Outcomes by Age Group
PFS benefit was maintained in both patients aged <65 and ≥65 years, with similar HRs observed between subgroups. The safety profile also remained comparable, with manageable CRS, infection and peripheral neuropathy rates, without a major increase in severe toxicities among older patients.
Bottom Line
With extended follow-up from the phase 3 SUNMO trial, fixed-duration Mosun-Pola continued to demonstrate high efficacy in ASCT-ineligible R/R LBCL, with durable responses observed across treatment-line and age subgroups. Activity remained strong in the 2L setting, including among patients with primary refractory or early relapsed disease. TEAEs remained consistent and manageable, also supporting the feasibility of outpatient administration, including in older and frail patients.
Discussion Point
The updated findings arrive at a time when treatment sequencing in R/R LBCL is receiving increasing attention, bringing focus to subsequent CAR-T eligibility in selected patients and integration into evolving clinical pathways.
{kind=link}
{kind=link}
{kind=link}