


At the 2026 ASCO Annual Meeting, Neeraj Agarwal presented results from TALAPRO-3, a Phase 3 trial evaluating talazoparib plus enzalutamide in patients with metastatic castration-sensitive prostate cancer harboring homologous recombination repair gene alterations. The results were also published on May 30, 2026, in The New England Journal of Medicine.
Study Design
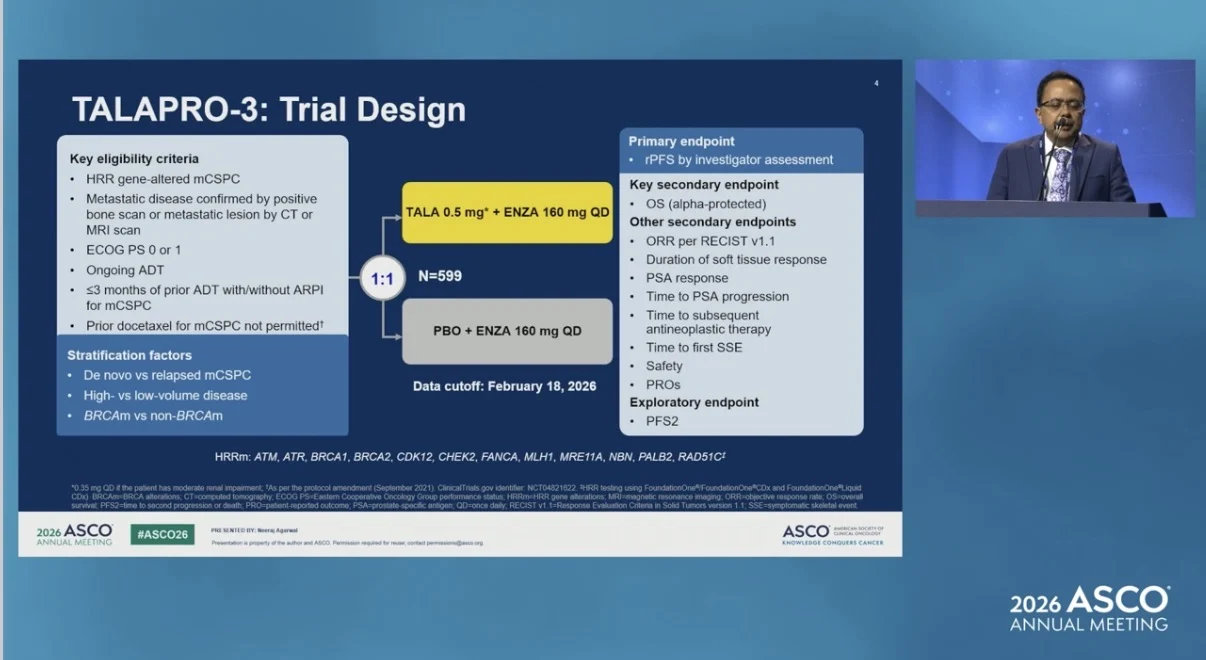
TALAPRO-3 is an ongoing, international, Phase 3, double-blind, randomized, placebo-controlled trial. Patients were randomized 1:1 to receive talazoparib 0.5 mg once daily plus enzalutamide 160 mg once daily, or placebo plus enzalutamide 160 mg once daily. Patients with moderate renal impairment received talazoparib 0.35 mg once daily. All patients received ongoing androgen-deprivation therapy.
Eligible patients had HRR gene-altered metastatic castration-sensitive prostate cancer, ECOG performance status 0 or 1, and metastatic disease confirmed by bone scan or CT/MRI. Patients could have received up to 3 months of prior ADT with or without an androgen receptor pathway inhibitor for metastatic castration-sensitive prostate cancer. Prior docetaxel for metastatic castration-sensitive prostate cancer was not permitted. Randomization was stratified by de novo versus relapsed disease, high- versus low-volume disease, and BRCA-mutated versus non-BRCA-mutated status.
The primary endpoint was investigator-assessed radiographic progression-free survival. Overall survival was the key secondary endpoint.

Study Population
A total of 599 patients were randomized. Among them, 300 were assigned to the talazoparib group and 299 to the control group. Patients had metastatic disease and alterations in at least one homologous recombination repair gene. Eligible genes included ATM, ATR, BRCA1, BRCA2, CDK12, CHEK2, FANCA, MLH1, MRE11A, NBN, PALB2, and RAD51C. Overall, 35% of patients had BRCA1 or BRCA2 alterations, 71% had high-volume disease, and 84% had newly diagnosed metastatic disease. The most commonly altered genes were BRCA2, ATM, CDK12, and CHEK2.
Key Efficacy Results
At the February 18, 2026 data cutoff, median follow-up for rPFS was 37.6 months in the talazoparib plus enzalutamide group and 37.7 months in the placebo plus enzalutamide group. Talazoparib plus enzalutamide significantly improved investigator-assessed rPFS compared with placebo plus enzalutamide.
At 3 years, rPFS was 76.6% with talazoparib plus enzalutamide and 56.2% with placebo plus enzalutamide. Median rPFS was not reached in the talazoparib plus enzalutamide group and was 45.8 months in the placebo plus enzalutamide group. The hazard ratio for progression or death was 0.481, with a 95% confidence interval of 0.357–0.647 and P<0.0001.
BRCA and Non-BRCA Subgroups
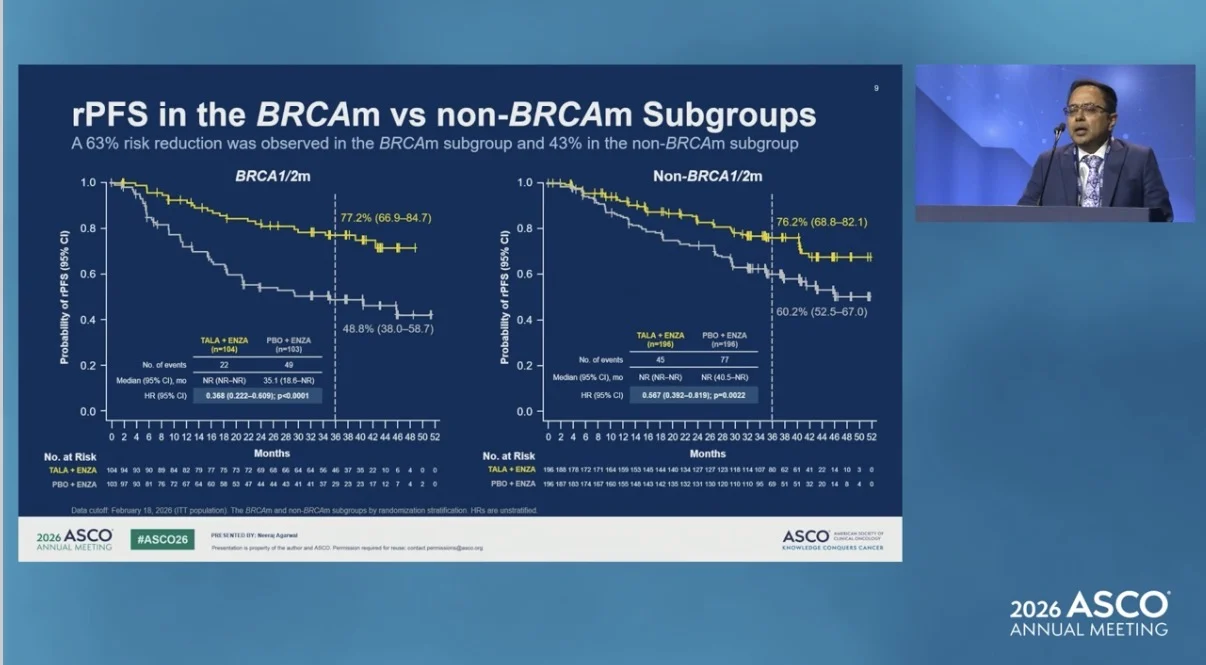
The rPFS benefit was observed in both BRCA-mutated and non-BRCA-mutated subgroups. Among patients with BRCA1/2 alterations, 3-year rPFS was 77.2% with talazoparib plus enzalutamide and 48.8% with placebo plus enzalutamide. The hazard ratio was 0.368, with a 95% confidence interval of 0.222–0.609.
Among patients without BRCA1/2 alterations, 3-year rPFS was 76.2% with talazoparib plus enzalutamide and 60.2% with placebo plus enzalutamide. The hazard ratio was 0.567, with a 95% confidence interval of 0.392–0.819. A consistent treatment effect for rPFS was observed across prespecified subgroups.

Overall Survival and Other Outcomes
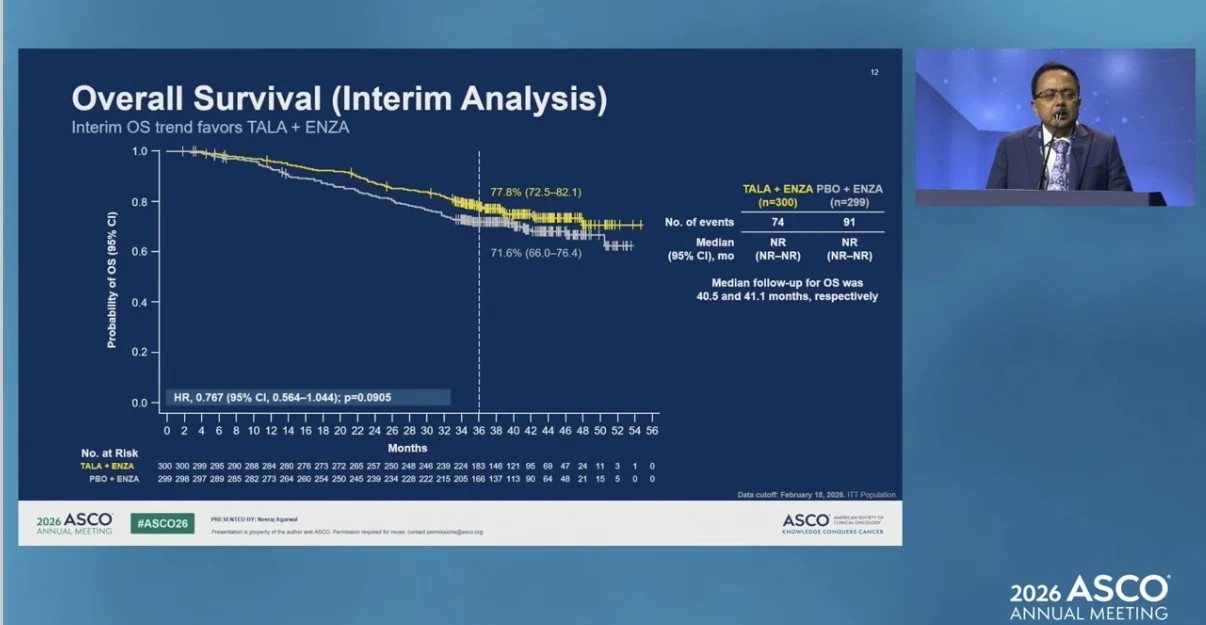
At the interim overall survival analysis, overall survival favored talazoparib plus enzalutamide, but statistical significance had not been reached. There were 74 deaths in the talazoparib plus enzalutamide group and 91 deaths in the placebo plus enzalutamide group.
At 3 years, overall survival was 77.8% with talazoparib plus enzalutamide and 71.6% with placebo plus enzalutamide. The hazard ratio was 0.767, with a 95% confidence interval of 0.564–1.044 and P=0.0905. Talazoparib plus enzalutamide also improved time to PSA progression. At 3 years, 78.3% of patients in the talazoparib plus enzalutamide group and 62.7% in the placebo plus enzalutamide group were free from PSA progression. The hazard ratio was 0.513, with a 95% confidence interval of 0.370–0.712 and P<0.0001.
Time to initiation of subsequent systemic antineoplastic therapy was also improved. At 3 years, 78.6% of patients in the talazoparib plus enzalutamide group and 62.0% in the placebo plus enzalutamide group had not started subsequent antineoplastic therapy. The hazard ratio was 0.514, with a 95% confidence interval of 0.378–0.698 and P<0.0001.
Among patients with measurable disease, objective response was reported in 74.7% of patients in the talazoparib plus enzalutamide group and 67.0% in the placebo plus enzalutamide group.

Safety
The most common treatment-emergent adverse events with talazoparib plus enzalutamide were hematologic events, including anemia and decreased neutrophil count, and fatigue.
Grade 3–4 treatment-emergent adverse events occurred in 79% of patients in the talazoparib plus enzalutamide group and 41% in the placebo plus enzalutamide group. Serious adverse events occurred in 42% and 32% of patients, respectively.
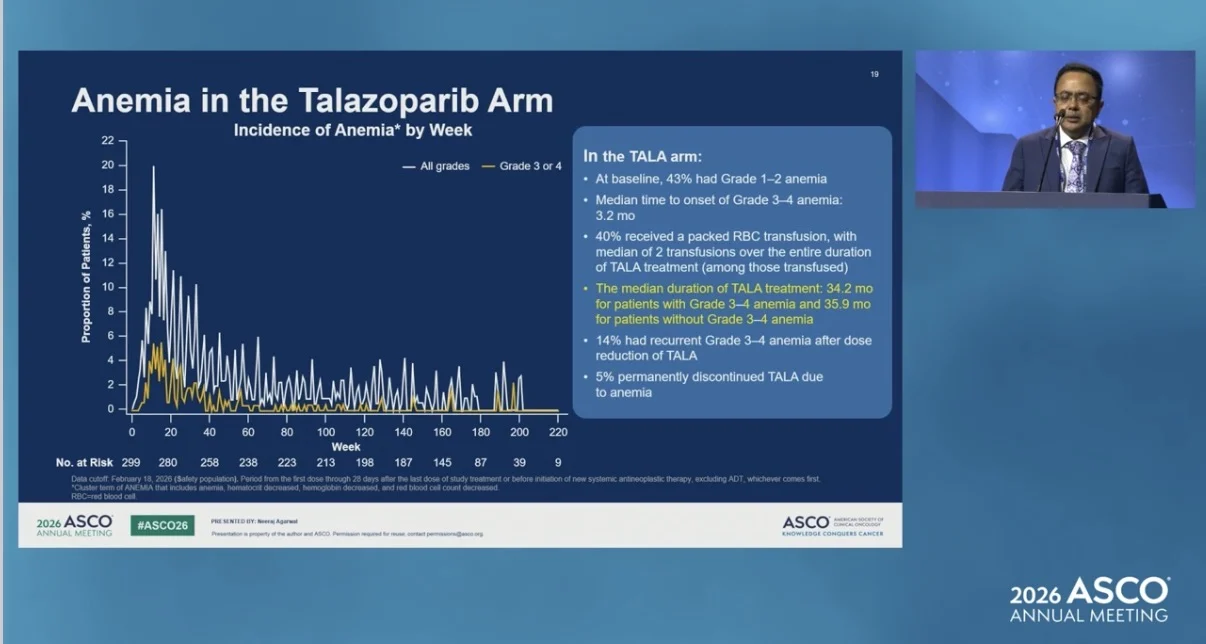
The most common all-cause treatment-emergent adverse events in the talazoparib plus enzalutamide group were anemia, fatigue, decreased neutrophil count, neutropenia, asthenia, and decreased white blood cell count. Anemia occurred in 71% of patients in the talazoparib plus enzalutamide group, including grade 3–4 anemia in 51%.

Adverse events led to permanent discontinuation of talazoparib in 19% of patients. Five percent of patients discontinued talazoparib due to anemia. Two treatment-related deaths occurred in the talazoparib plus enzalutamide group and none in the placebo plus enzalutamide group. Patient-reported outcomes generally did not show clinically meaningful differences between the two arms, except for appetite loss on the EORTC QLQ-C30.
Takeaway
TALAPRO-3 met its primary endpoint. Talazoparib plus enzalutamide significantly prolonged radiographic progression-free survival compared with placebo plus enzalutamide in patients with HRR gene-altered metastatic castration-sensitive prostate cancer.

The rPFS benefit was observed in both BRCA-mutated and non-BRCA-mutated subgroups. Interim overall survival trended in favor of talazoparib plus enzalutamide, but statistical significance had not been reached. The most common adverse events were hematologic events and fatigue. These results support talazoparib plus enzalutamide as a potential treatment option for patients with HRR gene-altered metastatic castration-sensitive prostate cancer.
The full abstract is available on the official ASCO website.

Read about A-DREAM/Alliance A032101 at ASCO 2026 on OncoDaily.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}