


At the 2026 ASCO Annual Meeting, Shilpa Gupta, MD, from Cleveland Clinic – Taussig Cancer Institute, presented results from MAIN-CAV, a phase 3 randomized trial evaluating maintenance cabozantinib plus avelumab compared with avelumab alone after first-line platinum-based chemotherapy in patients with locally advanced or metastatic urothelial cancer.
Maintenance avelumab is an established standard of care for patients with locally advanced or metastatic urothelial carcinoma who do not progress after first-line platinum-based chemotherapy. Cabozantinib targets VEGFR, MET, and TAM kinases, providing a rationale for combining VEGF inhibition with immune checkpoint blockade.
MAIN-CAV tested whether adding cabozantinib to maintenance avelumab could improve outcomes with an acceptable safety profile compared with avelumab maintenance alone.

Read more about Cabozantinib on OncoDaily.
Study Design
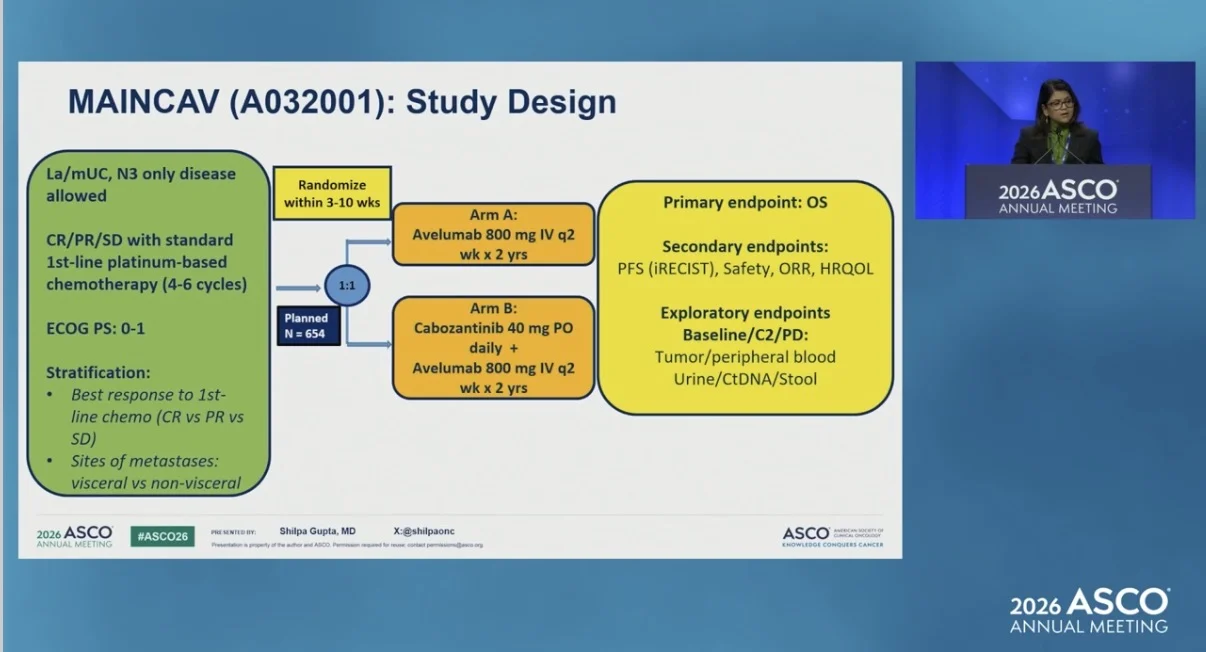
MAIN-CAV was a randomized phase 3 Alliance trial.
Eligible patients had locally advanced or metastatic urothelial carcinoma, including N3-only disease, and had complete response, partial response, or stable disease after 4 to 6 cycles of standard first-line platinum-based chemotherapy. Eligible patients had ECOG performance status 0 or 1.
Patients were randomized 1:1 within 3 to 10 weeks to receive avelumab 800 mg intravenously every 2 weeks for up to 2 years, either alone or with cabozantinib 40 mg orally daily.
Stratification factors included best response to first-line chemotherapy, defined as complete response versus partial response versus stable disease, and sites of metastases, defined as visceral versus non-visceral. The primary endpoint was overall survival. Secondary endpoints included progression-free survival, safety, objective response rate, and health-related quality of life.
The planned accrual was 654 patients. However, the trial closed early because of poor accrual in an evolving treatment landscape. Between March 2022 and March 2024, 68 patients were enrolled. At the data cutoff of January 13, 2026, median follow-up was 21.5 months.

Results
A total of 68 patients were randomized: 33 to avelumab alone and 35 to cabozantinib plus avelumab. In the combination arm, 33 patients received treatment.
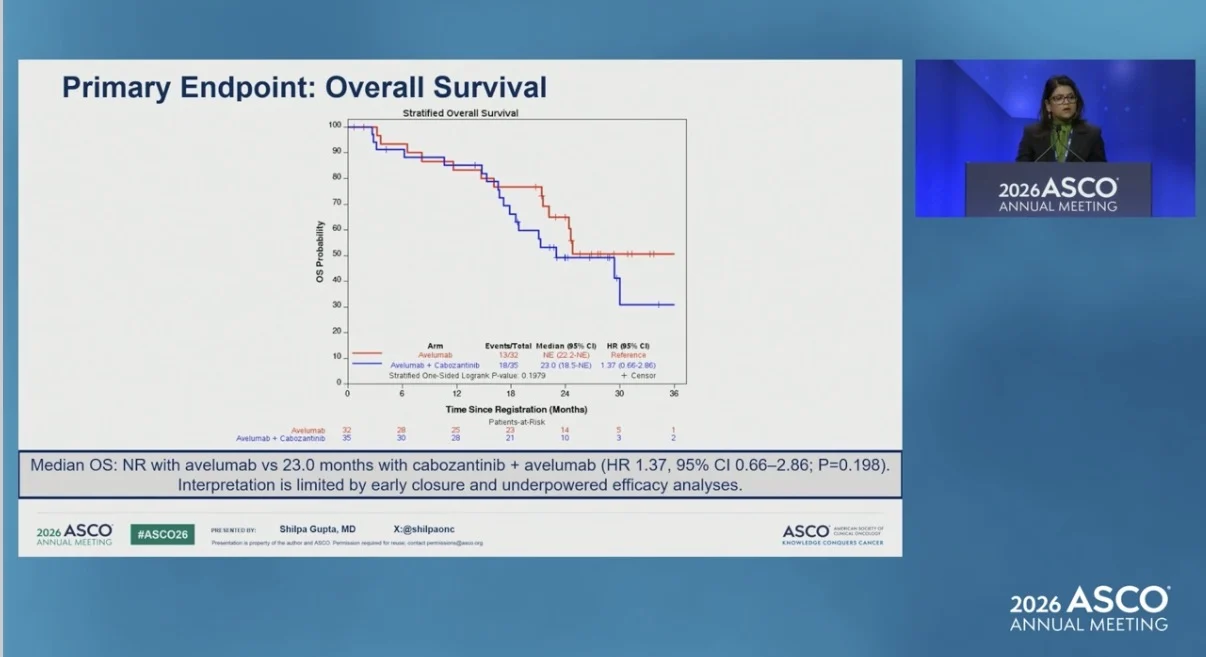
Median overall survival was not reached with avelumab alone and was 23.0 months with cabozantinib plus avelumab. The hazard ratio was 1.37, with a 95% confidence interval of 0.66 to 2.86, and the difference was not statistically significant.
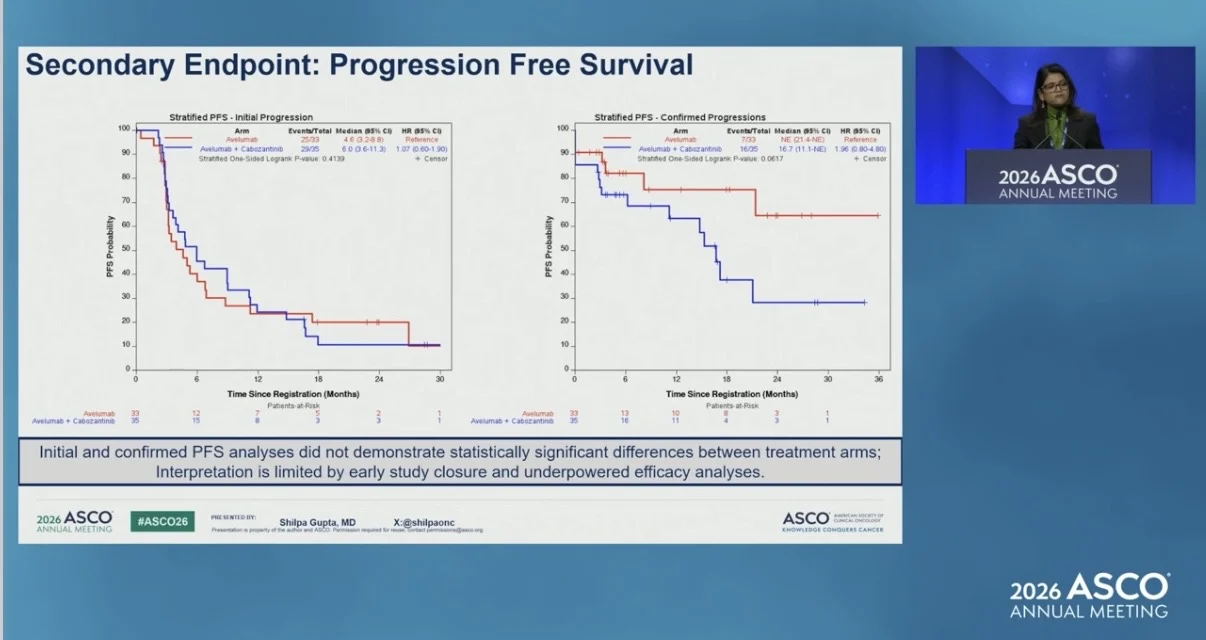
Initial-progression progression-free survival was also not significantly different between arms. Median PFS was 4.6 months with avelumab alone and 6.0 months with cabozantinib plus avelumab.

For confirmed progression, median PFS was not reached with avelumab alone and was 16.7 months with cabozantinib plus avelumab. This analysis also did not demonstrate a statistically significant difference between treatment arms, and interpretation was limited by early study closure and underpowered efficacy analyses.
Among RECIST-evaluable patients, confirmed objective responses occurred in 5 of 24 patients treated with avelumab alone and 3 of 26 patients treated with cabozantinib plus avelumab. The objective response rate was 20.8% with avelumab and 11.5% with cabozantinib plus avelumab.
Safety
Grade 3 treatment-related adverse events occurred in 24.2% of patients treated with avelumab alone and 39.4% of patients treated with cabozantinib plus avelumab.
Grade 3 hypertension occurred in 3.0% of patients in the avelumab arm and 18.2% of patients in the combination arm. Grade 3 or higher hematologic treatment-related adverse events occurred in 0% and 9.1% of patients, respectively.
Cabozantinib dose reductions occurred in 22 of 33 patients, or 66.7%. Drug discontinuations were reported in 6 of 66 patients receiving avelumab and 7 of 33 patients receiving cabozantinib. No new safety signals were identified beyond the known safety profiles of avelumab and cabozantinib.
Conclusion
In this prematurely closed, underpowered randomized phase 3 trial, adding cabozantinib to maintenance avelumab did not improve overall survival compared with avelumab alone in patients with locally advanced or metastatic urothelial carcinoma who had not progressed after first-line platinum-based chemotherapy.

The combination did not show a clear efficacy benefit, while safety was consistent with the known profiles of avelumab and cabozantinib. Ongoing correlative analyses may provide further insight into mechanisms of response and resistance.
The full abstract is available on the official ASCO website.

You can also read about PROTRACT Updates at ASCO 2026 on OncoDaily.
{kind=link}
{kind=link}
{kind=link}
{kind=link}