


In a series of detailed updates shared on his X page, Dr. Talha Badar, Hematology/Oncology Specialist at Mayo Clinic, broke down the most impactful myeloid and lymphoid malignancy presentations from EHA2026.
From targeted AML treatment strategies to novel molecular pathways in MPNs, MDS, and ALL, here are the key practice-informing highlights reshaping hematologic oncology.
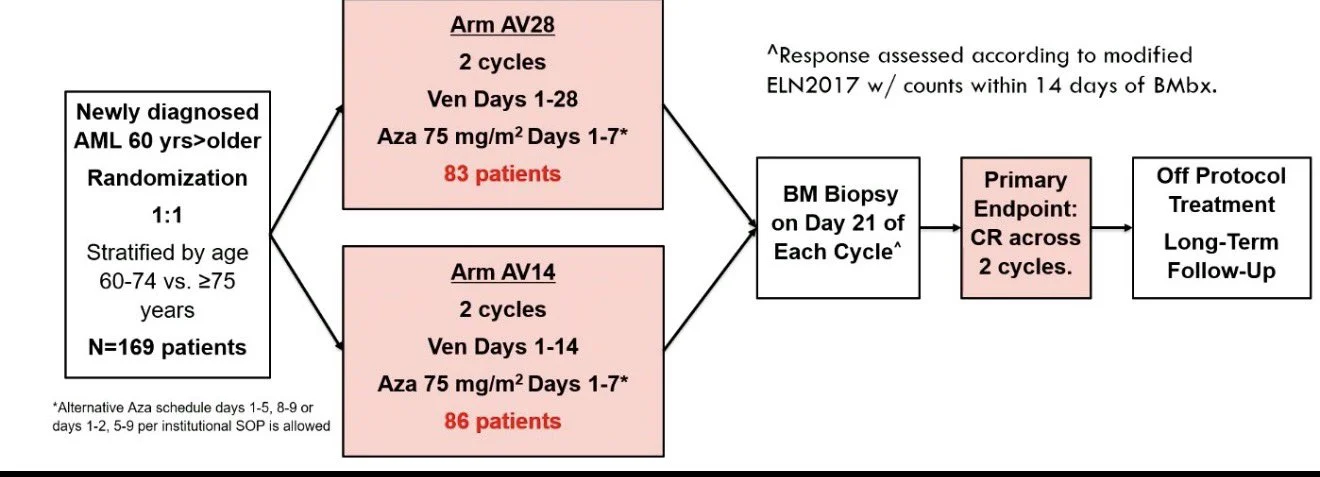
“Dr. Barote: OPTI-AML: the first prospective RCT of Ven 14d vs 28d + Aza ×2 cycles in older AML – and it reframes the whole ‘shorter is fine’ debate.
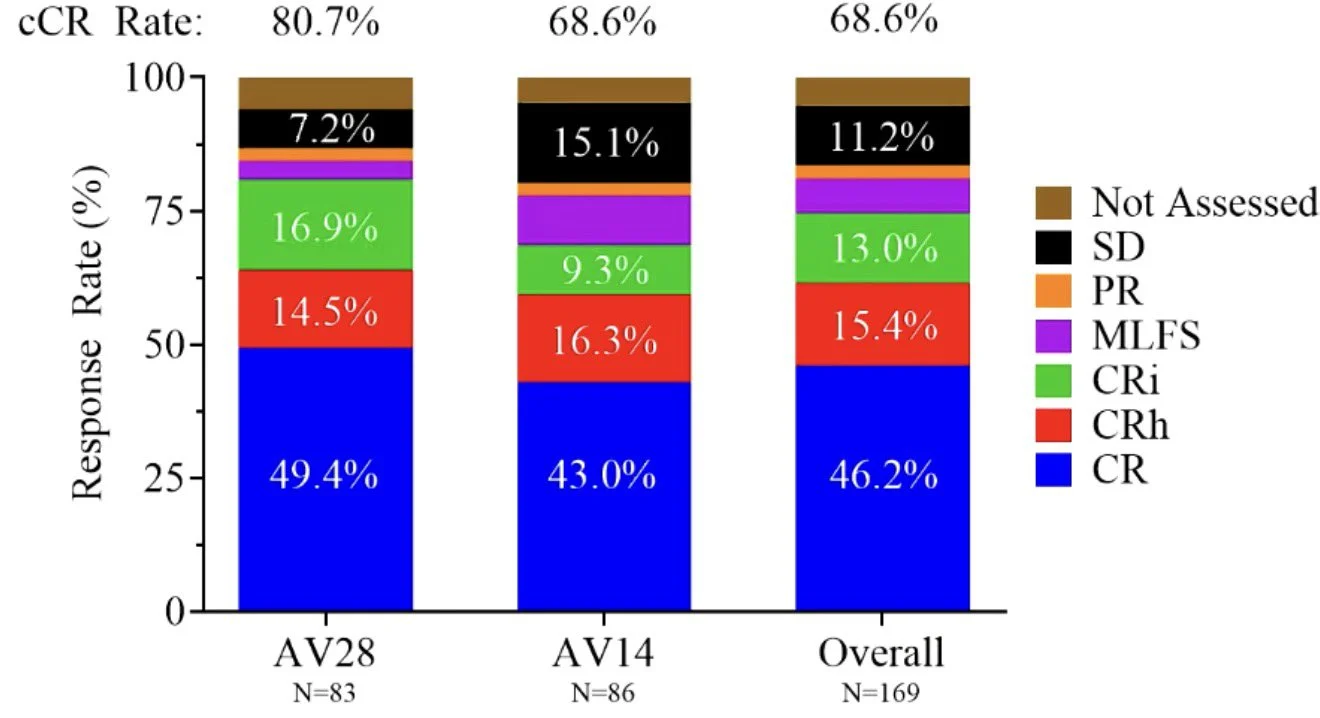
AV14 did NOT meet non-inferiority for CR (43% vs 49% AV28; ΔCI –8% to +21%, upper bound >10%).
Key takeaways
But the real story is molecular, not calendar:
- NPM1 and IDH1/2 – favored 28d (61% vs 42%)
- Every other subset – 44% vs 44%, identical
And cumulative delivery, not the planned schedule, tracked with response: pts who couldn’t complete Ven had lower CR in BOTH arms (AV28 39% vs 56%; AV14 36% vs 49%). Only 68% of AV28 finished C1 Ven (vs 89%) – mostly infections. MRD negativity (78% vs 77%) and toxicity were superimposable. OS numerically favored AV28 but on MVA was driven by TP53/KRAS + counts, not arm.
Bottom line: Ven duration should be titrated to molecular subtype + triplet partner – what matters is cumulative exposure delivered, and for NPM1/IDH that exposure still earns its keep.

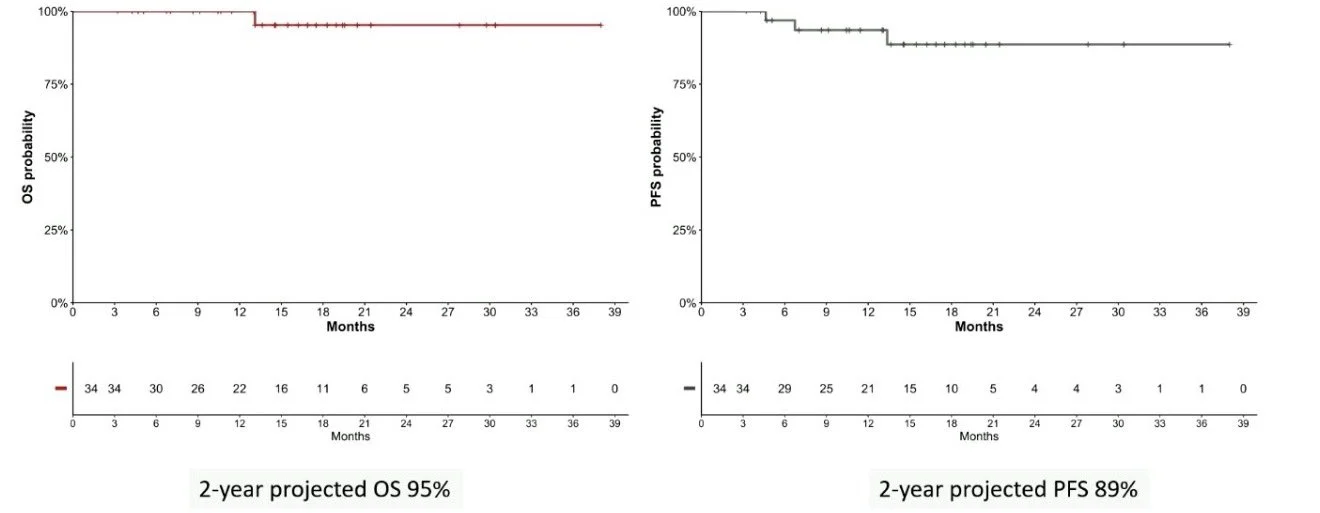
GIMEMA AML2521 (Ph2): VEN-AZA for molecular failure in NPM1-mut AML as a bridge-to-transplant.
Results are striking:
- MRDneg 79% (median 2 cycles)
- 85% bridged to HSCT, 70% MRDneg pre-SCT
- 2-yr OS 95% / PFS 89%
Key Takeaways
Why VEN-AZA over the alternatives?
- vs direct transplant: pre-HSCT MRD+ predicts relapse, so deepening first is rational – but a single-arm n=34 can’t separate true benefit from selection of favorable biology.
- vs menin inhibitor: revumenib/zifto are now approved, but only for overt R/R disease (~21% CR/CRh); zero prospective data in the molecular-failure/bridge setting.
Promising, practice-informing, hypothesis-generating; practice-changing? The MRD-directed menin ± VEN-AZA trial is the obvious next step.

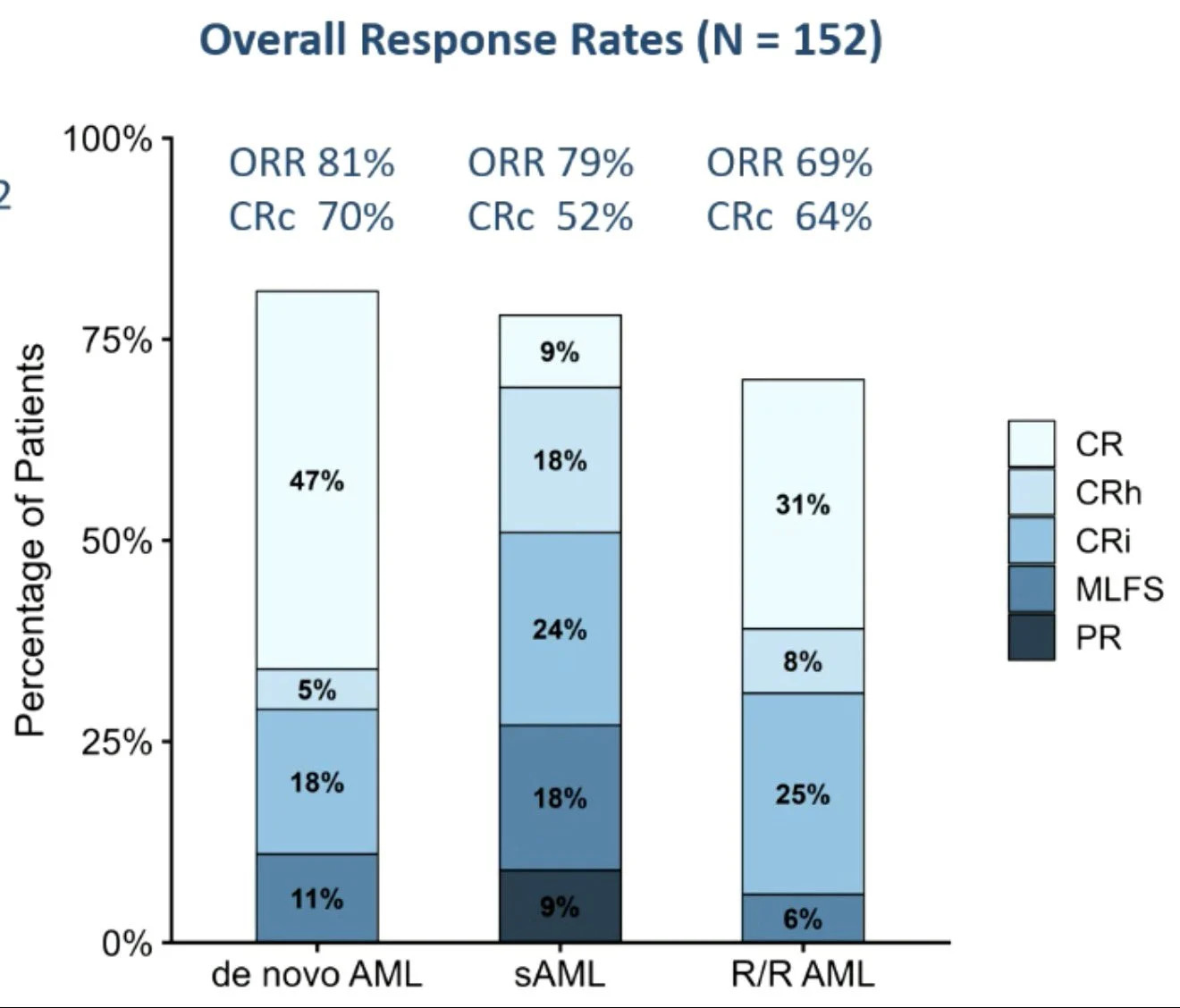
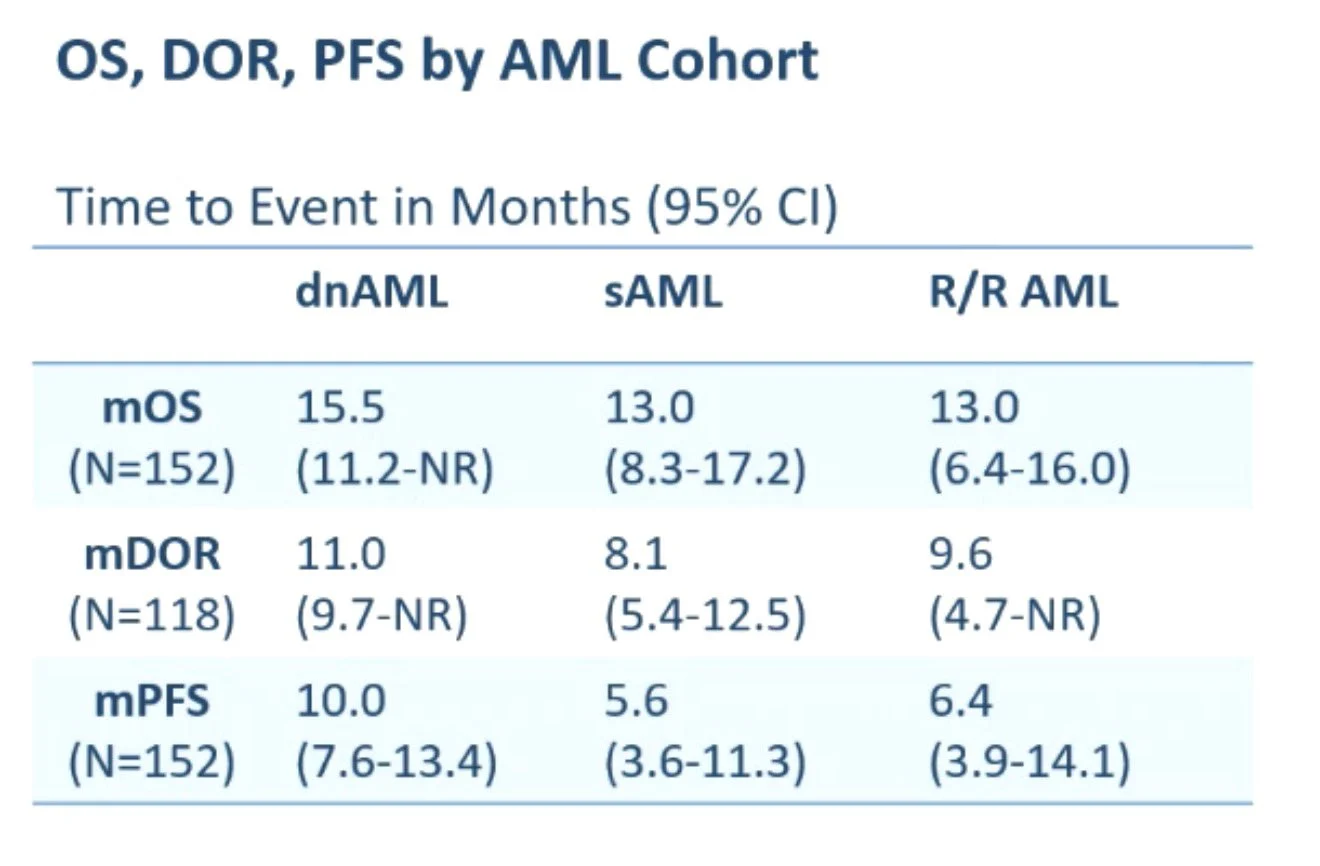
Nordic LD-VenEx (Ph2): reduced-duration VEN (D1-14 – D1-7 after blast clearance) + AZA across AML.
- CRc 70% / 52% / 64% (de novo / sAML/ R/R)
- mOS 15.5 / 13.0 / 13.0 mo
- G≥3 thrombocytopenia 21% vs 45% (VIALE-A)
- Outpatient incl. C1, lower cost
Key takeaways
Once blasts clear, 7 days of VEN may be enough. LD-VenEx supports reduced-duration VEN/AZA as efficacious, safer and cheaper across dn/s/R/R AML. Less VEN, same efficacy.

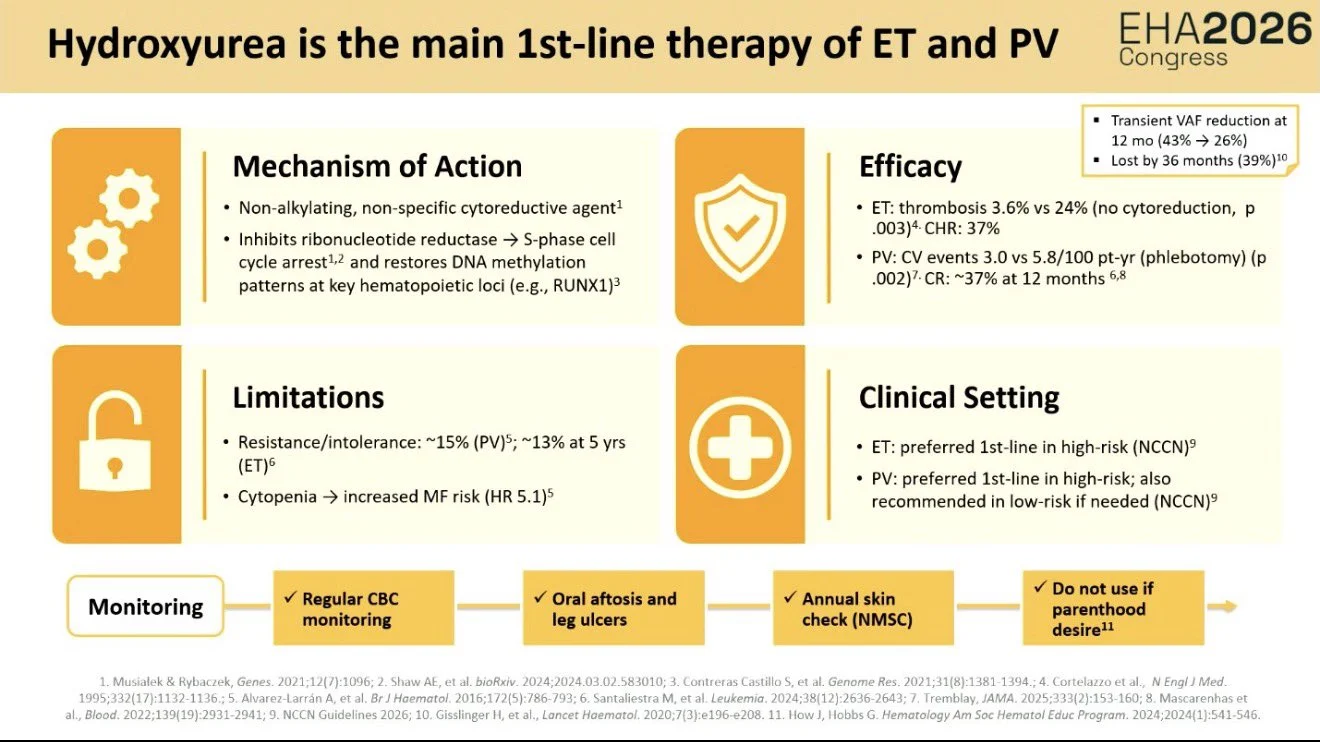
Excellent talk by Dr. Francesca Palandri on ET/PV at EHA2026
Key takeaways:
Hydroxyurea remains the main 1L cytoreductive therapy, but care is increasingly individualized.
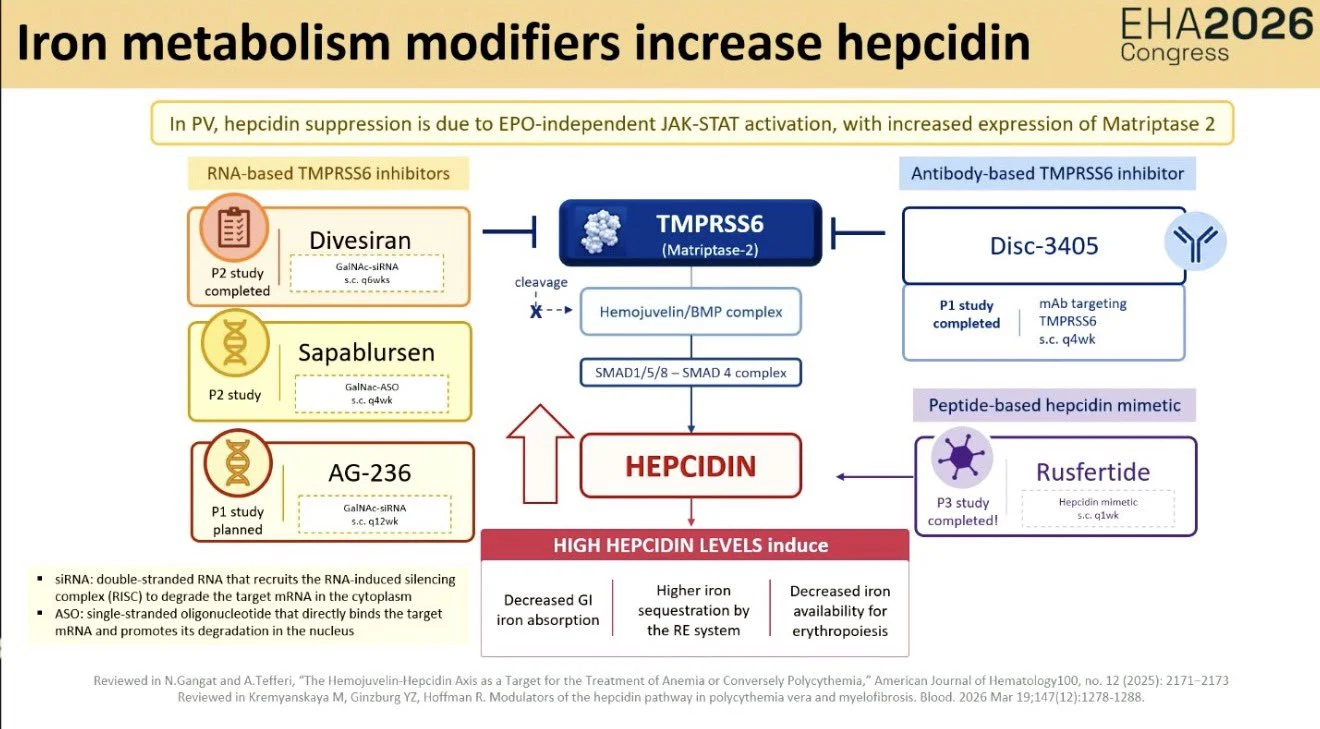
Emerging directions:
- Hepcidin modulation in PV, rusfertide and TMPRSS6 inhibitors
- CALR-targeted therapy, mAb and bispecific T-cell engagers
- Multidisciplinary care, including CV risk, fertility, dermatology, thrombosis, QoL
bvThe future of MPN care is moving beyond count control toward disease biology, iron regulation, immune targeting, and patient-centered care.

Interesting translational data from the EPO-PRETAR trial presented at EHA2026 exploring predictors of ESA response in lower-risk MDS.
Early ESA response in LR-MDS appears linked to adaptive immune activation, especially CD4/CD8 T-cell and IFN-γ signatures. Late/non-responders show more inflammatory and innate immune signaling, including IL-6/IL-10 pathways.
SF3B1-mutated disease may enrich for an immune profile associated with ESA sensitivity.

TP53-Mutated MDS: The CCR5 Axis as a Driver of T-Cell Exhaustion
TP53-mutated MDS exhibits a distinct exhausted T-cell phenotype with increased immune checkpoint expression.
- Single-cell analyses identified activation of the CCR5 signaling axis as a key driver of T-cell dysfunction and immune escape.

Decitabine Primes CD38-Directed Immunotherapy in T-ALL
- Decitabine upregulates CD38 expression on T-ALL cells, enhancing susceptibility to daratumumab-mediated ADCP.
- In preclinical models, decitabine followed by daratumumab improved leukemia control and prolonged survival compared with either agent alone.
- These findings support epigenetic priming as a strategy to enhance CD38-targeted immunotherapy in mature T-ALL and warrant clinical investigation.

Poster Presentation: Predicting CNS Dissemination in B-ALL
Transcriptomic signatures involving chemokine trafficking, adhesion/ECM remodeling, and pro-survival signaling pathways may underlie CNS dissemination in B-ALL.

Poster Presentation: High-Risk Genetics in ALL: Outcomes Improving, But Not Equally Across Subtypes
- In 615 children and young adults with high-risk genetic ALL, overall survival improved substantially across successive UKALL trials (47% – 84%), with relapse rates falling from 65% to 27%.
- The greatest gains were seen in KMT2A-rearranged and iAMP21 ALL, whereas outcomes for low hypodiploid, near-haploid, and BCR::ABL1 ALL showed less improvement in the pre-TKI era.
- Risk factors differed by genetic subtype: CNS involvement and immunophenotype predicted relapse in KMT2A-r ALL, while relapse was more frequent in B-cell than T-cell ABL-class ALL, underscoring the need for genotype-specific risk stratification.”


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}