


Samer Al Hadidi, Associate Professor at UT Southwestern Medical Center, shared a post on X:
“CAR-PRISM: Cilta cel in smoldering myeloma
n=20 patients
1ry endpoint: dose limiting toxicities+ treatment emergent adverse events (I.e: safety)
With important observations.
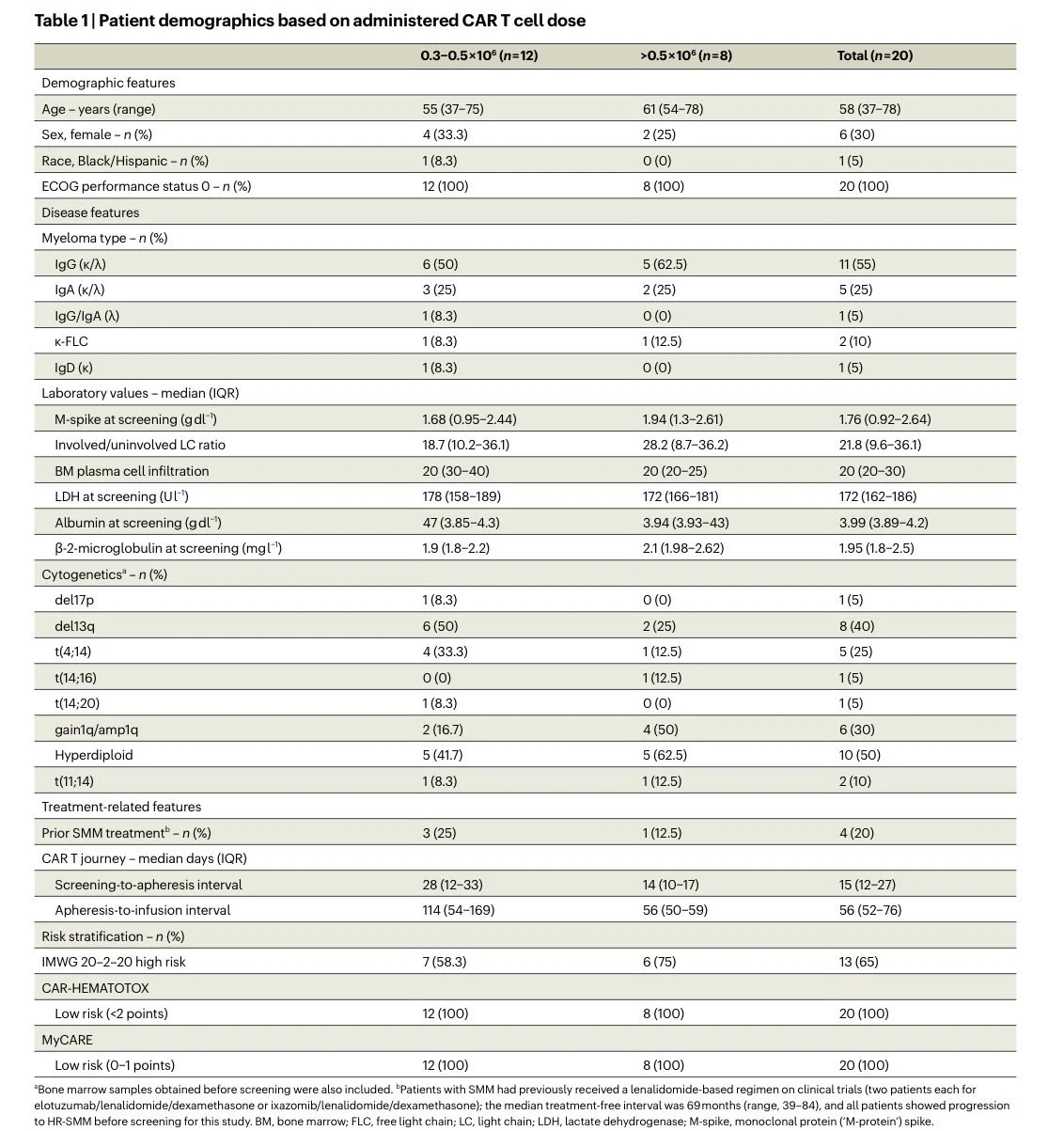
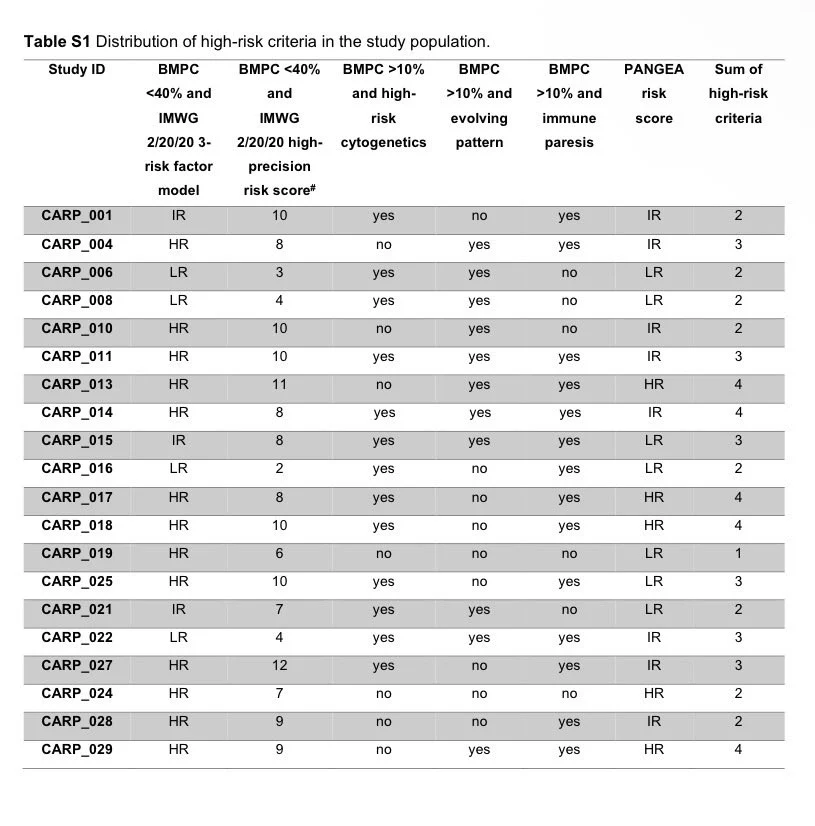
1. Did the trial actually enrolled only high risk smoldering myeloma?
- 35% didn’t meet IMWG 20-2-20 criteria for high risk
- median time between initial diagnosis enrollment was 16.1 months (IQR 8.4-36.2 months)
- 20% (n=4) had prior ttt for SMM with median ttt free interval of ~6 yrs)
- >=40% PC in marrow excluded
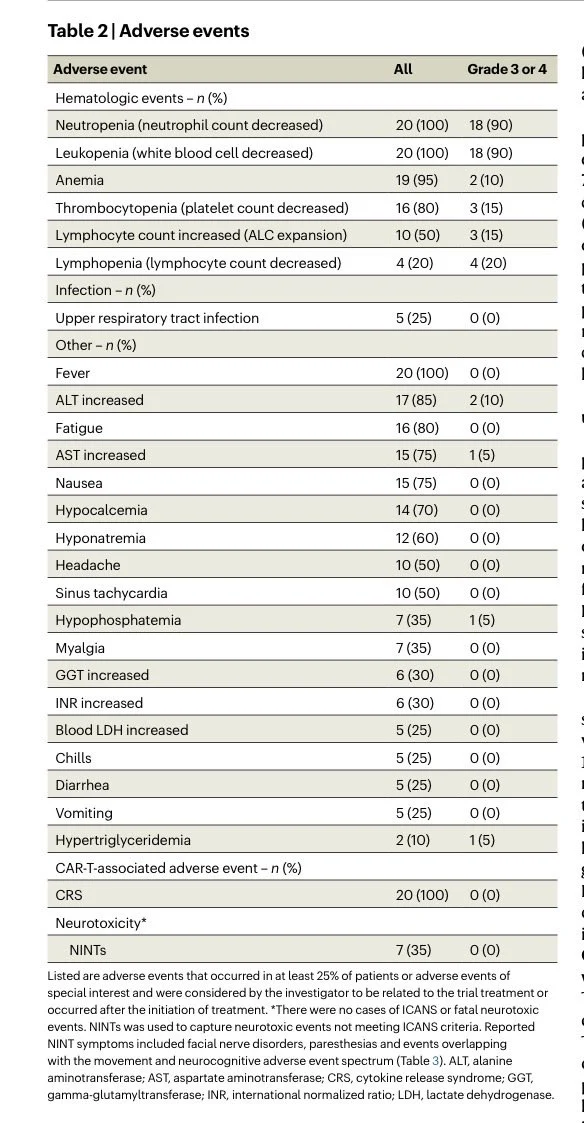
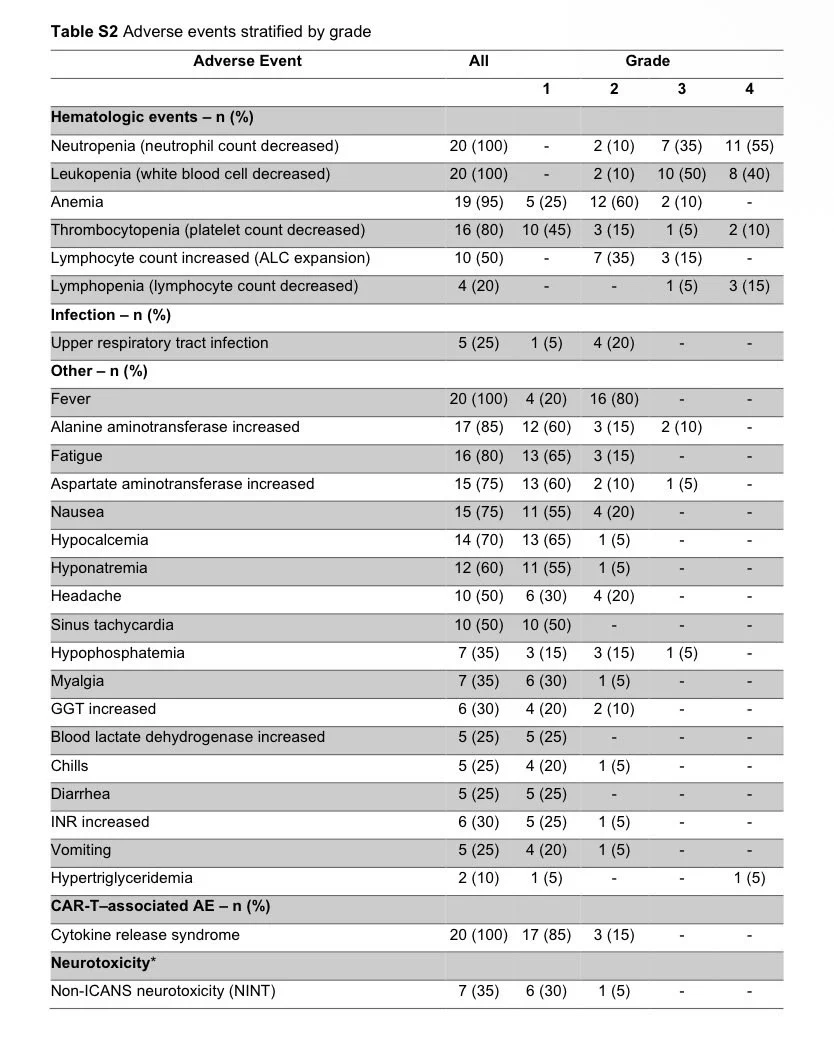
2. How safe was the use of Cilta cel in relatively low volume disease and no bridging therapy?
- CRS: 100% (G2: 15%)
- Neutropenia: 100% (G3: 35%, G4: 55%)
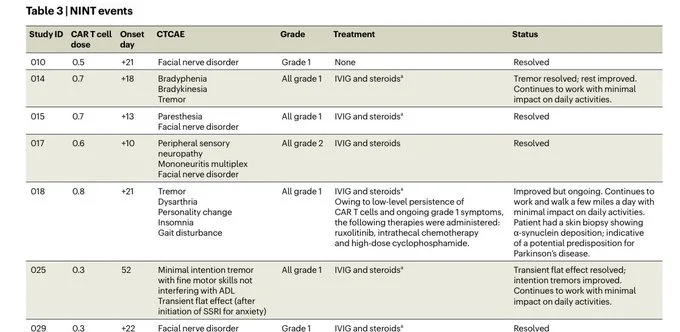
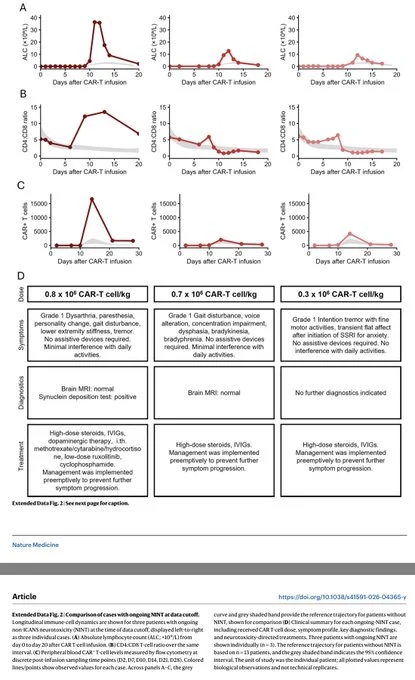
- Non ICANS neurotoxicity: 35% (15% of pts with persistent toxicity)
- Cranial nerve palsy: 20%, including bilateral facial nerve palsy
- Transaminitis: 85% (G3/4: 10%)
3. Any changes that occurred based on the toxicity signal?
The trial was mid-course amended:
- dose reduced to 0.3×10⁶
- ALC-triggered dexamethasone added
- enrollment spaced to 30-day intervals
- FDA safety pause
Summary of Non ICANS neurotoxicity below.
4. Was dose deriving the non ICANS neurotoxicity?
Not likely, but the worst reported case was with the dose 0.8, quite worrisome adverse events.
One patient received intrathecal chemotherapy + cyclophosphamide + ruxolitinib
5. What did the patients get as part of the treatment?
- Chemotherapy, lymphodepleting: 100%
- Prophylactic IVIG: 100%
- Therapeutic IVIG: ~40% (on top of prophylaxis, IVIG used for NINT management and 2 cases of immune thrombocytopenia. High-dose regimens (1g/kg × 1-2 doses) used in some)
- Tocilizumab: 85%
- Dexamethasone: 65%
For asymptomatic persons, depending on the math you use, a lot of time commitments, hospitalisation, caregiver support, time of work, etc.
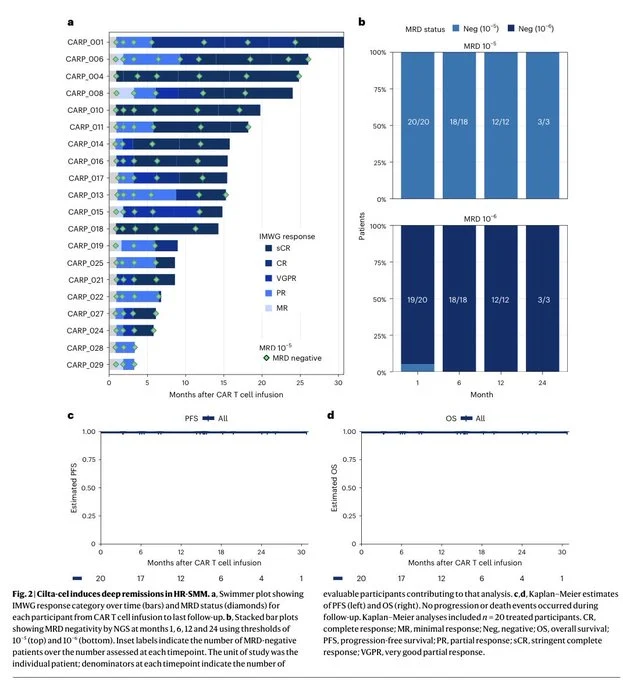
6. What is the efficacy?
This is a secondary goal (the most important Q in this study was safety):
- median follow up: 15 months
- MRD negativity 10-6 by 2 months: 100%
Deep responses , short follow up to assess durability.
Bottom line:
For asymptomatic condition with a risk to progress to a condition that has excellent treatment options and outcomes (and despite the deep responses) those toxicities reported are really concerning
End.
Raj Chakraborty, Hematologist, Oncologist, Clinical Researcher at Herbert Irving Comprehensive Cancer Center, and Assistant Professor at Columbia University Irving Medical Center, shared the post, adding:
“Excellent summary of CAR-PRISM by Samer Al Hadidi:
‘For an asymptomatic condition with a risk to progress to a condition that has excellent treatment options and outcomes (and despite the deep responses) those toxicities reported are really concerning!’
Title: Ciltacabtagene autoleucel in high-risk smoldering multiple myeloma: the CAR-PRISM phase 2 trial

Other articles featuring Samer Al Hadidi and Raj Chakraborty on OncoDaily.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}