


Tyler Seiber, Assistant Professor in the Division of Radiation Oncology and a member of the RMAS Center for Precision Radiation Medicine (CPRM), shared a post by Tony Felefly, Radiation Oncologist, on X, adding:
”RAMPP trial: Some signals for benefit of radical prostatectomy for oligometastatic Prostate Cancer Underpowered for OS. More grade 3+ toxicity compared to RT Radiation Oncology.”
Quoting Tony Felefly‘s post:
”The RAMPP trial has landed.
Congratulations to the authors for this great work!! It compared best systemic therapy + RP (with extended LND) to BST alone for patients with de-novo synchronous oligometastatic PCa, defined as =< 5 bone mets. BST consisted of lifelong ADT. It closed early due to STAMPEDE results. Cancer-Specific mortality was the primary enpoint. Clinical progression and OS were secondary endpoints. An X-torial.
Nearly 1/3 were PET-staged, 92% had 1-3 bone mets. ~1/3 had cN1 disease. ARPI was used in 6% in BST arm, 0% in BST+RP. Chemo was in 5% (BST+RP) and 11% (BST). So technically, the trial evaluates the addition of RP to ADT alone in patients with moslty 1-3 bone mets.
Of note, the population studied in RAMPP has a lower disease burden than STAMPEDE and PEACE-1, that included patients with low-burden as per CHAARTED definition, that was NOT necessarily oligometastatic. The benefit of local therapy is expected to decrease with increasing metastatic burden.
Title: Association of Bone Metastatic Burden With Survival Benefit From Prostate Radiotherapy in Patients With Newly Diagnosed Metastatic Prostate Cancer: A Secondary Analysis of a Randomized Clinical Trial
Authors: Adnan Ali, Alex Hoyle, Áine M. Haran, Christopher D. Brawley, Adrian Cook, Claire Amos, Joanna Calvert, Hassan Douis, Malcolm D. Mason, David Dearnaley, Gerhardt Attard, Silke Gillessen, Mahesh K. B. Parmar, Christopher C. Parker, Matthew R. Sydes, Nicholas D. James, Noel W. Clarke
Read the Full Article published in JAMA Oncology.

RAMPP showed significant CSM benefit for the addition of RP (5-yr rates: 13% vs 23%). Clinical progression was similar. Albeit promising, we should note that CSM has never been shown to be a good surrogate endpoint for OS in advanced PCa.
Actually no intermediate endpoint has been confirmed as a valid surrogate. CSM has too many pitfalls, including attribution uncertainty, and other-cause mortality being reassuring does NOT rule out bias in attributed cases.
Title: Meta-Analysis of Candidate Surrogate End Points in Advanced Prostate Cancer
Authors: Laila A. Gharzai, Ralph Jiang, Elizabeth M. Jaworski, Krystal Morales Rivera, Robert T. Dess, William C. Jackson, Holly E. Hartman, Rohit Mehra, Amar U. Kishan, Abhishek A. Solanki, Edward M. Schaeffer, Felix Y. Feng, Nicholas G. Zaorsky, Alejandro Berlin, Lee Ponsky, Jonathan Shoag, Yilun Sun, Matthew J. Schipper, Jorge Garcia, Daniel E. Spratt
Read the Full Article published in NEJM Evidence.

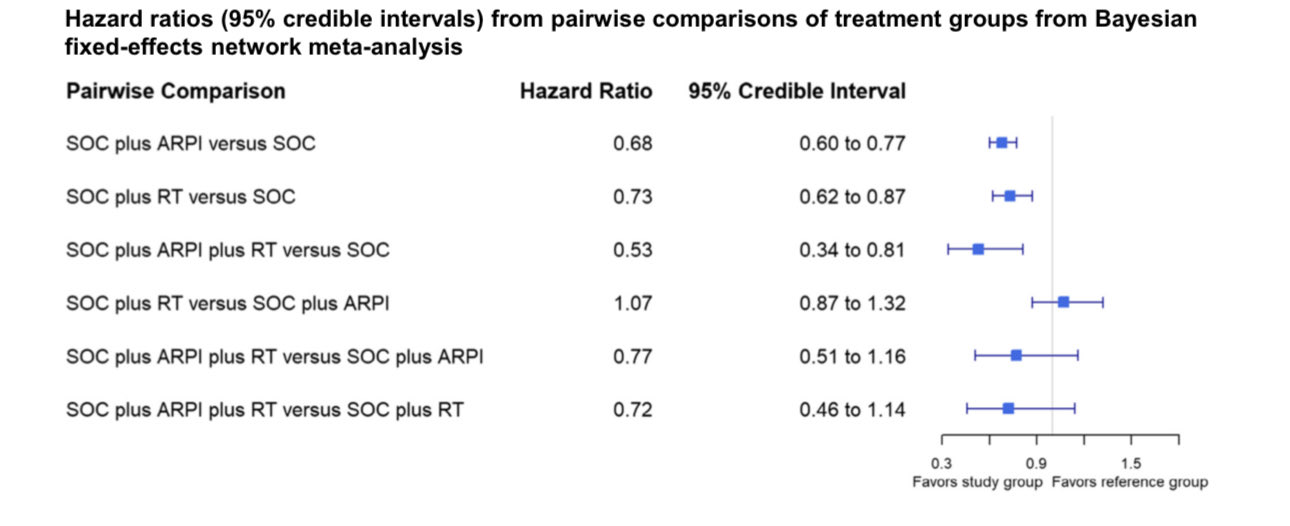
There was a promising signal in OS, however NOT confirmed, with a p=0.13. RT has a proven OS benefit in the context of ADT alone, even in a higher disease burden population, as shown in Soumyajit Roy (Soum) network meta-analysis. Also, there was a good trend for OS benefit in the context of ADT+ARPI. STOPCAP has shown a 7% OS improvement at 3 years.
Title: Prostate Radiotherapy in Low-volume Metastatic Hormone-sensitive Prostate Cancer: A Network Meta-analysis
Authors: Soumyajit Roya, Gagan Fervahab, Daniel E. Sprattc, Yilun Sund, Amar U. Kishane, Andrew Loblawf, Shawn Maloneg, Michael Ongh, Fred Saadi, Christopher J.D. Wallisc, Scott C. Morgan
Read the Full Article published in EUROPEAN ONCOLOGY.

There was 14% G3+ surgery-specific complications in RAMPP. In STAMPEDE, RT was associated with ~6% G3+ toxicity, and PEACE-1 RT toxicity profile was quite similar.
IMO, RT remains the only proven local treatment to the primary in the setting of low-burden mHSPC, including oligometastatic disease not treated with metastases-directed therapy, as it has a proven OS benefit, and a favorable toxicity profile. RAMPP does not confirm an OS benefit for RP, and CSM is not a robust surrogate, at least not proven to be one.
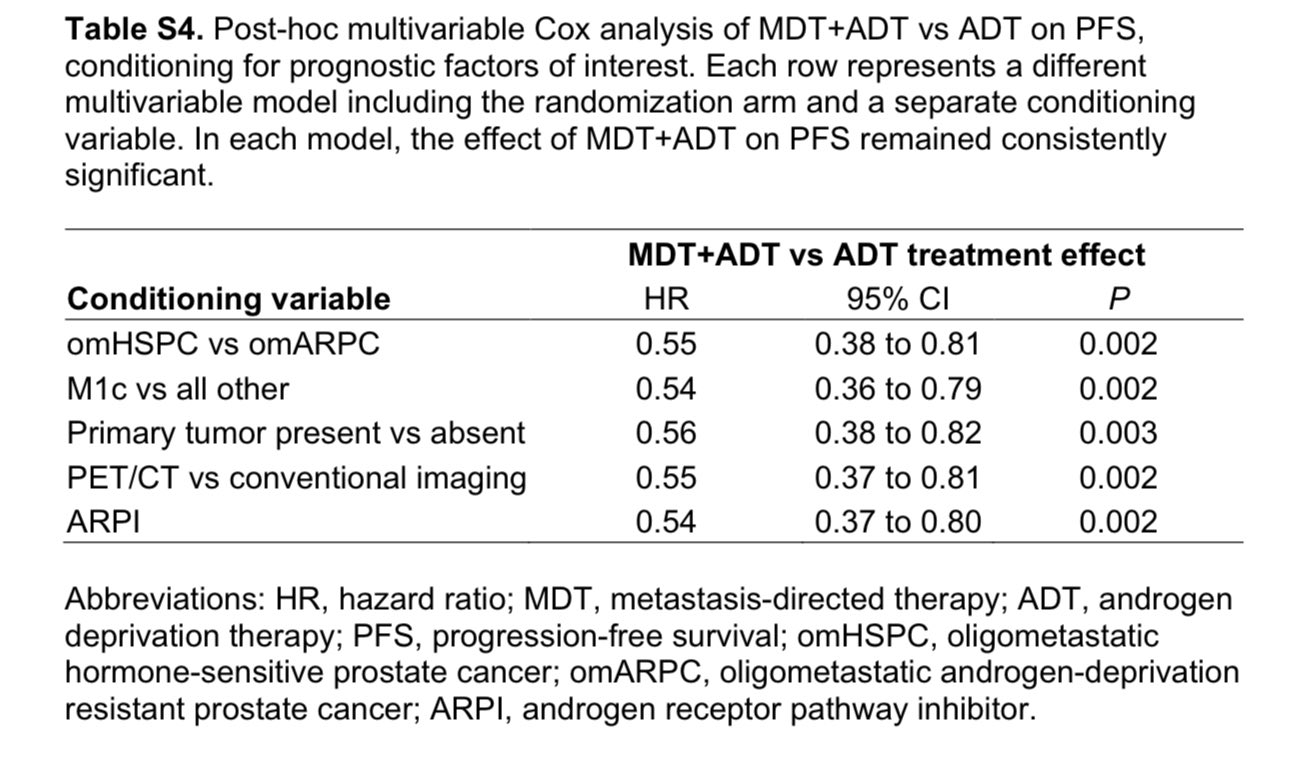
The field is moving towards MDT for oligometastatic disease, however we still eagerly await ongoing RCTs. EXTEND trial included 30% synchronous oligometastatic disease, where the primary was treated with RT. FWIW, MDT showed consistent PFS benefit on post-hoc multivariable analysis, regardless of synchronous vs metachronous setting. Alex Sherry.
Such data is lacking for RP.
Title: Continuous Androgen Deprivation Therapy with or Without Metastasis-directed Therapy for Oligometastatic Prostate Cancer: The Multicenter Phase 2 Randomized EXTEND Trial
Authors: Alexander D. Sherrya, Bilal A. Siddiquib, Cara Haymakerc, Bryan M. Fellmand, Marina N. Medina-Rosalesc, Tharakeswara K. Bathalae, Shuqi Wangd, Suyu Liud, Aaron Seoa, Kieko Harac, Hsinyi Luc, Patricia Troncosof, Stephen G. Chuna, Chul S. Hag, Lauren L. Mayoa, Henry Mokh, Ryan J. Parkh, Brian F. Chapini, Ryan M. Phillipsj, Matthew P. Deekk, Craig A. Kovitzl, Ana Apariciob, Amado J. Zuritab, Patrick G. Pilieb, Lorenzo Cohenm, Seungtaek L. Choih, Alexandre Reubeno, Phuoc T. Tranp, Paul G. Cornb, Sumit K. Subudhib, Chad Tang
Read the Full Article published in EUROPEAN ONCOLOGY.

In summary, the role of RP in the setting of oligometastatic or low-burden mHSPC remains to be proven. IMHO, the authors’ conclusion in the RAMPP paper is a bit overreaching, and I don’t think the results robustly support the addition of RP in this setting. I’m eager to know what others think about these results.”
More posts featuring Tyler Seibert on OncoDaily.
{kind=link}
{kind=link}