


Olubukola Ayodele, Breast Cancer Lead at University Hospitals of Leicester NHS Trust , shared a post on LinkedIn:
“ESMO25 | Presidential Session Highlights Day 2
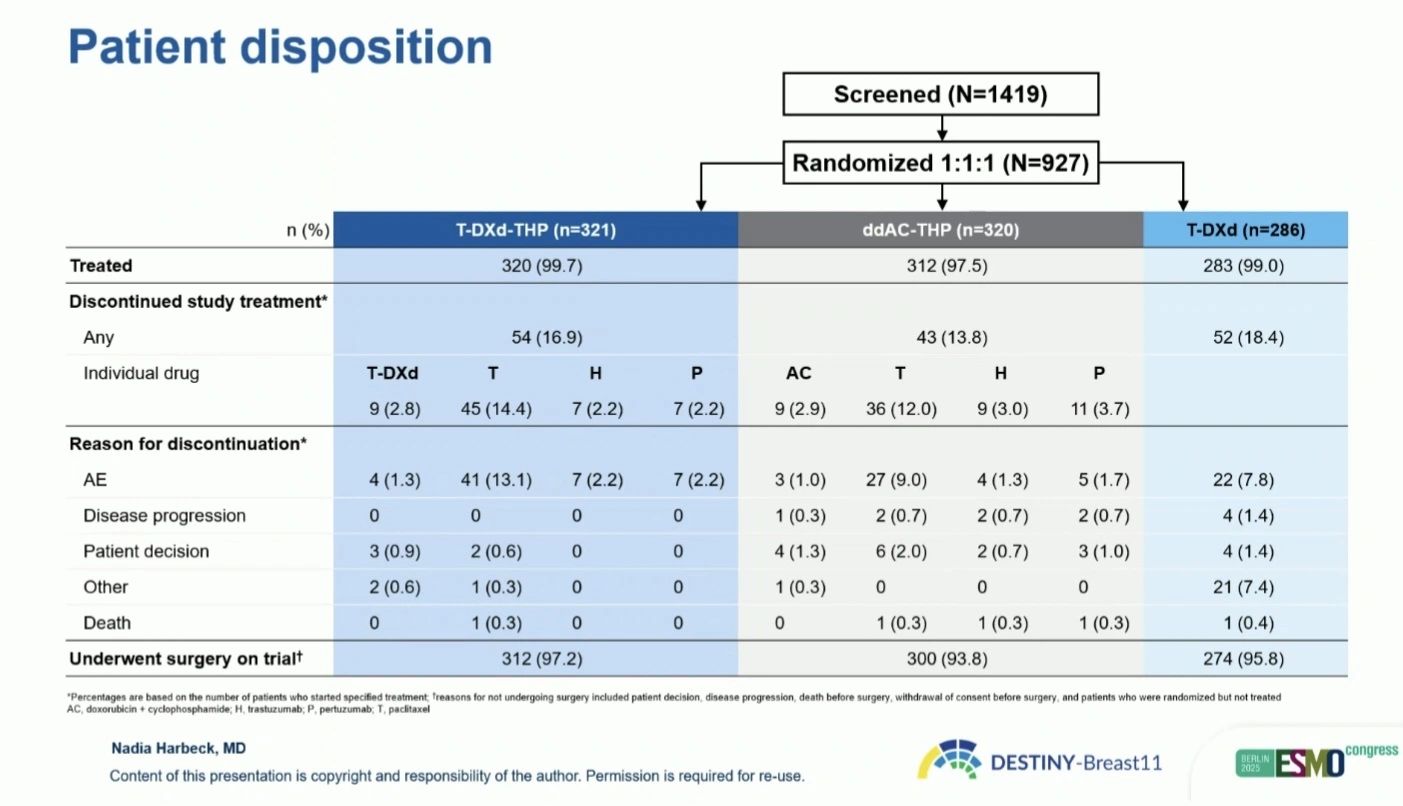
One of the most practice-defining presentations today was DESTINY-Breast11, evaluating trastuzumab deruxtecan (T-DXd) in the neoadjuvant setting for high-risk, HER2-positive early breast cancer.
Trial design:
Phase 3, multicentre, open-label randomisation to:
- T-DXd + trastuzumab + pertuzumab (T-DXd–THP)
- Dose-dense doxorubicin/cyclophosphamide → THP (ddAC–THP)
(The T-DXd monotherapy arm was closed early due to lower pCR rates)
Key results:
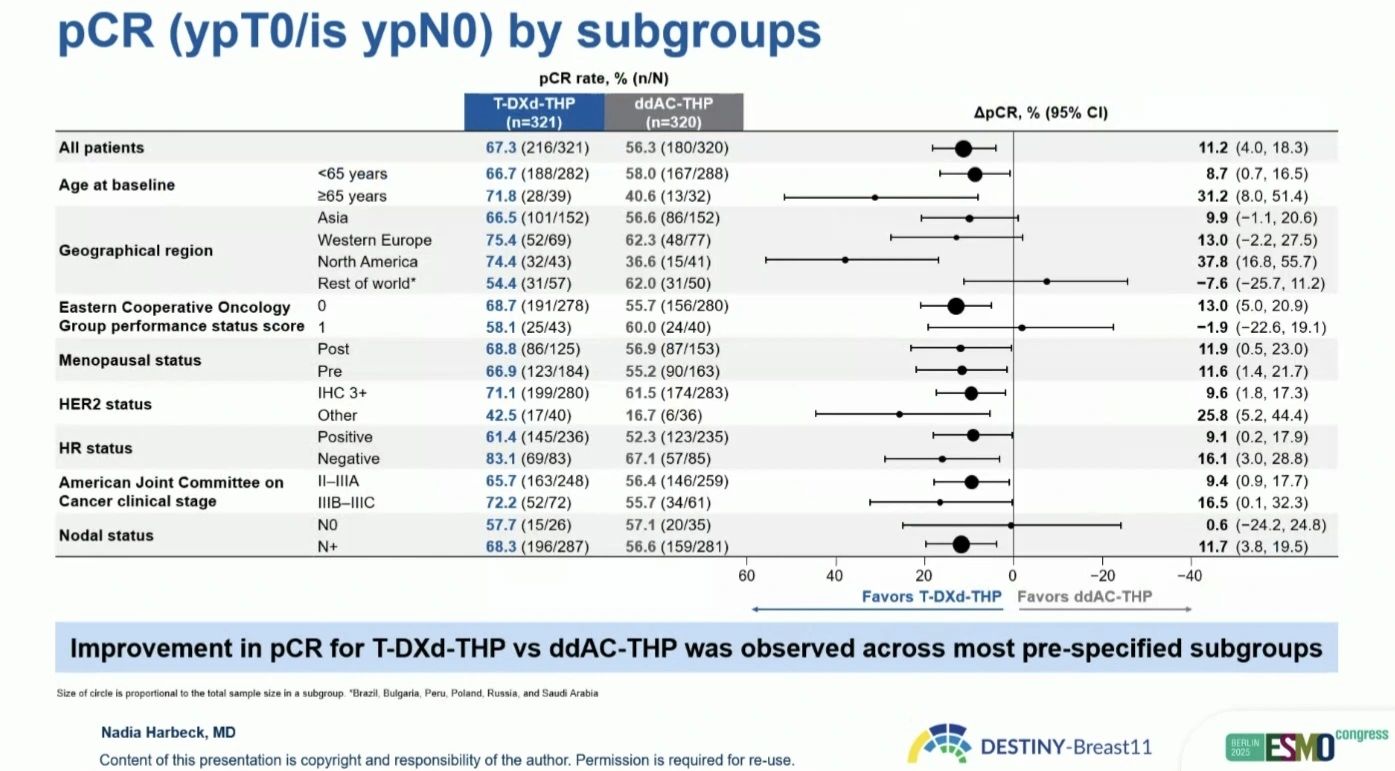
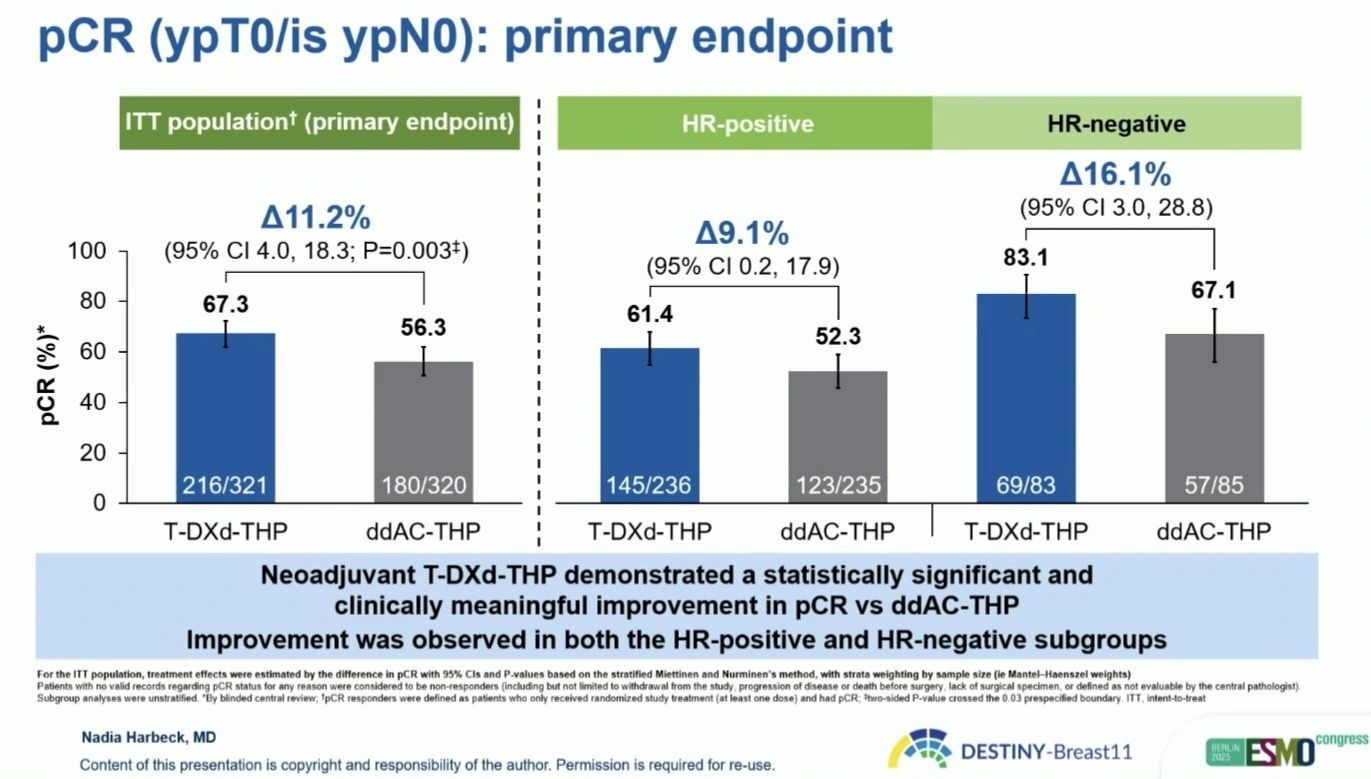
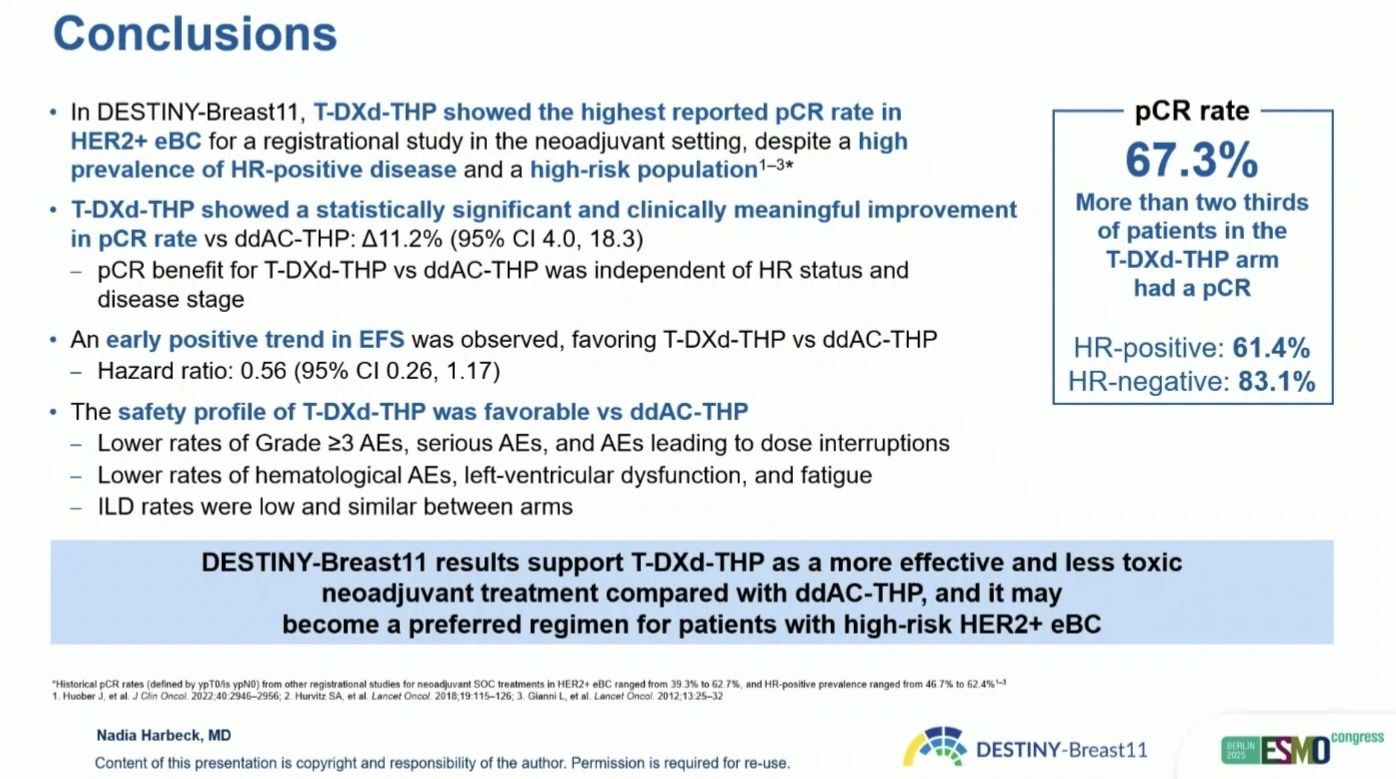
- pCR: 67.3% (T-DXd–THP) vs 56.3% (ddAC–THP) → Absolute benefit: +11.2% (95% CI 4.0–18.3; p = 0.003)
- HR+ disease: 61.4% vs 52.3%
- HR– disease: 83.1% vs 67.1%
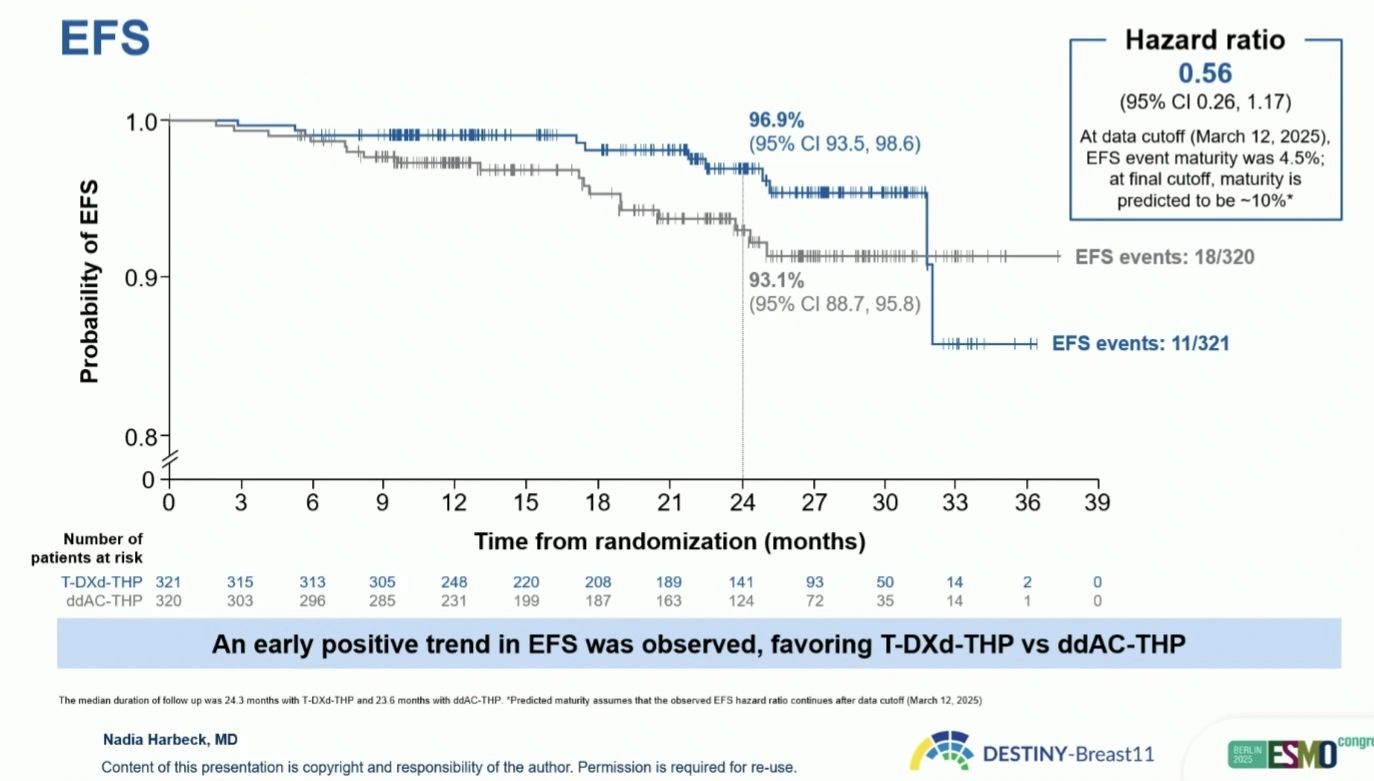
- Early EFS trend: HR 0.56 (95% CI 0.26–1.17)
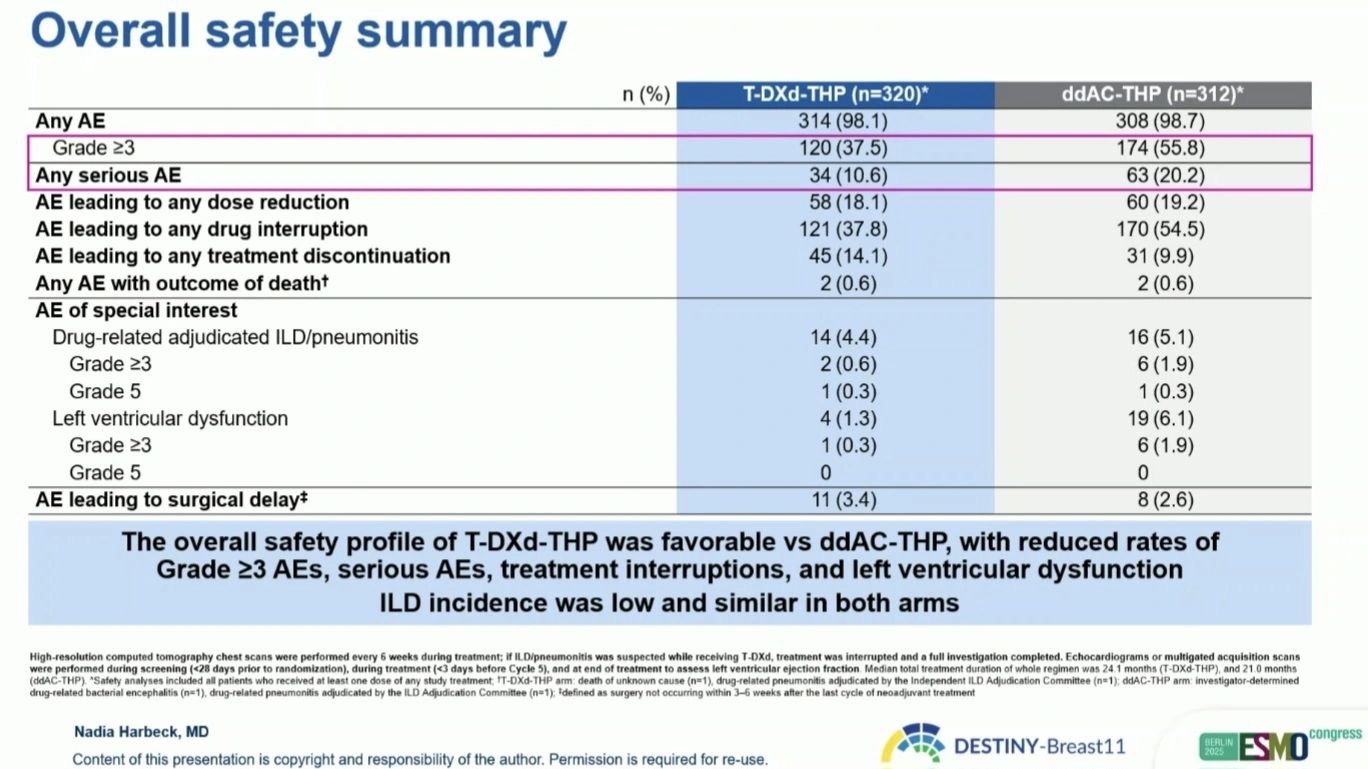
- Grade ≥3 AEs: 37.5% vs 55.8%
- ILD/pneumonitis: 4.4% vs 5.1%
- LV dysfunction: 1.9% vs 9.0%
No adverse event prevented surgery in either arm.
Clinical meaning:
DESTINY-Breast11 is the first phase 3 trial showing that an anthracycline-free, ADC-based regimen can deliver superior pCR rates with lower toxicity compared to ddAC–THP, potentially rewriting the standard of care for high-risk HER2+ disease.
But with every advance comes complexity.
What happens next?
If patients relapse after neoadjuvant T-DXd, what do we treat them with in the metastatic setting?
T-DXd is already a standard post-T-DM1 in advanced HER2+ disease but if it’s used upfront, resistance mechanisms (such as HER2 loss, drug efflux, or payload-related cross-resistance) could limit later-line ADC options.
We may see earlier use of T-DM1, trastuzumab duocarmazine, or HER2 bispecifics, but this sequencing challenge will require new strategies and molecular profiling at relapse.
Pragmatically:
T-DXd–THP could help us move toward a chemo-light, cardioprotective, curative pathway, but we must balance cure with stewardship. Overuse of ADCs too early could compromise future lines of therapy in those who recur.
The key will be selecting the right patients: those truly at high risk of relapse, not every HER2+ case.
A remarkable step forward but one that must be navigated wisely.”

You can also read: ESMO 2025 Day 2 Highlights Not to Miss

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}