


Olubukola Ayodele, Breast Cancer Lead at University Hospitals of Leicester NHS Trust, shared a post on LinkedIn:
“Day 2 SABCS25 update
LidERA
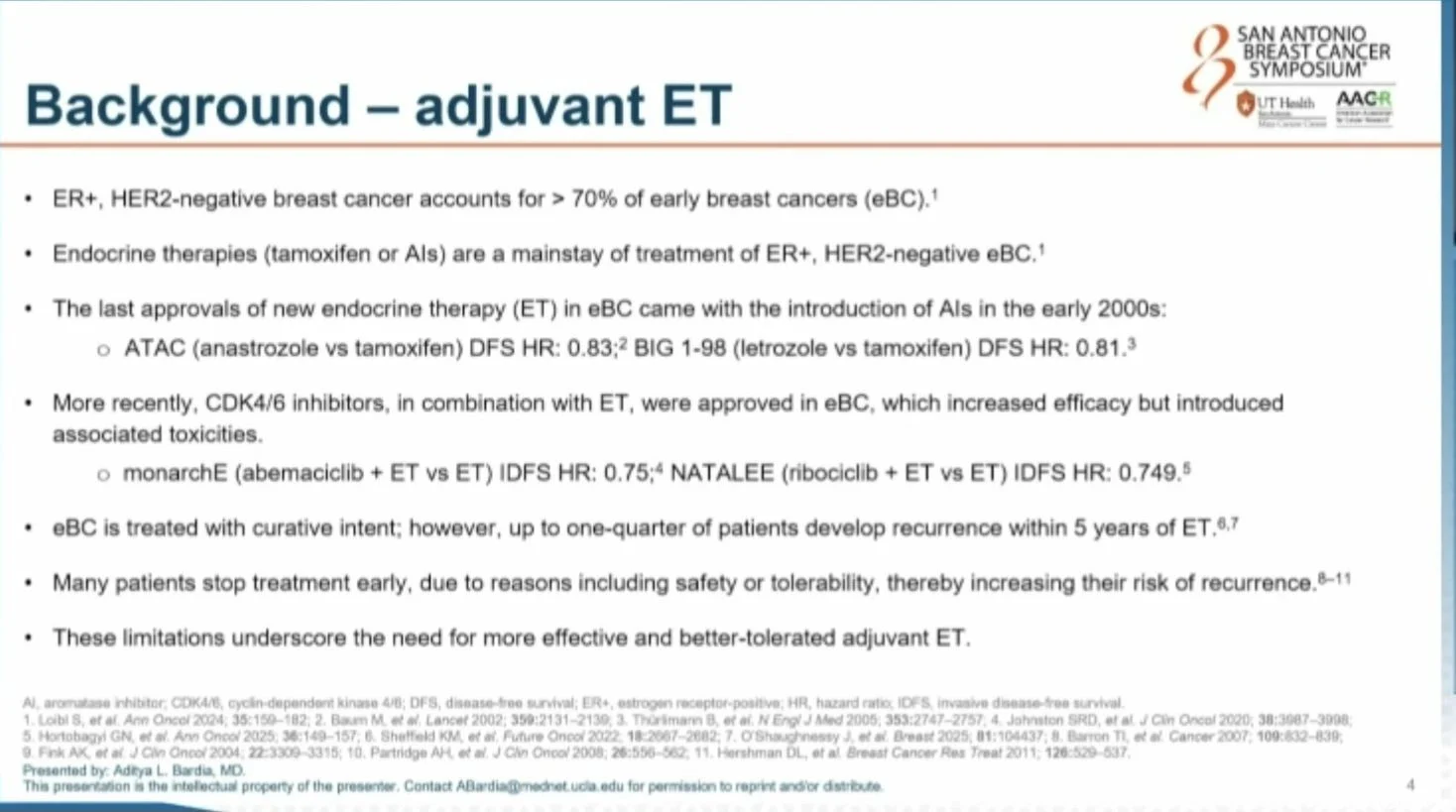
• ER+/HER2– early breast cancer is the most common subtype.
• Endocrine therapy works, but adherence and tolerability remain challenges.
• No truly new adjuvant endocrine option has been approved since Aromatase Inhibitors.
• Giredestrant is an oral SERD designed for deeper ER blockade.
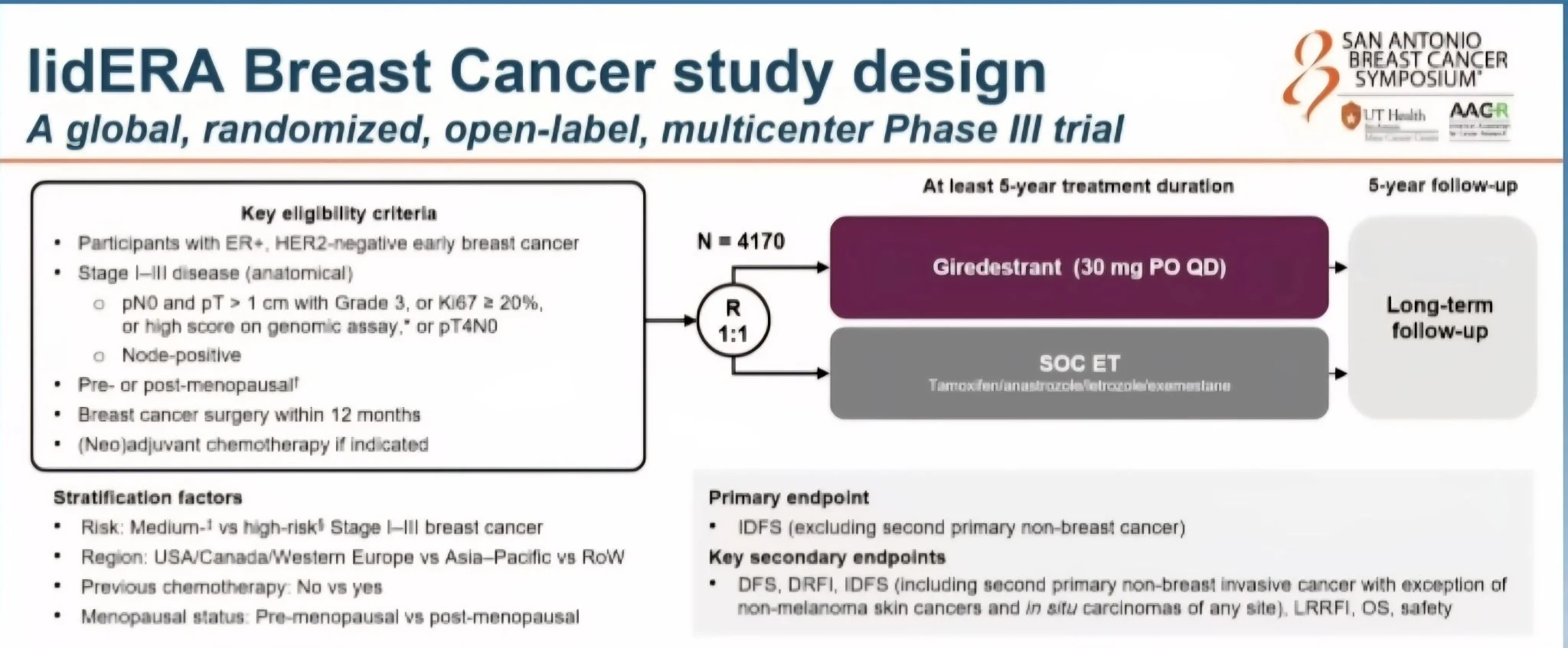
Trial Design
* Global, Phase III, open-label trial.
• 4170 patients with Stage I–III ER+/HER2– breast cancer.
• Randomised 1:1 to giredestrant 30 mg daily vs standard ET (tamoxifen or AI).
• Planned ≥5 years of treatment.
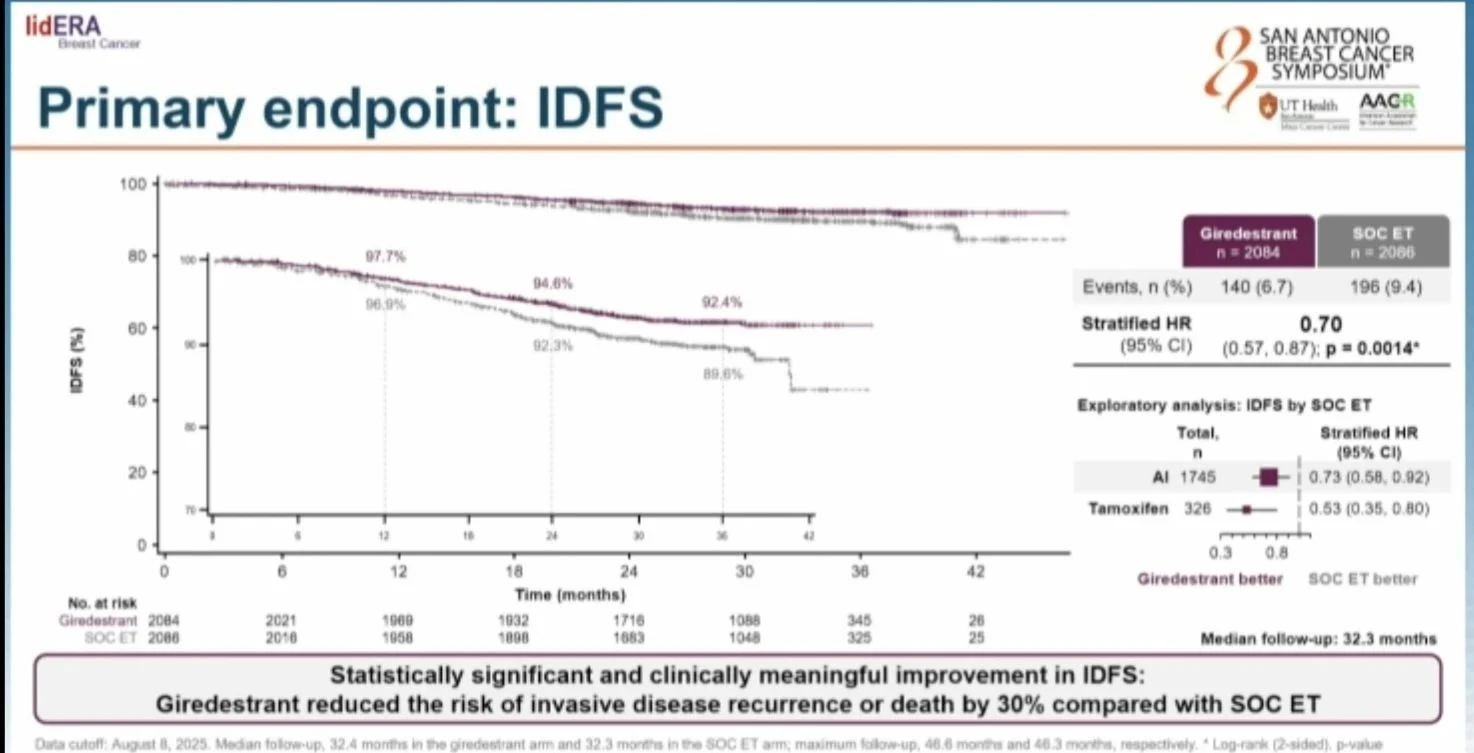
• Primary endpoint: invasive disease-free survival (IDFS).
Key Results
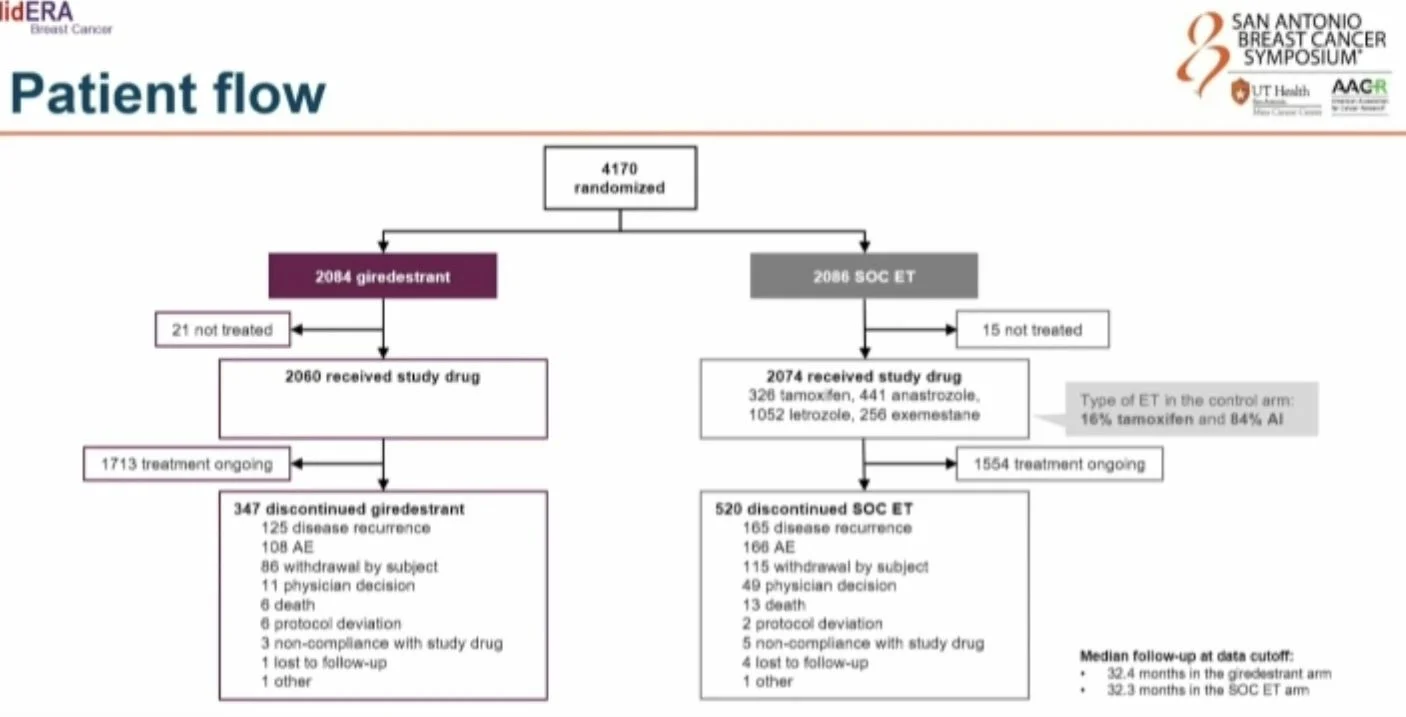
• Median follow-up: 32.3 months.
• 3-year IDFS: 92.4% (giredestrant) vs 89.6% (SOC).
• IDFS improved: HR 0.70 (95% CI 0.57–0.87; p=0.0014).
• Benefit consistent across stage, menopausal status, chemo exposure and regions.
• Distant recurrence-free interval improved (HR 0.69).
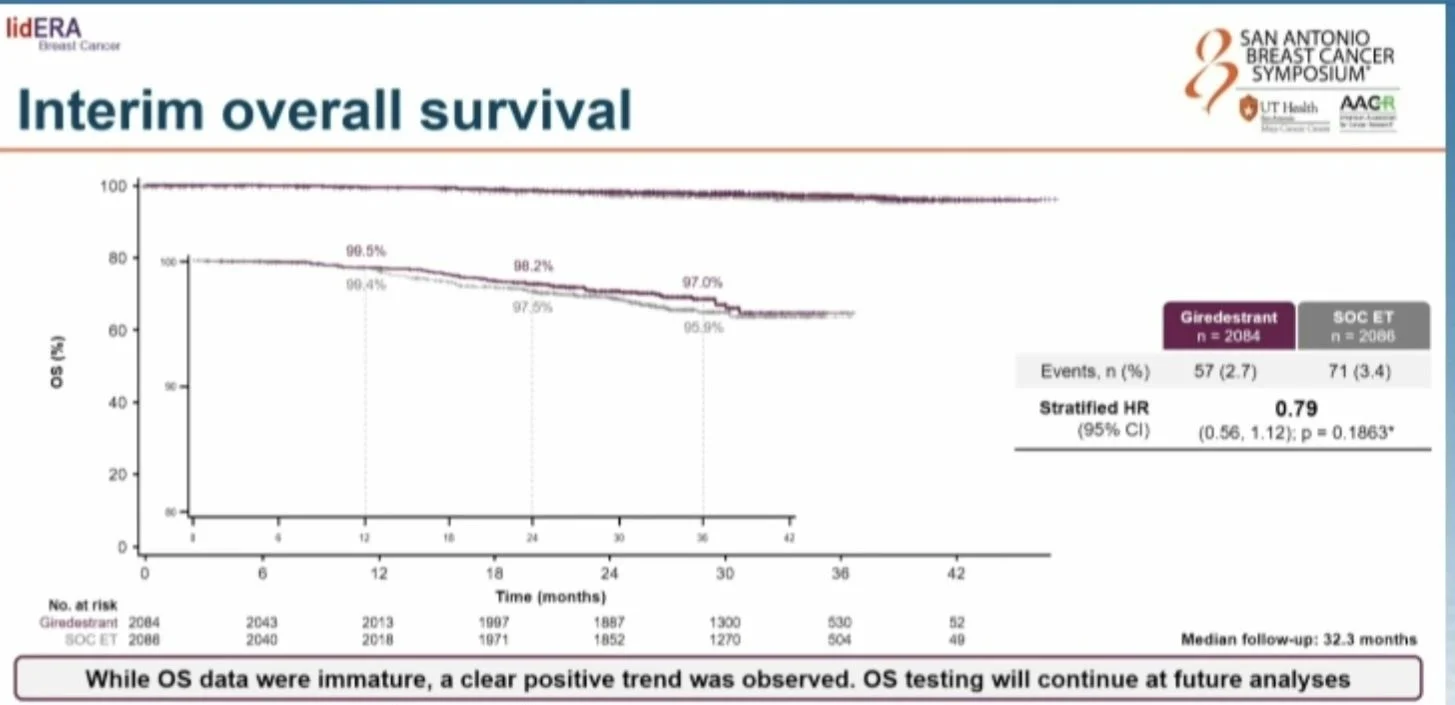
• Early overall survival shows a positive trend (immature).
Toxicity
• Safety profile similar to standard ET.
• Grade 3–4 and serious AEs comparable between arms.
• Lower treatment discontinuation with giredestrant (5.3% vs 8.2%).
• Fewer musculoskeletal and vasomotor-related discontinuations.
Why It Matters
• First meaningful advance in adjuvant endocrine therapy since AIs.
• Absolute benefit of <3%, however, similar to current combination strategies with CDK4/6 inhibitors at the time of follow up, suggesting that benefit will continue to grow.
• Potential to become a new standard for HR+/HER2– early breast cancer.
Caution
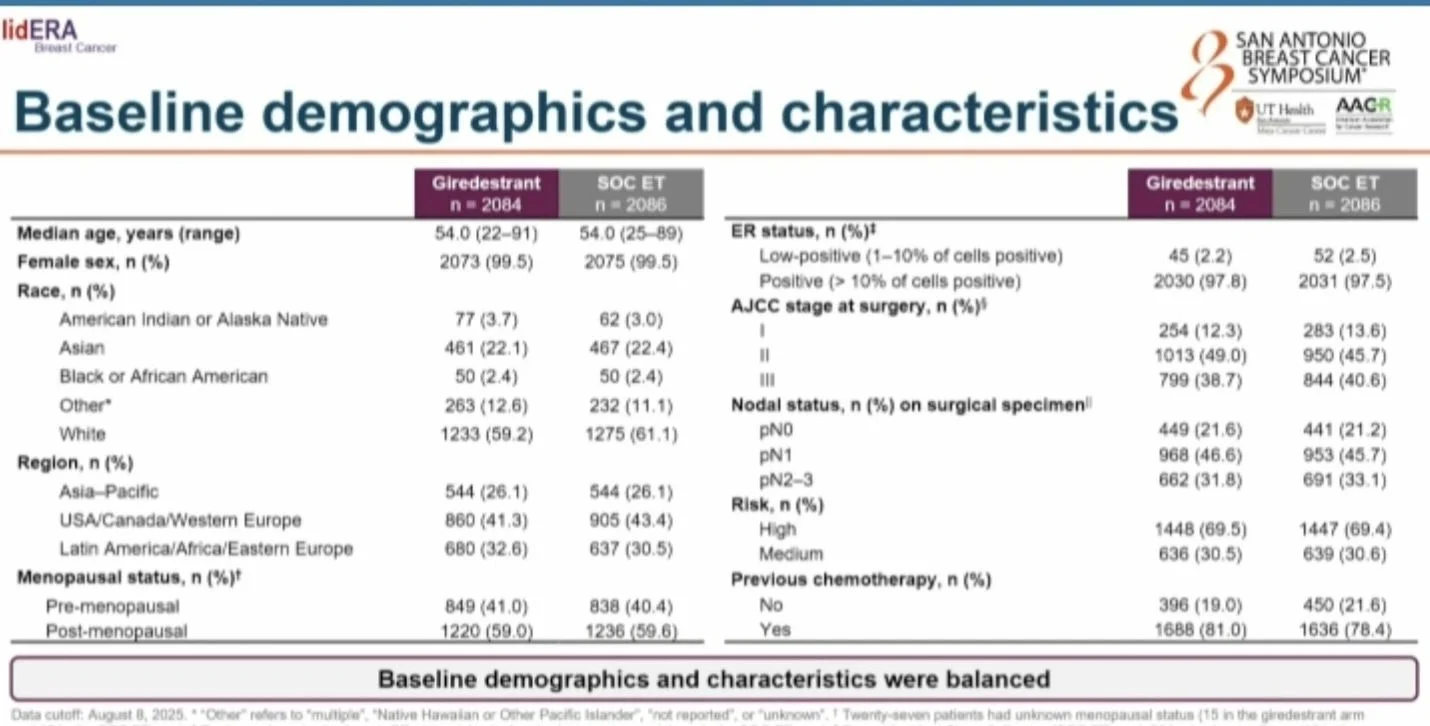
* Control arm not currently soc especially with >80% being N+, as those patients would be offered a CDK4/6 inhibitor combo.
* Financial toxicity
* Less treatment options on progression for metastatic disease.
However, it’s great to see positive progress since AIs.”

You Can Also Read:
15 Posts Not to Miss from SABCS 2025, Part 1
20 Posts Not to Miss from SABCS 2025, Part 2

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}