


Al-Ola Abdallah, Board Member at Kansas Society OF Clinical Oncology, Associate Professor of Medicine, Assistant Professor at University of Kansas Medical Center, shared a post on X:
“Cilta-cel in High-Risk Smoldering Myeloma (CAR-PRISM, Phase 2)
Groundbreaking – but let’s stay critical and take a look at this closely from all angles.
1. Concept shift: Treating precursor disease (HR-SMM) with CAR-T
Aim: intercept progression, maybe even cure.
Rationale:
- Lower tumor burden
- Better T-cell fitness
- Less immune exhaustion
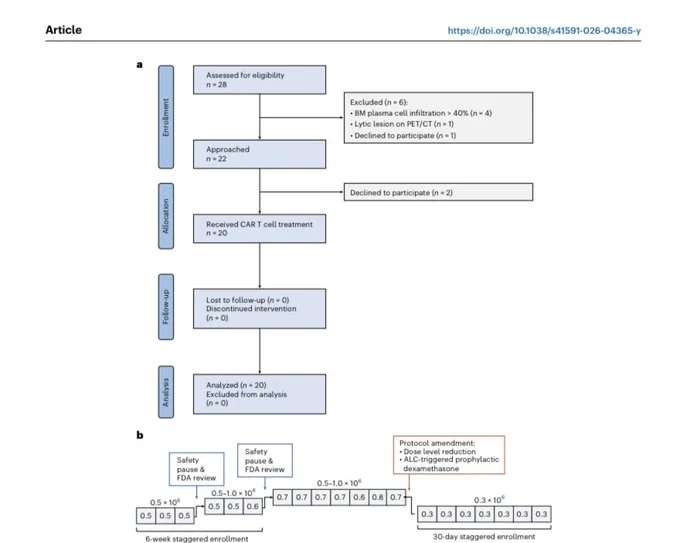
2. Study design
- Phase 2, single-center
- n = 20 treated patients
- No induction, no bridging
- Cilta-cel upfront
- Primary: safety
- Secondary: MRD, response
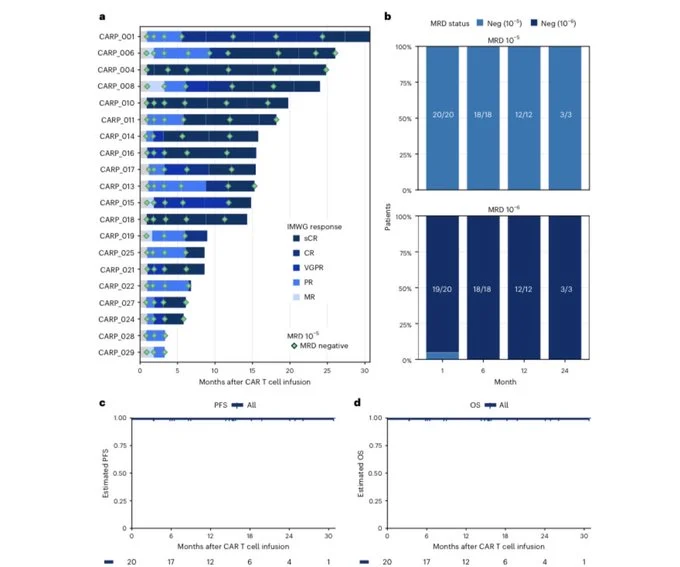
3. Efficacy = Not surprising
- 100% MRD negativity (10⁻⁶) by ~2 months
- 90% CR/sCR
- No progression or deaths (median FU 15.3 mo)
Fast + deep + sustained responses
- All patients MRD(-) at 10⁻⁶
- Sustained across timepoints
Compared to prior trials:
- KRd-based strategies ~50-60% MRD(-)
- CAR-T clearly deeper
Let’s get into business
4. Toxicity profile
- CRS: 100% (ALL grade 1–2)
- Cytopenias: common but transient
- NINTs (non-ICANS neurotoxicity): 35%
Cranial nerve palsies + movement disorders
New neurotoxicity phenotype emerging.
5. Neurotoxicity signal (important!)
- Associated with elevated CAR-T expansion and ALC
- Some persistent grade 1 symptoms
Raises concern for:
- Parkinsonian features
- Long-term neurologic risk
Mechanism still unclear.
6. Critiques/Limitations
- Small sample size (n=20)
- No statistical power
- Rare toxicities likely missed
Signals ≠ definitive conclusions
7. Single-arm, no comparator
- No randomized control
- Cannot compare vs:
- Dara
- KRd-based early intervention
Magnitude of benefit unclear.
8. Short follow-up (15 months)
- SMM is a long disease course
Key unanswered:
- Are we curing disease?
- Or just delaying progression?
Durability remains unknown.
9. Overtreatment risk
SMM ≠ always destined to progress
Treating all HR-SMM with CAR-T:
- Cost
- Toxicity
- Resource burden
Risk-benefit balance unclear.
10. Neurotoxicity concerns
- Novel NINTs (movement disorders)
- Some persistent
In asymptomatic patients – big issue
Tolerance threshold is much lower vs RRMM
11. No QoL data
- Hospitalization
- Toxicity burden
- Long-term function
Critical in asymptomatic population.
12. Big picture takeaways
Proof-of-concept: CAR-T can induce deep MRD(-) in SMM
But:
- Not practice-changing yet
- Needs randomized trials + long-term data
Bottom Line: I will not feel comfortable to treat HRSMM with Cilta-Cel!
Even on a clinical trial.”
Title: Ciltacabtagene autoleucel in high-risk smoldering multiple myeloma: the CAR-PRISM phase 2 trial

Other articles featuring Al-Ola Abdallah on OncoDaily.
{kind=link}
{kind=link}