
Krishan Jethwa: ESOPEC practice shifting trial at ASCO24
Krishan Jethwa, Assistant Professor of Radiation Oncology at Mayo Clinic, shared on X:
”ESOPEC.
Practice shifting trial.
Patients with resectable, locally advanced, esophagus/GEJ adenocarcinoma.
Randomized Peri-op FLOT (FLOT4) vs Pre-operative chemoradiation (CROSS).
Congratulations to the study investigators!
Let’s dive in!

First… Background. Both Peri-operative chemotherapy (MAGIC/FLOT4) and pre-operative chemoradiation (CROSS) are standard of care treatment options for patients with resectable, locally advanced, esophagus/GEJ adenocarcinoma. Each has demonstrated: Improved OS.
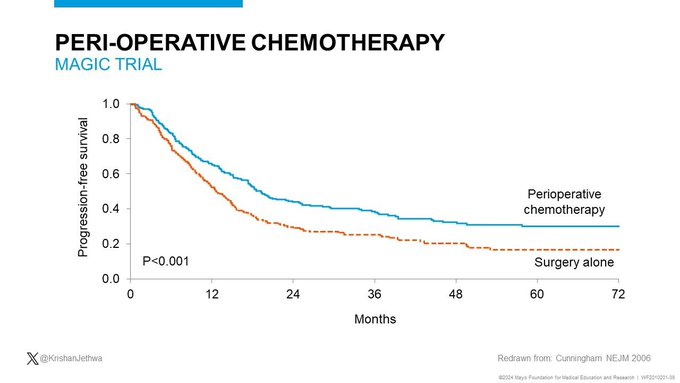
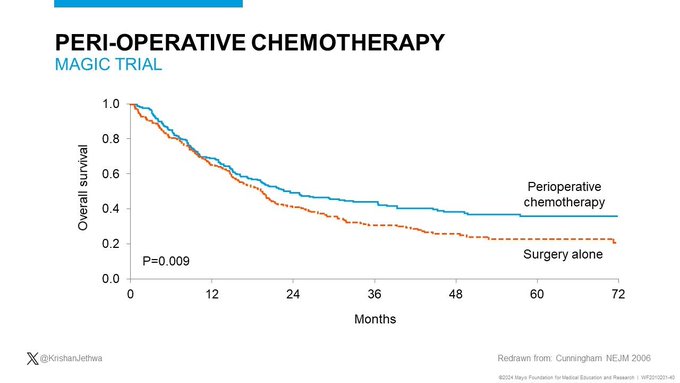
MAGIC trial included patients with GEJ or gastric adenocarcinoma. Randomized patients to: Up-front surgery vs Peri-operative ECF chemotherapy. Peri-operative ECF was associated with:
- Improved OS,
- Improved DFS.

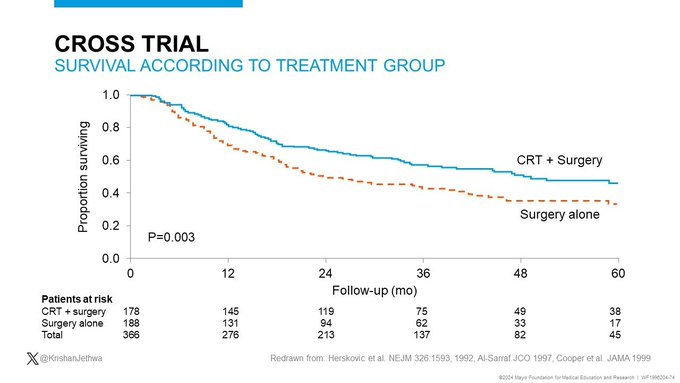
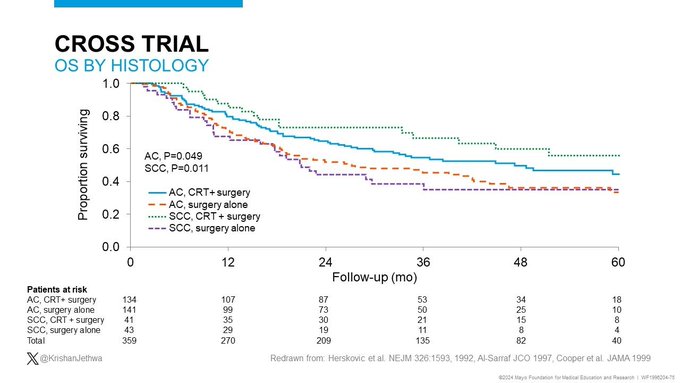
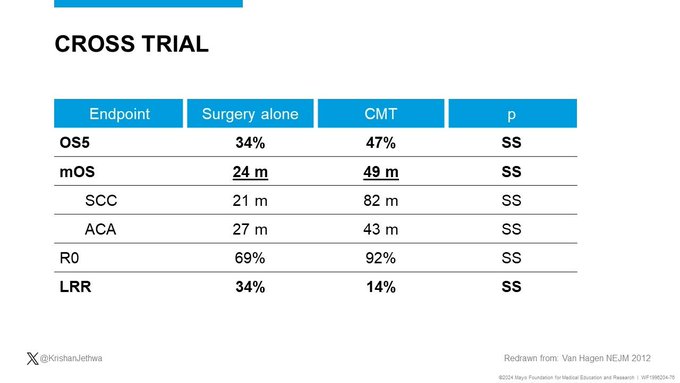
CROSS trial included patients with resectable, LA esophagus/GEJ cancer. Randomized patients to: Up-front surgery vs Pre-operative carbo-taxol based CRT, 41.4 Gy/23. CRT Improved:
- OS ,
- DFS,
- Locoregional control,
- 29% pCR.

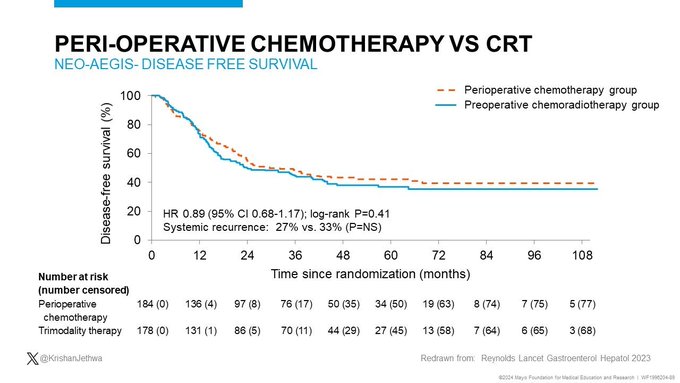
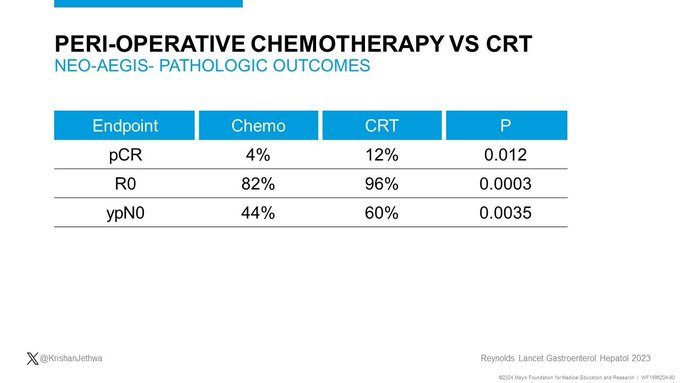
NEO-AEGIS included patients with resectable, LA esophagus/GEJ cancer. Randomized Peri-op chemotherapy (MAGIC) vs Pre-op chemoradiation (CROSS). Findings:
- Comparable OS3 (55% vs 57%),
- Comparable DFS,
- Improved R0 and pCR with CRT,
- Equipoise, BUT, practice evolved.

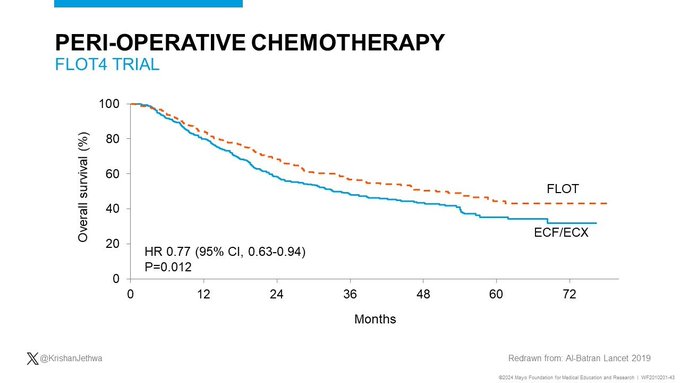
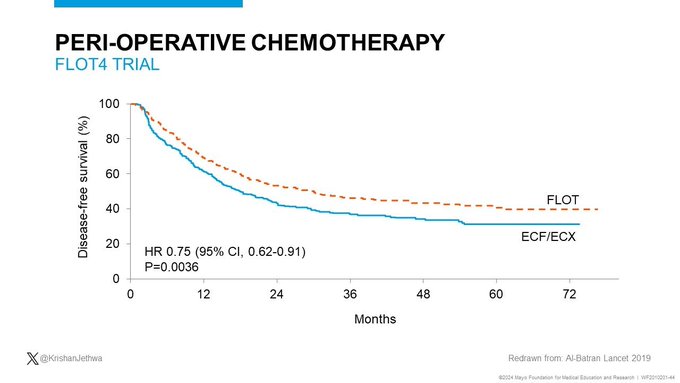
FLOT4 Trial included patients with resectable GEJ or gastric adenocarcinoma. Randomized patients to: Peri-operative ECF vs Peri-operative FLOT. FLOT improved:
- OS,
- DFS,
- FLOT became new standard of care.

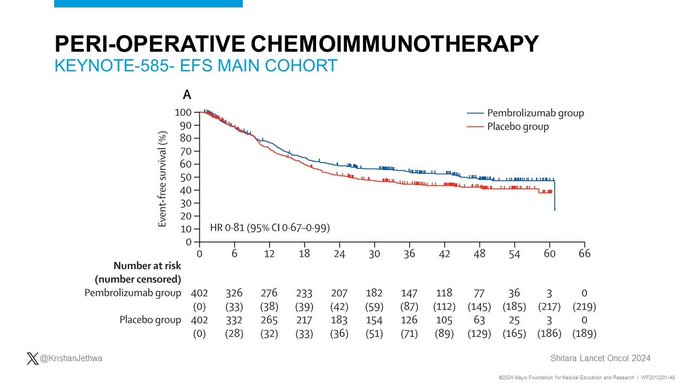
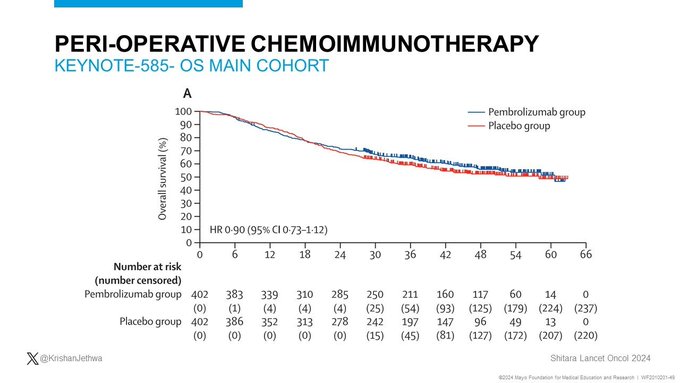
KN-585, MATTERHORN, DANTE are exploring peri-operative chemotherapy (Cis/FU or FLOT) +/- ICI (Pembro/Durva/Atezo) for resectable, LA Gastric/GEJ adenocarcinoma, respectively:
- KN-585: = OS; increased EFS,
- MATTERHORN/DANTE: increased pCR, EFS maturing.
At present, FLOT remains standard of care.

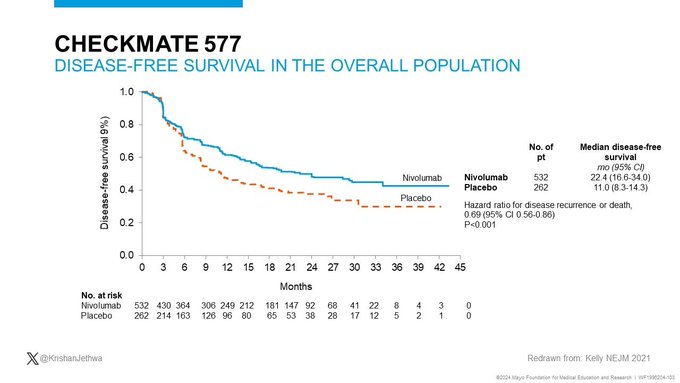
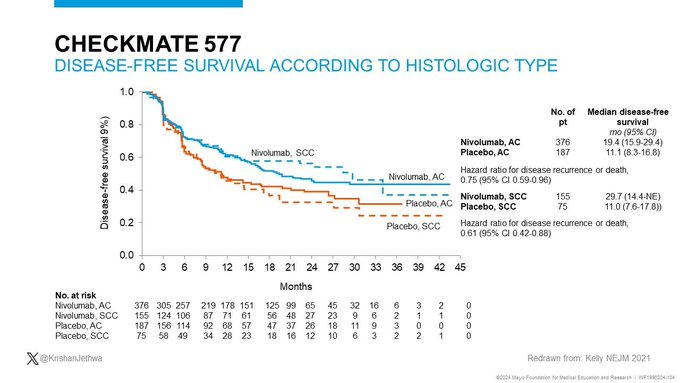
CM-577 included patients with resectable, LA E/GEJ or gastric cancer status post pre-operative chemoradiation and esophagectomy. Patients with path residual disease randomized to: Placebo vs Nivolumab x 12m. Nivolumab improved:
- mDFS 22m vs. 11m,
- CM-577 regimen is now standard of care.

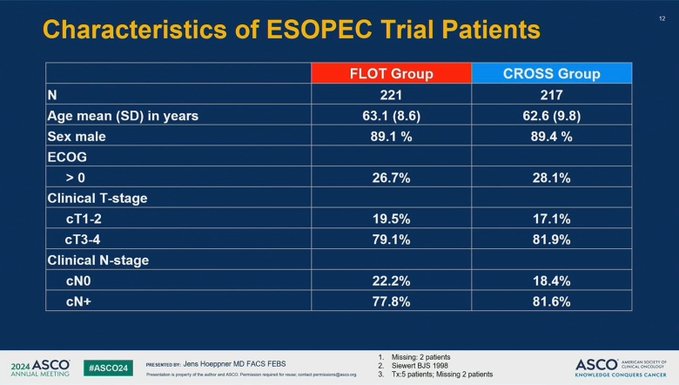
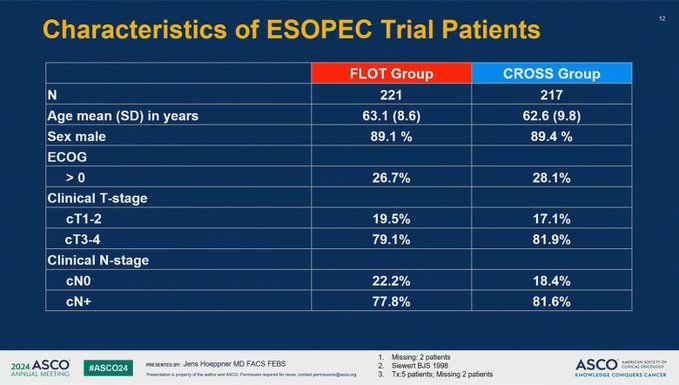
ESOPEC.
Resectable, cT2+ or N+, E/GEJ adenocarcinoma.
Peri-op FLOT (FLOT4) vs Pre-op CRT (CROSS; no ICI if < pCR).
N=438.
81% T3-4; 80% N+
Outcomes:
- Only 68% completed nCRT.
- R0 94% vs 95%.
- pCR: 19% vs 14%.
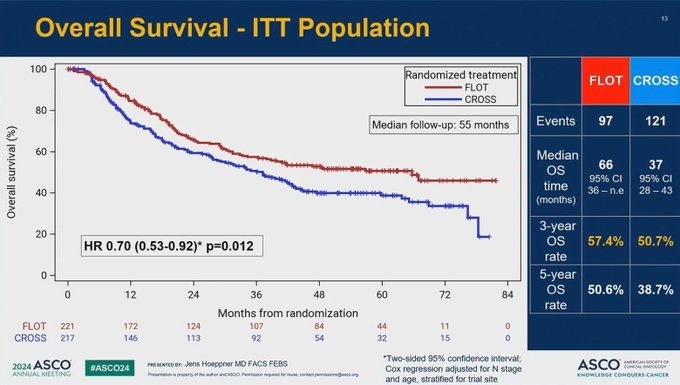
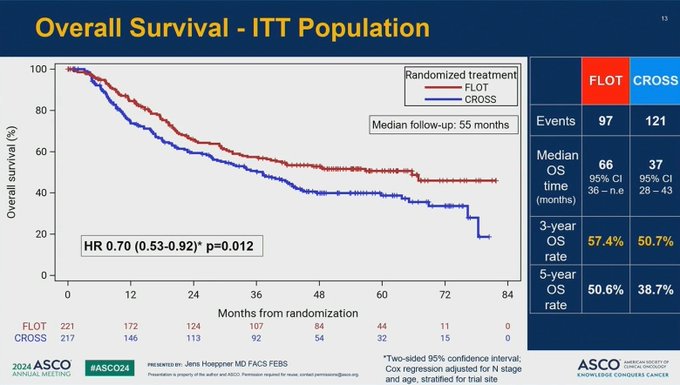
- FLOT increased mOS 66m vs 37m.
- FLOT increased OS3 57% vs 51%.

Takeaways:
- FLOT should be a standard of care.
BUT:
- Is FLOT > CM-577 regimen,
- Toxicity,
- E vs GEJ (S1/2 vs S3),
- Poorer pCR/OS compared with CROSS,
- TNT
If FLOT ineligible or not a surgical candidate, CRT is preferred.
Takeaways 2:
- Peri-op chemotherapy and CRT increased OS.
- Each works by independent mechanism.
- Outcomes in LA esophagus cancer remain sub-optimal (OS3 50-57%).
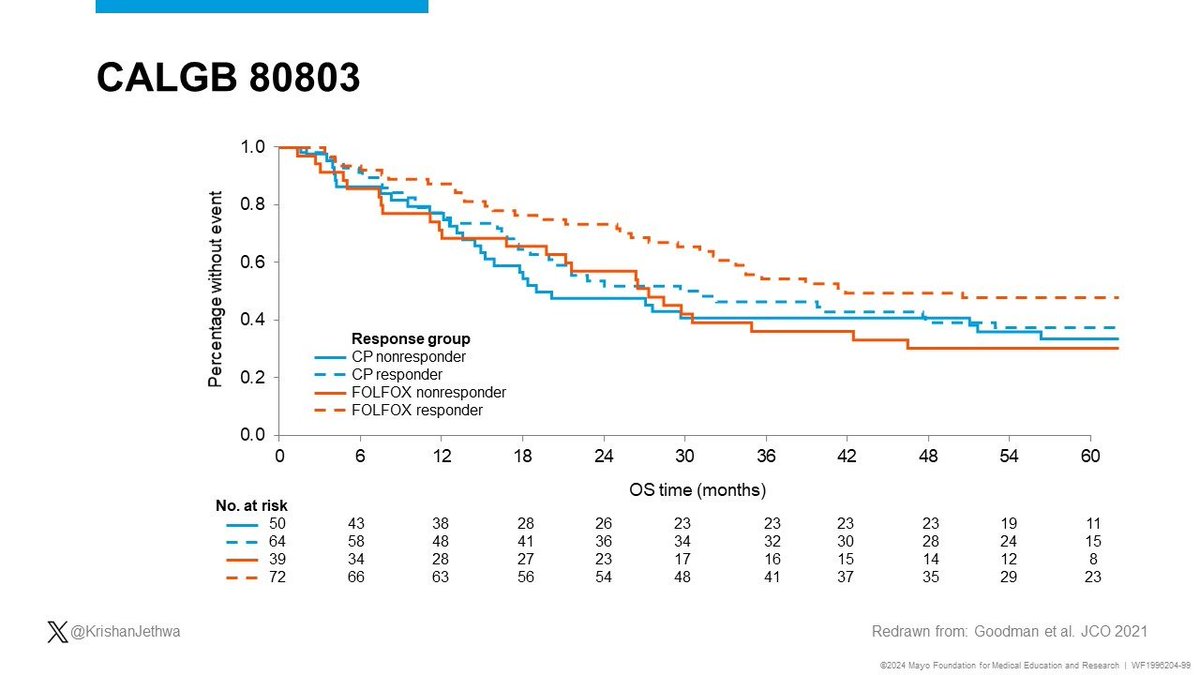
- Combined modality (rather than competing) peri-op strategies should be investigated in future trials!
EG. CALGB 80803.

To balancing QoL and cancer control, organ preservation with CRT should be considered.
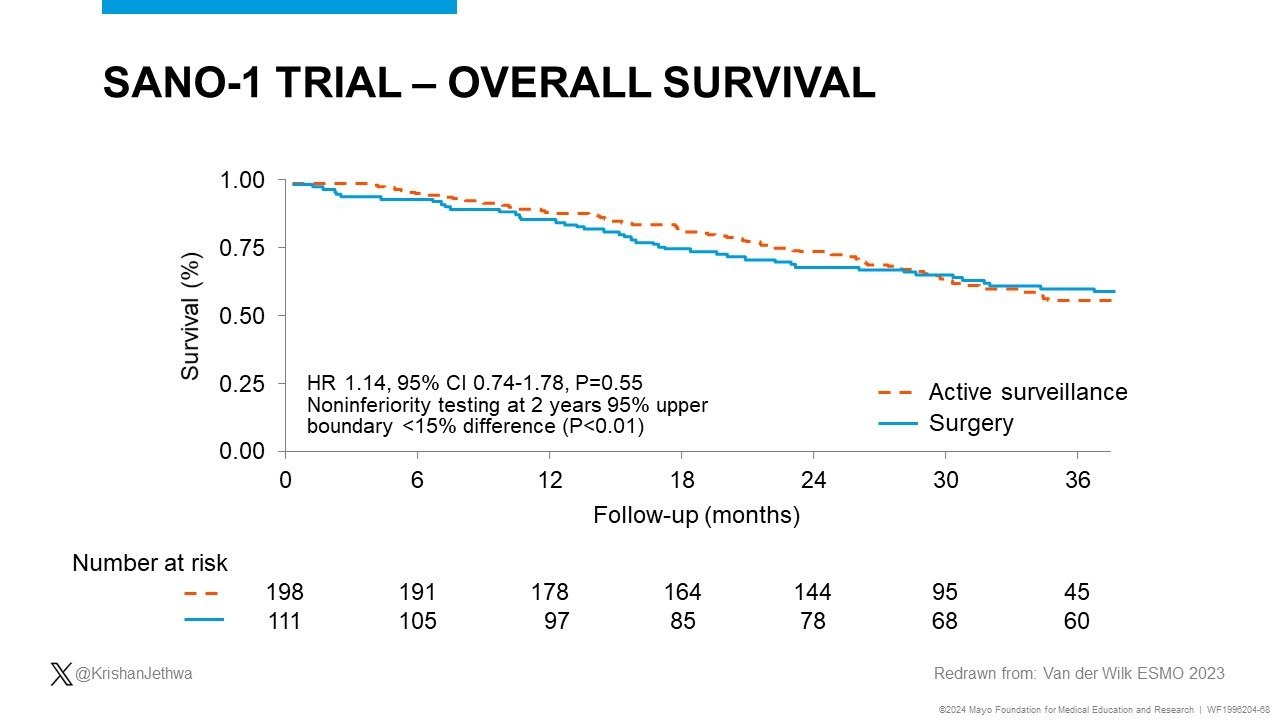
SANO.
Esophageal cancer with clinical complete response after CRT.
Active surveillance vs esophagectomy.
AS
- Non-inferior overall survival.
- Increased QoL.
SANO-2, ESOSTRATE, ESORES exploring.
Much unleashed potential with CRT + systemic treatment approach leads to organ preservation.”

Source: Krishan Jethwa/X
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-
Challenging the Status Quo in Colorectal Cancer 2024
December 6-8, 2024
-
ESMO 2024 Congress
September 13-17, 2024
-
ASCO Annual Meeting
May 30 - June 4, 2024
-
Yvonne Award 2024
May 31, 2024
-
OncoThon 2024, Online
Feb. 15, 2024
-
Global Summit on War & Cancer 2023, Online
Dec. 14-16, 2023