Predictors of Response to CDK4/6i Rechallenge in ER+ Metastatic Breast Cancer
Sergio Cifuentes Canaval, Medical Oncology Fellow at National Autonomous University of Mexico, shared a post on X:
“Check out my latest insights on Predictors of Response to CDK4/6i Rechallenge in ER+ Metastatic Breast Cancer: A Comprehensive Real-World Analysis
In this retrospective study, authors explored a recurrent question in clinical practice: What is the efficacy of CDK4/6 inhibitor rechallenge in patients with ER+ metastatic breast cancer who have previously undergone CDK4/6i therapy?
This analysis, encompassing 195 patients, provides key insights into both the clinical outcomes and molecular predictors associated with CDK4/6i retrial.
Study Overview:
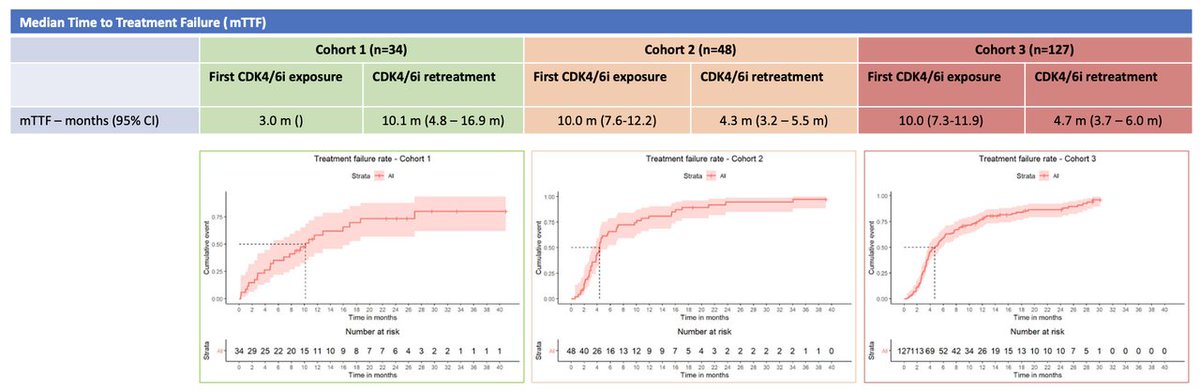
- Cohort 1 (n=34): Patients who discontinued initial CDK4/6i purely due to toxicity. This group experienced a median time to treatment failure (TTF) on rechallenge of 10.1 months, suggesting significant efficacy when prior discontinuation was due to adverse effects rather than progression. The leading toxicities causing discontinuation were neutropenia (32 percent), skin rash (17.5 percent), and joint pain (17 percent).
- Cohort 2 (n=48): Patients who progressed on first-line endocrine therapy (ET) + CDK4/6i and were rechallenged with the same CDK4/6i but a different ET agent. The median TTF for this cohort on retrial was 4.3 months, compared to 10.0 months during initial therapy.
- Cohort 3 (n=127): Patients who progressed on first-line ET + CDK4/6i and subsequently underwent a retrial with a different CDK4/6i. The median TTF on retrial was 4.7 months, compared to 10.0 months in initial treatment.
Molecular Insights: Detailed somatic mutation profiling was performed, particularly in Cohort 3. We analyzed patients who had a TTF2 on retrial less than 4 months (indicative of resistant disease) and those with a TTF2 more than 9 months (indicative of responsive disease):
- TP53 mutations: More frequent in the low TTF2 group (43 percent) compared to the high TTF2 group (21 percent).
- CDK4 amplifications: Observed in 4 percent of patients with TTF2 less than 4 months and absent in the more than 9 months group.
- RB1 loss-of-function mutations: Detected in 5 percent of patients with low TTF2, none in the high TTF2 cohort. Notably, these mutations emerged after initial CDK4/6i exposure, correlating with immediate progression upon retrial.
- FAT1 loss-of-function mutations: Found in 5 percent of patients in the low TTF2 cohort, with no occurrences in the high TTF2 group.
Key Considerations:
- Cohort 1 Findings: Patients who halted CDK4/6i due to toxicity had longer median TTF on rechallenge, supporting the practice of CDK4/6i reintroduction in those who tolerate the therapy but experienced initial adverse effects. However, there remains a significant risk of recurrence of similar toxicities.
- Molecular Profiling Insights: The marked presence of mutations such as TP53, RB1, and FAT1, as well as CDK4 amplifications in patients with poor TTF2, emphasizes the importance of genetic testing, particularly in those with rapid progression (<4 months) and extended responses (>9 months). Recognizing these patterns can aid in selecting candidates for rechallenge and tailoring individualized treatment plans.
- Future Directions: While prospective studies like PACE, PALMIRA, and MAINTAIN continue to explore these questions, real-world data enrich our understanding and support clinical practices that meet the nuanced needs of patients.
In-depth Discussion: This retrospective study, despite its limitations, addresses an often-posed question in clinical practice that remains unresolved by randomized trials. Changing CDK4/6i after progression on initial treatment is a common strategy, driven by both the trust in the first-line CDK4/6i approach and the limited efficacy or availability of subsequent options. This analysis offers reassurance regarding this practice and highlights the potential utility of molecular profiling for better decision-making. Also this study underscores that rechallenging with CDK4/6i post-toxicity discontinuation can be effective, with potential benefits also seen post-progression when guided by molecular assessment. Integrating genomic profiling into routine practice could optimize treatment sequencing and outcomes for patients with ER+ MBC.
Authors: Nicholas Mai, Carlos H. dos Anjos, Pedram Razavi, Anton Safonov, Sujata Patil, Yuan Chen, Joshua Z. Drago, Shanu Modi, Jacqueline F. Bromberg, Chau T. Dang, Dazhi Liu, Larry Norton, Mark Robson, Sarat Chandarlapaty, Komal Jhaveri. “

{kind=link}
-
Challenging the Status Quo in Colorectal Cancer 2024
December 6-8, 2024
-
ESMO 2024 Congress
September 13-17, 2024
-
ASCO Annual Meeting
May 30 - June 4, 2024
-
Yvonne Award 2024
May 31, 2024
-
OncoThon 2024, Online
Feb. 15, 2024
-
Global Summit on War & Cancer 2023, Online
Dec. 14-16, 2023