


Rishabh Jain, Medical Oncologist at AIIMS, shared on X:
“POLARGO may have changed the salvage conversation in transplant-ineligible R/R DLBCL. Not with a bispecific. Not with CAR-T. But by simply adding polatuzumab to R-GemOx.
Title: Polatuzumab Vedotin Plus Rituximab, Gemcitabine, and Oxaliplatin in Relapsed or Refractory Diffuse Large B-Cell Lymphoma: Results From the Phase III, Randomized POLARGO Trial
Authors: Matthew Matasar, Zhiming Li, Theodoros P. Vassilakopoulos, Juan-Manuel Sancho, Andreas Viardot, Andrew McMillan, Mehmet Sinan Dal, Juliana Pereira, Jin Seok Kim, Lugui Qiu, Connie Lee Batlevi, Rania Ibrahim, Juana Hernandez, Bruce McCall, Yanwen Jiang, Mark Yan, Will Harris, Lisa Musick, Corinne Haioun
Read the full article.

Patients with transplant-ineligible R/R DLBCL were randomized to: Pola-R-GemOx vs R-GemOx.
What changed?
OS improved
- 19.5 vs 12.5 months
- HR 0.60, p=0.0017
PFS improved
- 7.4 vs 2.7 months
- HR 0.37, p<0.0001
CR rate doubled
- 40.3% vs 19.0%
ORR doubled
- 52.7% vs 24.6%
Why this matters
This is not just a response-rate story. This is a true overall survival benefit in a setting where many patients are older, frail, or not candidates for transplant/CAR-T.
But toxicity is the catch
- Peripheral neuropathy: 57% vs 28.8%
- Grade 5 AEs: 11.7% vs 4.0%
- Excess fatal AEs were largely infection-related, including COVID.
My take
For transplant-ineligible R/R DLBCL, Pola-R-GemOx looks like a real new option, especially where access to CAR-T/bispecifics is limited.
The debate now is not whether it works. It’s where it fits against bispecifics, CAR-T, and pola-BR in 2026 practice. Would you use Pola-R-GemOx as your default salvage backbone in transplant-ineligible R/R DLBCL?”
Jeff Ryckman, Associate Professor of Radiation Oncology at WVU Medicine Camden Clark Medical Center, shared this post, adding:
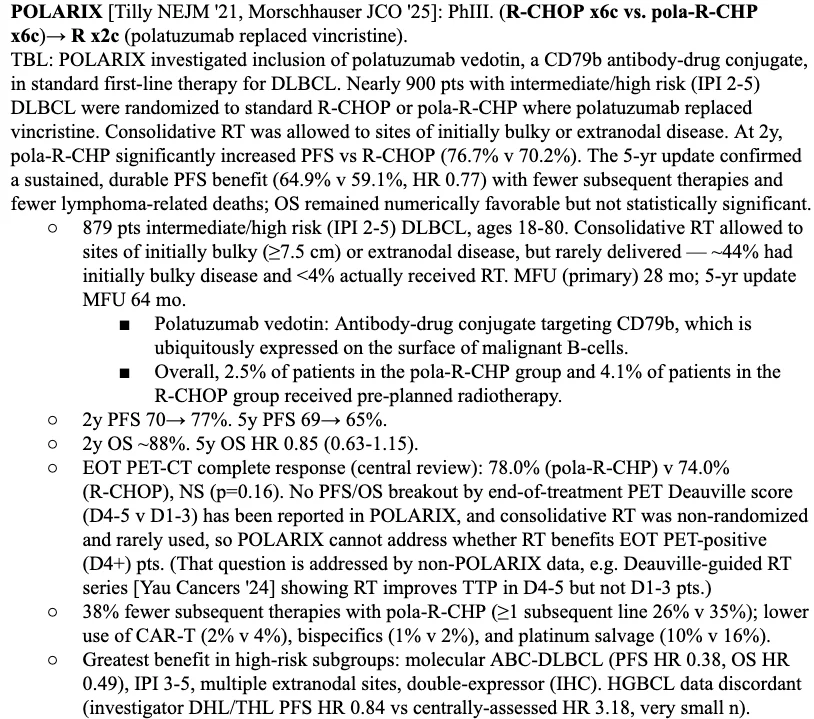
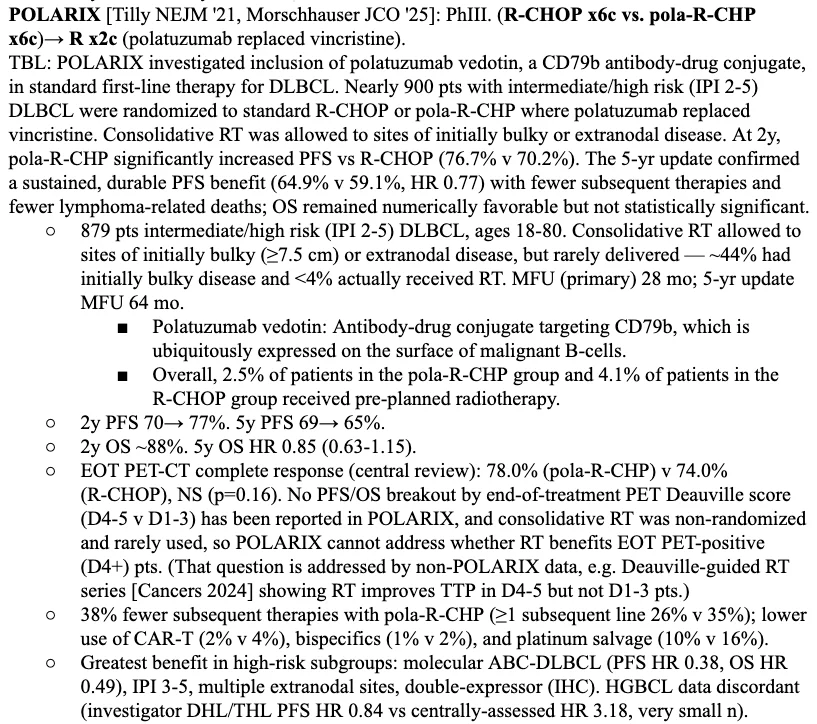
“As with POLARIX, the end-of-treatment PET non-CR subgroup went unreported in POLARGO. We still haven’t seen Deauville 4+ EOT outcomes for POLARIX, where ~22% were D4+, yet the low ~3% RT utilization rate was touted as a victory without PFS shown within the D4+ subgroup(!)
POLARGO does the same: no separate D4+ EOT reporting, even though ~60% were EOT PET D4+ – 3x the POLARIX rate(!). Only ~10% got radiotherapy on POLARGO, roughly a sixth of those who plausibly qualified. These patients likely would have benefited from salvage RT. RT shouldn’t have to be prespecified in trials like these (as it was on POLARIX) as one can’t reliably predict who’ll be D4+ at EOT. Similarly, POLARGO counted receipt of RT after planned systemic therapy as an EFS event, but not PFS event. Why not consider RT as part of the treatment package if EOT D4+?
RT shouldn’t have to be prespecified in trials like these (as it was on POLARIX) as one can’t reliably predict who’ll be D4+ at EOT. Similarly, POLARGO counted receipt of RT after planned systemic therapy as an EFS event, but not PFS event. Why not consider RT as part of the treatment package if EOT D4+?
Still, we need to see those outcomes in the D4+ EOT subgroup to help manage these patients in the real world. “Radiation-free survival” needs reframing in the era of modern RT techniques, especially against the known toxicity of salvage therapies.”
You can also read:
Diffuse Large B-Cell Lymphoma (DLBCL): Molecular Heterogeneity and Progress in Therapy

{kind=link}
{kind=link}