


Stereotactic body radiotherapy has changed the treatment landscape for medically inoperable early-stage non-small cell lung cancer.
For many patients, SBRT offers high local control with a short, highly focused radiation course. But not all tumors behave the same way. Some remain controlled for years. Others recur locally despite treatment that appears technically adequate.
A new study published in Clinical Lung Cancer suggests that pretreatment tumor metabolism may help explain part of that difference.
The study found that maximum standardized uptake value, or SUVmax, on pretreatment FDG-PET/CT was a strong prognostic marker in patients with stage I NSCLC treated with SBRT.
More importantly, SUVmax appeared to identify which patients were most affected by treatment schedule.
Patients with high-metabolic tumors, defined as SUVmax ≥5.0, had better local control when SBRT was delivered consecutively over 4–5 days, compared with non-consecutive treatment over 6–10 days.
For low-metabolic tumors, treatment gaps did not appear to significantly affect local control.
The findings support a more biologically guided approach to lung SBRT scheduling.
Why Tumor Metabolism Matters in Lung SBRT
FDG-PET/CT is already widely used in lung cancer staging and radiation planning.
SUVmax provides a semi-quantitative measure of glucose uptake. Higher uptake often reflects more aggressive tumor biology, including rapid proliferation, hypoxia, and radioresistant features.
In early-stage NSCLC, several studies have linked higher pretreatment SUVmax with worse local control and survival after SBRT.
The new analysis adds another layer: tumor metabolism may not only predict outcomes, but also help determine how sensitive a tumor is to treatment prolongation.
This is clinically relevant because SBRT schedules can vary in real-world practice. A 4-fraction course may be delivered on consecutive days, or it may be interrupted by weekends, holidays, machine availability, or departmental logistics.
The question is whether those short gaps matter.
According to this study, they may matter most for metabolically aggressive tumors.

Study Design
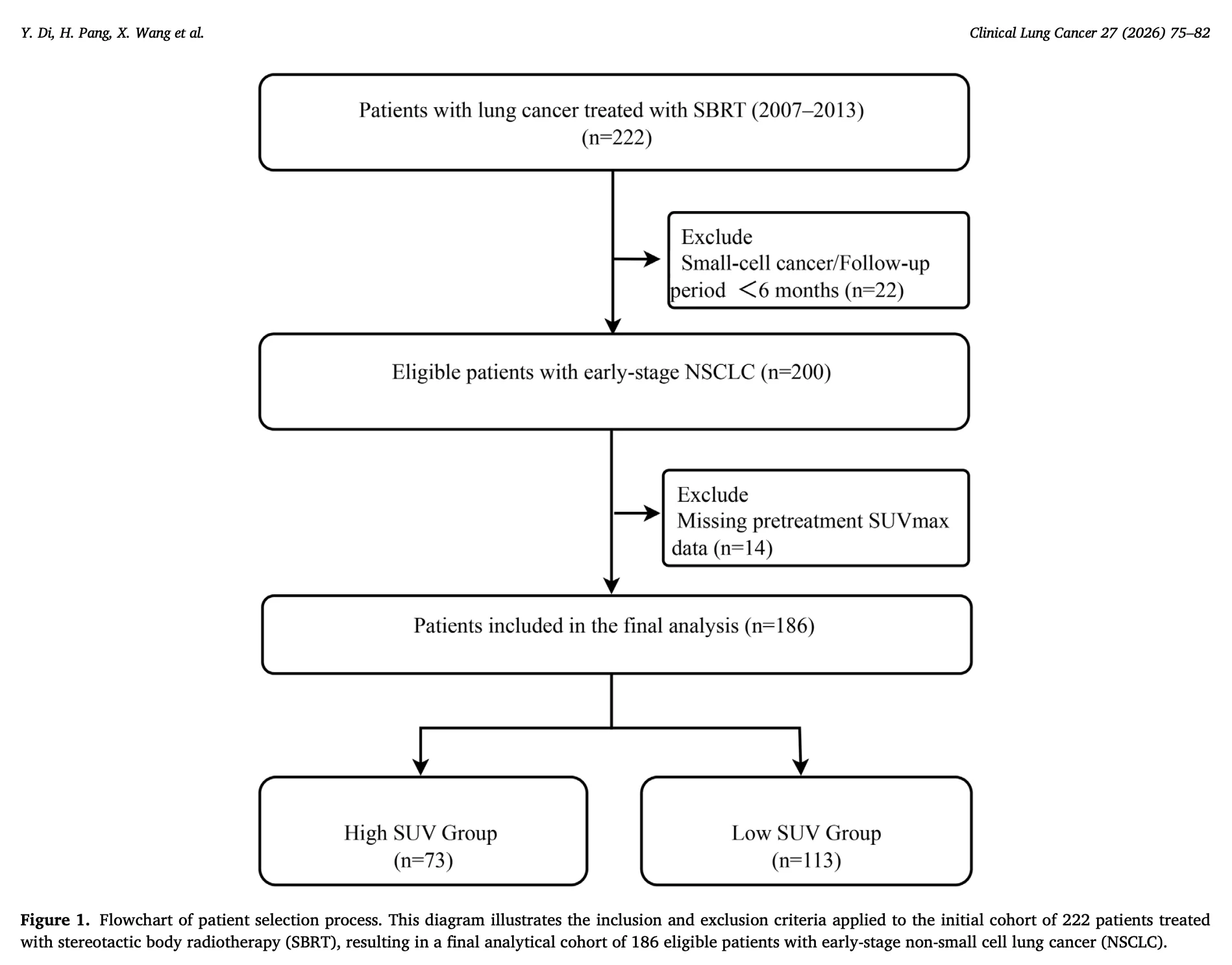
The investigators retrospectively analyzed 186 patients with stage I NSCLC treated with SBRT between 2007 and 2013.
All patients received a uniform SBRT regimen of 48 Gy in 4 fractions.
Patients were stratified by pretreatment FDG-PET/CT SUVmax:
- High SUVmax: SUVmax ≥5.0, 73 patients
- Low SUVmax: SUVmax <5.0, 113 patients
Treatment schedule was categorized as:
- Consecutive SBRT: completed within 4–5 days
- Non-consecutive SBRT: completed over 6–10 days
The main endpoints were local control and overall survival.
The study also evaluated whether SUVmax modified the relationship between treatment schedule and clinical outcomes.
High SUVmax Predicted Worse Local Control and Survival
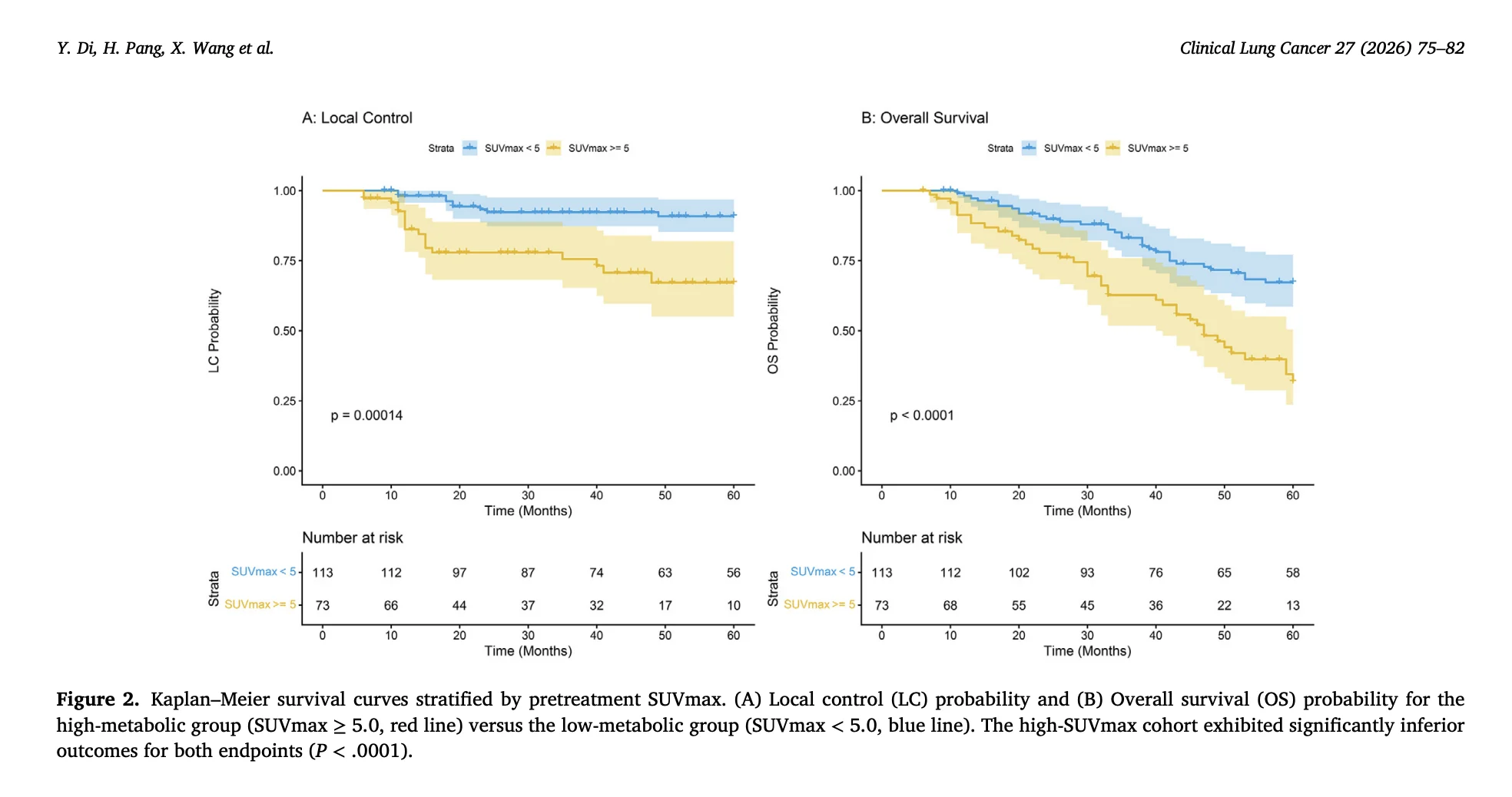
At a median follow-up of 41 months, pretreatment SUVmax strongly stratified outcomes.
The 3-year local control rate was:
- 92.1% in the low SUVmax group
- 63.4% in the high SUVmax group
This difference was statistically significant.
On multivariable analysis, SUVmax ≥5.0 independently predicted local failure, with a hazard ratio of 3.70.
High SUVmax also independently predicted worse overall survival, with a hazard ratio of 2.38.
These findings reinforce the role of tumor metabolism as a clinically meaningful risk marker in early-stage NSCLC treated with SBRT.
Anatomical staging alone may not fully capture tumor behavior.
Two tumors of similar size and stage may have very different biological risk if their metabolic activity differs substantially.
Consecutive SBRT Helped the High-SUVmax Group
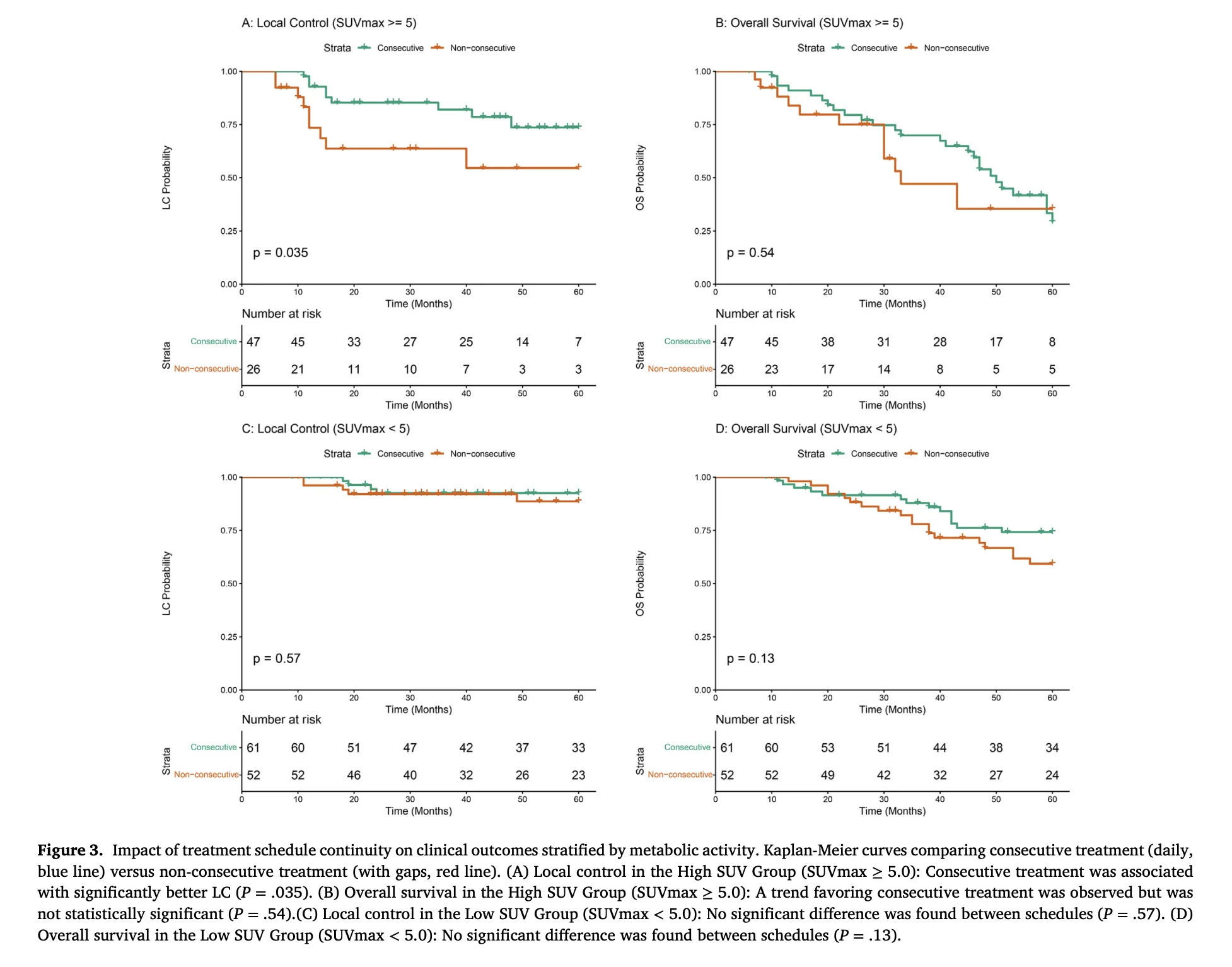
The most important finding was the interaction between SUVmax and treatment schedule.
In the high SUVmax group, consecutive daily SBRT was associated with significantly better local control compared with non-consecutive SBRT.
The difference was statistically significant, with P=0.035.
By contrast, in the low SUVmax group, there was no significant difference in local control between consecutive and non-consecutive schedules.
This suggests that metabolically active tumors may be more vulnerable to treatment gaps.
The authors also reported a significant interaction between SUVmax and treatment schedule, with a P-interaction of 0.042.
That interaction is important because it suggests the effect of scheduling is not uniform across all patients.
The same treatment gap may be clinically meaningful in one tumor biology and less important in another.
A Possible Radiobiological Explanation
The authors propose that high-SUVmax tumors may have more aggressive growth kinetics and greater potential for accelerated repopulation during treatment gaps.
In radiotherapy, overall treatment time can matter because surviving clonogenic tumor cells may begin to repopulate during interruptions.
For conventional radiotherapy, this concept is well established in several tumor types.
For SBRT, the effect has been less clear because treatment courses are short and doses per fraction are high.
This study suggests that even within a short SBRT course, timing may still matter for selected high-risk tumors.
The authors also note that the prescribed regimen, 48 Gy in 4 fractions, was at the lower end of standard ablative SBRT dosing. This may have made treatment timing more important, especially for high-metabolic tumors near the threshold of adequate biological dose.

Low-SUVmax Tumors May Tolerate Short Gaps
In the low SUVmax group, non-consecutive treatment did not significantly worsen local control or overall survival.
This finding is also clinically useful.
Not every patient may need the most compressed schedule. For more indolent tumors, modest treatment spacing may be acceptable, particularly when anatomy or safety concerns make consecutive delivery less desirable.
This is especially relevant for central or ultra-central lung tumors, larger targets, prior radiotherapy, or cases where normal tissue constraints require caution.
The authors emphasize that biological prioritization must be balanced against safety.
Consecutive treatment may be beneficial for high-metabolic peripheral tumors when technically safe, but protracted schedules remain necessary when compressed dosing could raise the risk of toxicity.
Safety Still Comes First
The study does not argue that all lung SBRT should be delivered consecutively.
That would be too simple.
For some patients, especially those with central or ultra-central tumors, prior overlapping radiation fields, large target volumes, or challenging organ-at-risk constraints, non-consecutive or more protracted schedules may be mandatory.
The key message is not “daily SBRT for everyone.”
The message is that pretreatment SUVmax could help identify patients in whom avoiding unnecessary treatment gaps may be particularly important.
In resource-constrained departments, this could help prioritize scheduling.
High-SUVmax tumors may deserve greater urgency for uninterrupted treatment when safe.
Low-SUVmax tumors may allow more scheduling flexibility.
Limitations
The study has important limitations.
It was retrospective and conducted at a single institution.
The treatment period was 2007 to 2013, and SBRT technology, imaging, planning, and risk-adapted fractionation have continued to evolve.
The number of local failure events was limited, especially in the low SUVmax subgroup.
The analysis is hypothesis-generating and requires prospective validation before changing practice.
Also, SUVmax can be affected by PET acquisition parameters, scanner calibration, blood glucose levels, tumor size, respiratory motion, and image reconstruction methods.
A single universal cutoff may not apply across all institutions.
Still, the signal is clinically compelling because it connects a widely available imaging biomarker with a practical treatment-delivery decision.
What This Could Mean for Practice
This study supports a more personalized approach to SBRT timing in early-stage NSCLC.
For patients with high pretreatment SUVmax, clinicians may consider minimizing avoidable treatment gaps when anatomy and safety allow.
For patients with low SUVmax, modestly non-consecutive treatment may remain reasonable, particularly when needed for safety or logistics.
The findings also support the broader role of FDG-PET/CT beyond staging.
Pretreatment PET may help guide not only whether SBRT is appropriate, but also how urgently and continuously it should be delivered.
In modern lung cancer care, biology should increasingly inform radiation scheduling.

The Bottom Line
In this Clinical Lung Cancer study, pretreatment SUVmax was a strong prognostic biomarker in stage I NSCLC treated with SBRT.
Patients with SUVmax ≥5.0 had worse local control and overall survival.
They also appeared to benefit more from consecutive daily SBRT.
For high-metabolic tumors, consecutive treatment was associated with improved local control. For low-metabolic tumors, treatment gaps over a short SBRT course did not significantly affect outcomes.
The results suggest a practical concept: early-stage NSCLC SBRT scheduling may be optimized by tumor biology.
High-risk metabolic tumors may need fewer gaps.
Indolent tumors may allow more flexibility.
Safety, however, remains the final boundary.
References
- Di Y, Pang H, Wang X, Meng L. Pretreatment SUVmax stratifies the benefit of consecutive daily SBRT in early-stage non-small cell lung cancer. Clinical Lung Cancer. 2026;27:75–82. doi:10.1016/j.cllc.2026.06.002.
- Ikawa T, Tabuchi T, Konishi K, et al. Prolonged overall treatment time negatively affects the outcomes of stereotactic body radiotherapy for early-stage non-small-cell lung cancer: a propensity score-weighted, single-center analysis. PLOS One. 2021;16(6).
- Dong M, Liu J, Sun X, Xing L. Prognostic significance of SUVmax on pretreatment 18F-FDG PET/CT in early-stage non-small cell lung cancer treated with stereotactic body radiotherapy: a meta-analysis. Journal of Medical Imaging and Radiation Oncology. 2017;61(5):652–659.
- Takeda A, Sanuki N, Fujii H, et al. The maximum standardized uptake value on FDG-PET is a strong predictor of local recurrence for localized non-small-cell lung cancer after stereotactic body radiotherapy. Radiotherapy and Oncology. 2011;101(2):291–297.
- Horne ZD, Clump DA, Vargo JA, et al. Pretreatment SUVmax predicts progression-free survival in early-stage non-small cell lung cancer treated with stereotactic body radiation therapy. Radiation Oncology. 2014;9:41.
{kind=link}
{kind=link}
{kind=link}