


At the ASCO Annual Meeting, Atsuo Takashima, MD, PhD, presented Abstract LBA3508, the primary analysis of EPISODE-III: JCOG1503C, a randomized, double-blind, placebo-controlled phase 3 trial evaluating adjuvant low-dose aspirin in stage III colorectal cancer after curative resection.
The study examined whether adding low-dose aspirin to standard adjuvant chemotherapy could improve disease-free survival in an unselected population of patients with stage III colorectal cancer.
Background
Observational studies have suggested that postdiagnosis aspirin use may improve outcomes in colorectal cancer. However, adjuvant evidence remains limited. In unselected populations, phase 3 trials have not shown a clear benefit, while biomarker-selected studies have suggested a possible benefit in PI3K-altered tumors. EPISODE-III evaluated whether low-dose aspirin could improve disease-free survival in patients with unselected stage III colorectal cancer receiving standard adjuvant chemotherapy.
Study Design
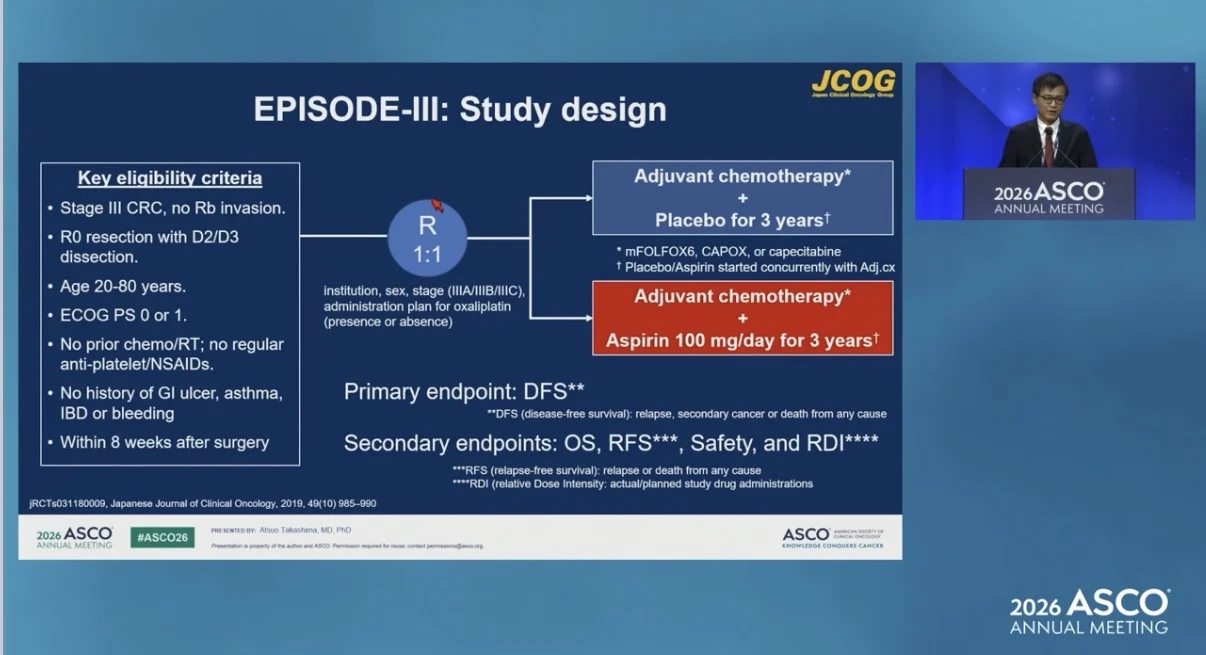
EPISODE-III was a multi-institutional, two-arm, randomized, double-blind, placebo-controlled phase 3 trial conducted at 36 institutions in Japan.
Eligible patients were 20 to 80 years old, had ECOG performance status 0–1, and had histologically confirmed R0-resected stage III adenocarcinoma from the cecum to the upper rectum. Patients with lower rectal cancer were excluded.
Additional eligibility criteria included no prior chemotherapy or radiotherapy, no regular antiplatelet or NSAID use, no history of gastrointestinal ulcer, asthma, inflammatory bowel disease, or bleeding, and enrollment within 8 weeks after surgery. Aspirin or placebo was started concurrently with adjuvant chemotherapy.
All patients had undergone D2/D3 lymph node dissection and received standard adjuvant chemotherapy with capecitabine, mFOLFOX6, or CAPOX.
Patients were randomized 1:1 to receive low-dose aspirin 100 mg once daily or matched placebo for 3 years, in addition to standard adjuvant chemotherapy. Randomization was balanced by institution, sex, stage, and planned oxaliplatin use.
The primary endpoint was disease-free survival, defined as relapse, second cancer, or death. Secondary endpoints included overall survival, relapse-free survival, relative dose intensity of aspirin and placebo, and safety. The planned sample size was 880 patients, with 279 disease-free survival events, providing 80% power with a one-sided alpha of 0.05 to detect a hazard ratio of 0.741.

Results
Between March 2018 and October 2022, 882 patients were enrolled. Of these, 442 were assigned to placebo and 440 to aspirin.
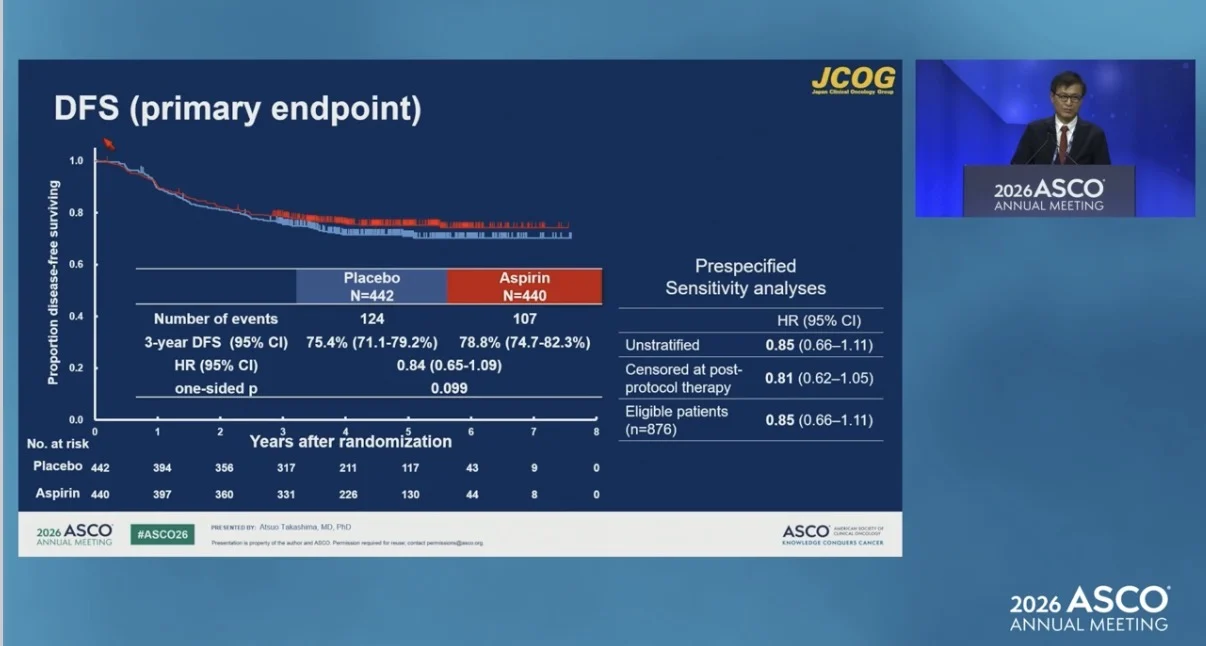
At the October 2025 data cutoff, the median follow-up for all randomized patients was 4.0 years. A total of 231 disease-free survival events had occurred, including 124 in the placebo arm and 107 in the aspirin arm.

Baseline characteristics were balanced between the two arms. Median age was 65 years in the placebo arm and 64 years in the aspirin arm. Stage distribution was IIIA/IIIB/IIIC in 19%/63%/18% of patients in the placebo arm and 19%/62%/19% in the aspirin arm. Planned oxaliplatin-containing treatment was used in 70% and 71% of patients, respectively.
Three-year disease-free survival was 75.4% with placebo and 78.8% with aspirin, showing a numerical difference of 3.4% in favor of aspirin. However, the primary endpoint was not met. The hazard ratio for disease-free survival was 0.84, with a 95% confidence interval of 0.65–1.09 and a one-sided p-value of 0.0987.
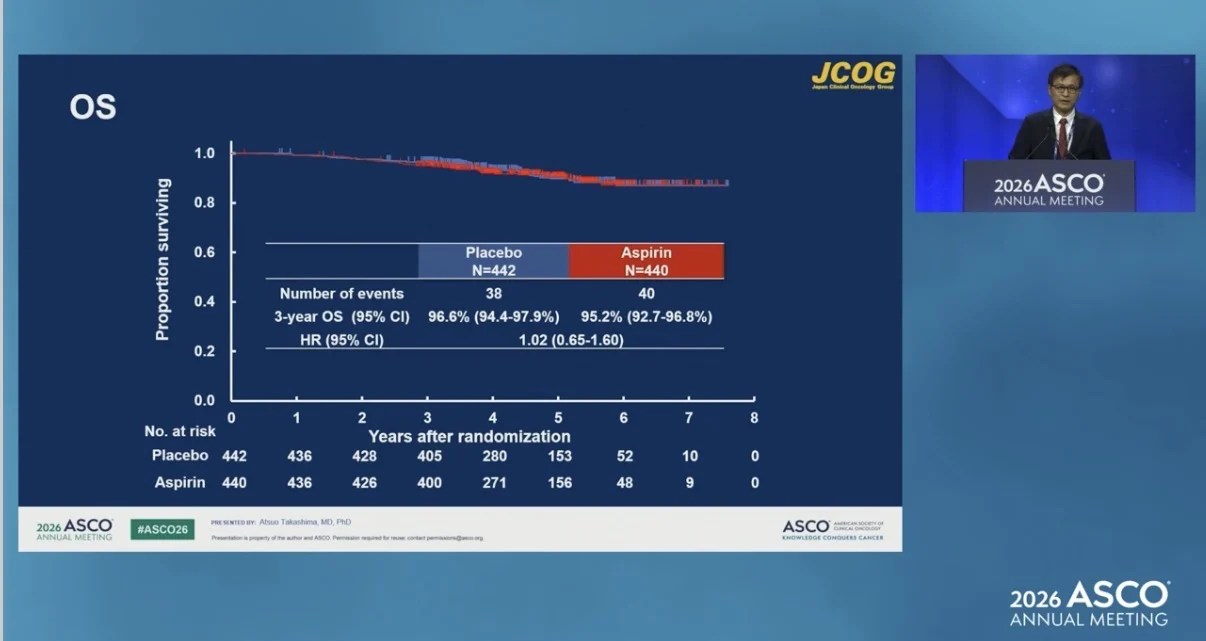
Three-year relapse-free survival was 77.2% with placebo and 79.5% with aspirin. The hazard ratio was 0.87, with a 95% confidence interval of 0.66–1.14. Three-year overall survival was 96.6% with placebo and 95.2% with aspirin. The hazard ratio was 1.02, with a 95% confidence interval of 0.65–1.60.

Safety
Grade 3 or higher adverse events were similar between the placebo and aspirin arms. Grade 3 or higher aspirin-related adverse events occurred in fewer than 1% of patients, including lower gastrointestinal bleeding in 4 patients. One treatment-related death occurred in the aspirin arm during chemotherapy and was due to ischemic heart disease. Relative dose intensity was high and comparable between arms, with a median of 98.6% in both groups.
Conclusion
In EPISODE-III, low-dose aspirin added to standard adjuvant chemotherapy did not significantly improve disease-free survival in patients with unselected stage III colorectal cancer after curative resection. A numerical disease-free survival improvement was observed with aspirin, and aspirin was well tolerated.

Exploratory biomarker analyses, including PI3K/PIK3CA, are ongoing and will inform a planned collaborative meta-analysis of randomized trials. Overall survival data were immature, with final OS analysis planned in 2028.
The full abstract is available on the official ASCO website.
{kind=link}
{kind=link}
{kind=link}
{kind=link}