


At the 2026 ASCO Annual Meeting, Ghassan K. Abou-Alfa, MD, presented results from EMERALD-3, a phase 3 randomized study evaluating tremelimumab plus durvalumab, with or without lenvatinib, combined with transarterial chemoembolization in patients with unresectable embolization-eligible hepatocellular carcinoma.
The study was presented as Abstract LBA4000.
Background
Transarterial chemoembolization is a global standard of care for patients with unresectable embolization-eligible hepatocellular carcinoma. Beyond its local antitumor effect, TACE can also induce a tumor immune response, providing a rationale for combining it with immunotherapy and anti-angiogenic therapy.
STRIDE, which consists of a single dose of tremelimumab followed by regular-interval durvalumab, is a frontline standard of care in advanced hepatocellular carcinoma and has shown sustained overall survival benefit through 6 years of follow-up versus sorafenib.
EMERALD-3 was designed to evaluate whether adding STRIDE, with or without lenvatinib, to TACE could improve outcomes in patients with unresectable embolization-eligible hepatocellular carcinoma.
Study Design
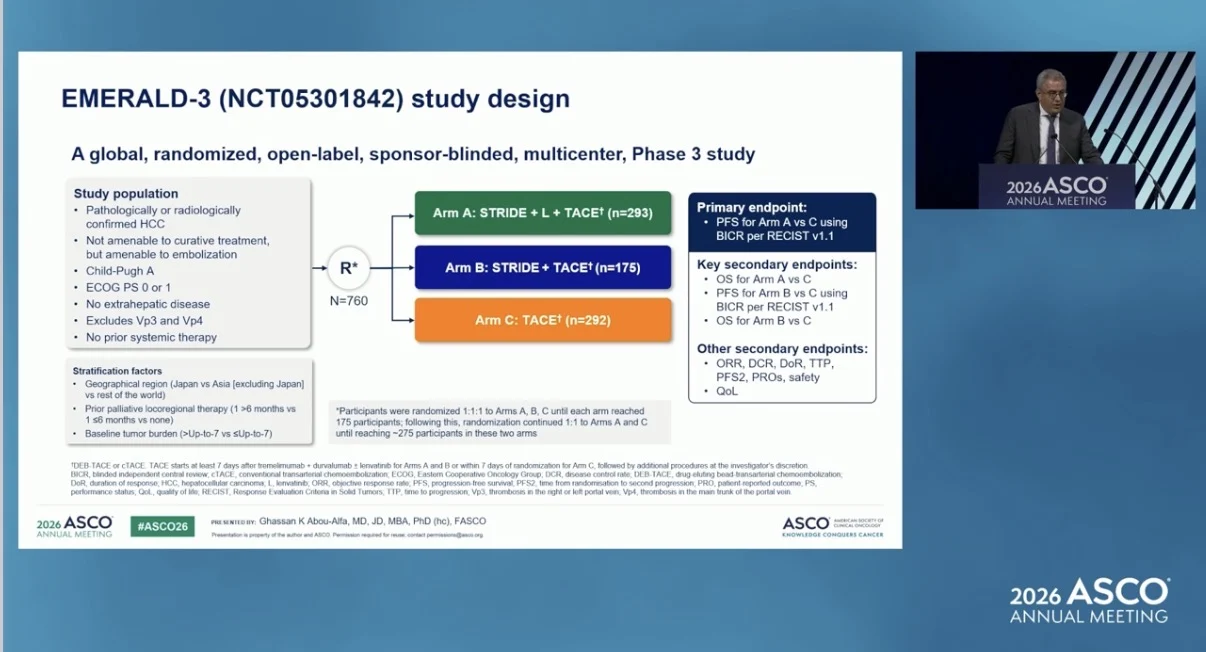
EMERALD-3 was a global, randomized, open-label, sponsor-blinded, multicenter phase 3 study.
The study enrolled patients with pathologically or radiologically confirmed hepatocellular carcinoma who were not amenable to curative treatment but were suitable for embolization. Eligible patients had Child-Pugh A liver function, ECOG performance status 0 or 1, no extrahepatic disease, no prior systemic therapy, and no Vp3 or Vp4 portal vein invasion. Patients were randomized to receive STRIDE plus lenvatinib plus TACE, STRIDE plus TACE, or TACE alone.
In the STRIDE-based arms, patients received tremelimumab 300 mg on day 1 and durvalumab 1500 mg on day 1, followed by durvalumab 1500 mg every 4 weeks. Lenvatinib was started on day 1 and continued daily.
TACE was started at least 7 days after tremelimumab, durvalumab, and lenvatinib in the STRIDE-based arms, or within 7 days of randomization in the TACE arm. Subsequent TACE procedures were administered at the investigator’s discretion.
Participants were randomized 1:1:1 until each arm reached 175 participants. After that, randomization continued 1:1 to STRIDE plus lenvatinib plus TACE and TACE until at least 275 participants were reached in those two arms.
The primary endpoint was progression-free survival for STRIDE plus lenvatinib plus TACE versus TACE by blinded independent central review using RECIST v1.1. Key secondary endpoints included overall survival for STRIDE plus lenvatinib plus TACE versus TACE, progression-free survival for STRIDE plus TACE versus TACE, and overall survival for STRIDE plus TACE versus TACE.

Results
As of February 23, 2026, 293 patients had been randomized to STRIDE plus lenvatinib plus TACE, 175 to STRIDE plus TACE, and 292 to TACE. Baseline characteristics were broadly balanced across the treatment arms.
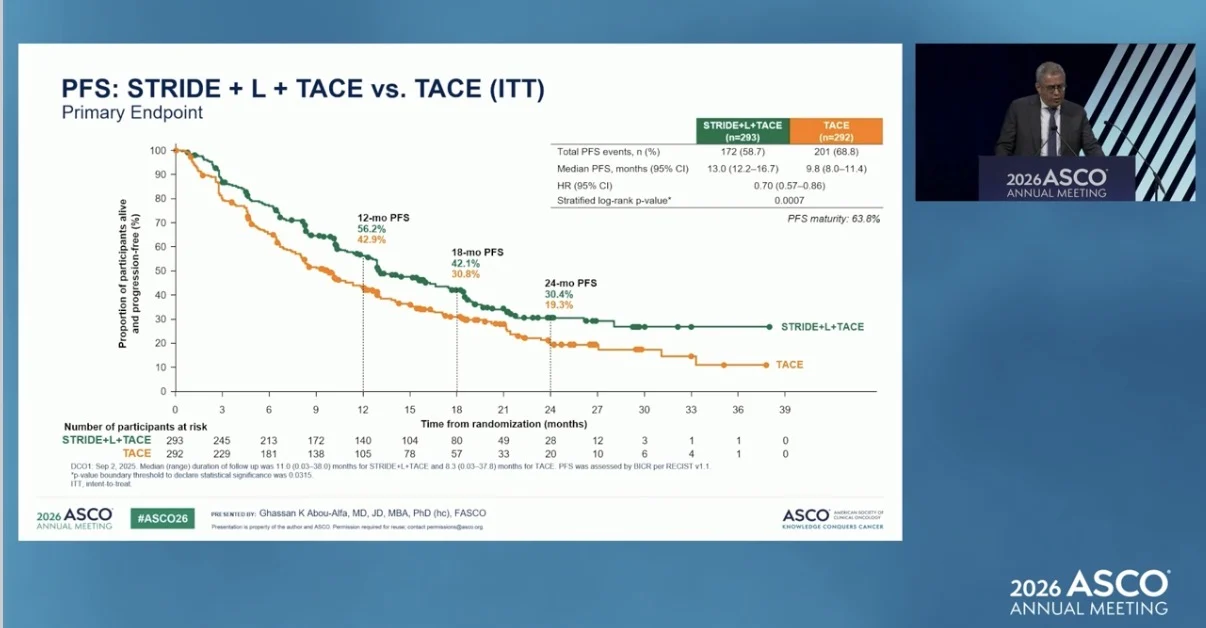
STRIDE plus lenvatinib plus TACE significantly improved progression-free survival compared with TACE. Median progression-free survival was 13.0 months with STRIDE plus lenvatinib plus TACE and 9.8 months with TACE, with a hazard ratio of 0.70.

At the interim overall survival analysis, with 40% maturity, STRIDE plus lenvatinib plus TACE showed a positive overall survival trend compared with TACE. Median overall survival was 39.5 months with STRIDE plus lenvatinib plus TACE and 34.7 months with TACE, with a hazard ratio of 0.84. The 24-month overall survival rate was 66.9% and 61.5%, respectively.
The STRIDE plus TACE arm also showed improved outcomes compared with TACE. Median progression-free survival was 12.9 months with STRIDE plus TACE and 8.1 months with TACE, with a hazard ratio of 0.71.
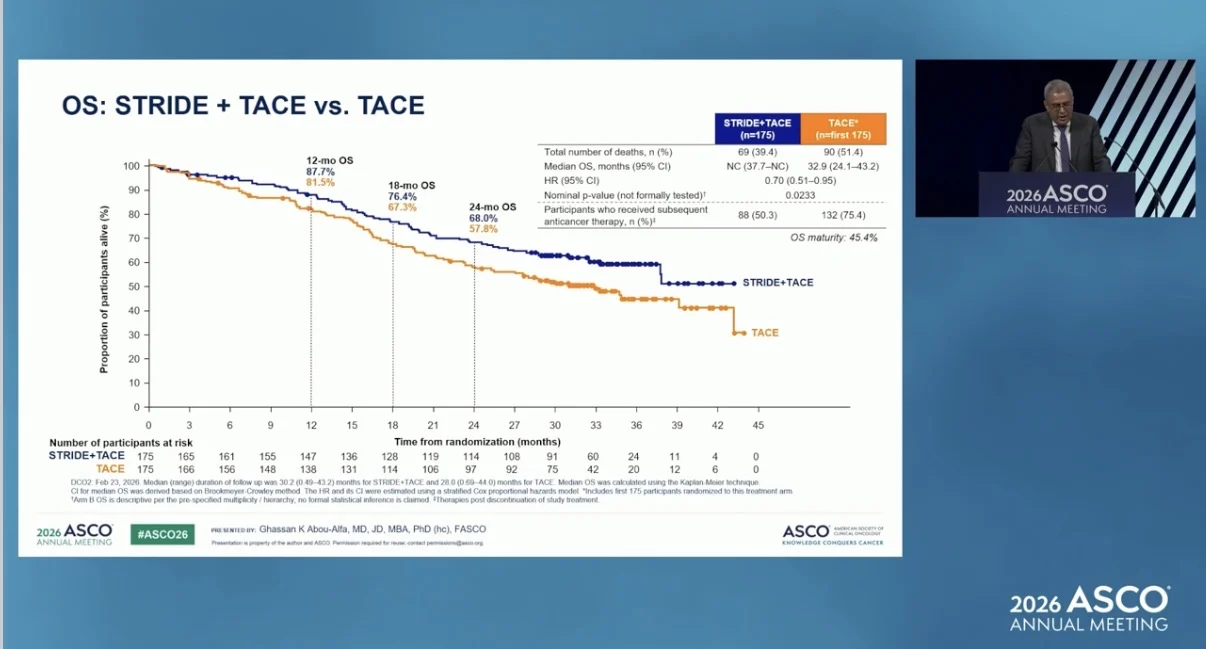
Overall survival also favored STRIDE plus TACE compared with TACE. Median overall survival was not calculable with STRIDE plus TACE and was 32.9 months with TACE, with a hazard ratio of 0.70. The 24-month overall survival rate was 68.0% with STRIDE plus TACE and 57.8% with TACE.

Safety
Treatment-related adverse events of maximum grade 3 or 4 occurred in 62.7% of patients receiving STRIDE plus lenvatinib plus TACE, 48.6% of those receiving STRIDE plus TACE, and 18.6% of those receiving TACE. The safety profile was acceptable and consistent with the known safety profiles of STRIDE, lenvatinib, and TACE.
Conclusion
EMERALD-3 showed that STRIDE plus lenvatinib plus TACE significantly improved progression-free survival compared with TACE alone in patients with unresectable embolization-eligible hepatocellular carcinoma.

At interim analysis, STRIDE plus lenvatinib plus TACE showed a favorable overall survival trend compared with TACE. STRIDE plus TACE also showed clinically meaningful improvements in progression-free survival and overall survival compared with TACE, although formal statistical testing has not yet been done.
EMERALD-3 is the first phase 3 study to demonstrate that a STRIDE-based regimen improves clinical outcomes when combined with TACE, supporting its role as a potential new treatment option in unresectable embolization-eligible hepatocellular carcinoma.
The full abstract is available on the official ASCO website.

Read more about EMERALD-3 Trial on OncoDaily.
{kind=link}
{kind=link}
{kind=link}
{kind=link}