


At the 2026 ASCO Annual Meeting, Gunnar Folprecht, MD, from Dresden, Germany, presented results from CIRCULATE, an AIO KRK-0217/ABCSG phase 3 trial evaluating whether postoperative circulating tumor DNA testing could guide adjuvant treatment decisions in patients with stage II colon cancer. The study was presented as Abstract LBA3500.
The trial focused on patients with UICC stage II, pMMR/MSS colon cancer. The analysis examined disease-free survival and time to recurrence using a ctDNA-based strategy for adjuvant chemotherapy decision-making.
Background
Adjuvant chemotherapy provides limited benefit in unselected patients with stage II colon cancer. Postoperative ctDNA has higher prognostic value than classical clinical or molecular markers, but its ability to predict benefit from adjuvant chemotherapy had not been proven.
Study Design
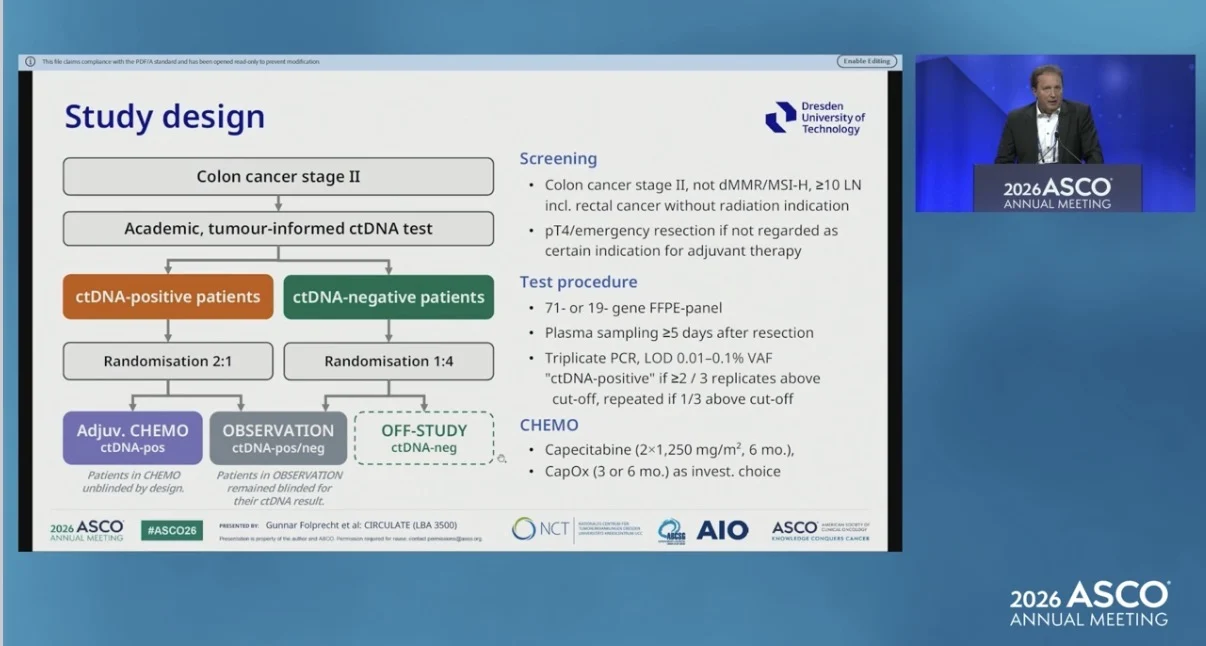
Patients with UICC stage II, pMMR/MSS colon cancer were tested for ctDNA using an academic, tumor-informed, next-generation sequencing-based test. Patients who were ctDNA positive were randomized, with a planned 2:1 ratio, to receive chemotherapy or observation without adjuvant chemotherapy. Chemotherapy consisted of 6 months of capecitabine or 3 to 6 months of capecitabine plus oxaliplatin.

Patients who were ctDNA negative were randomized 1:4 to observation or off-study. Patients in the observation arm and their investigators remained blinded to ctDNA status. The primary endpoint was disease-free survival in ctDNA-positive patients comparing chemotherapy with observation. Time to recurrence was reported as the 3-year recurrence rate. The planned sample size was 1,540 randomized patients, assuming a ctDNA-positive rate of 10%. Because the funding period expired, the trial ended early and was finally analyzed.
Patient Population
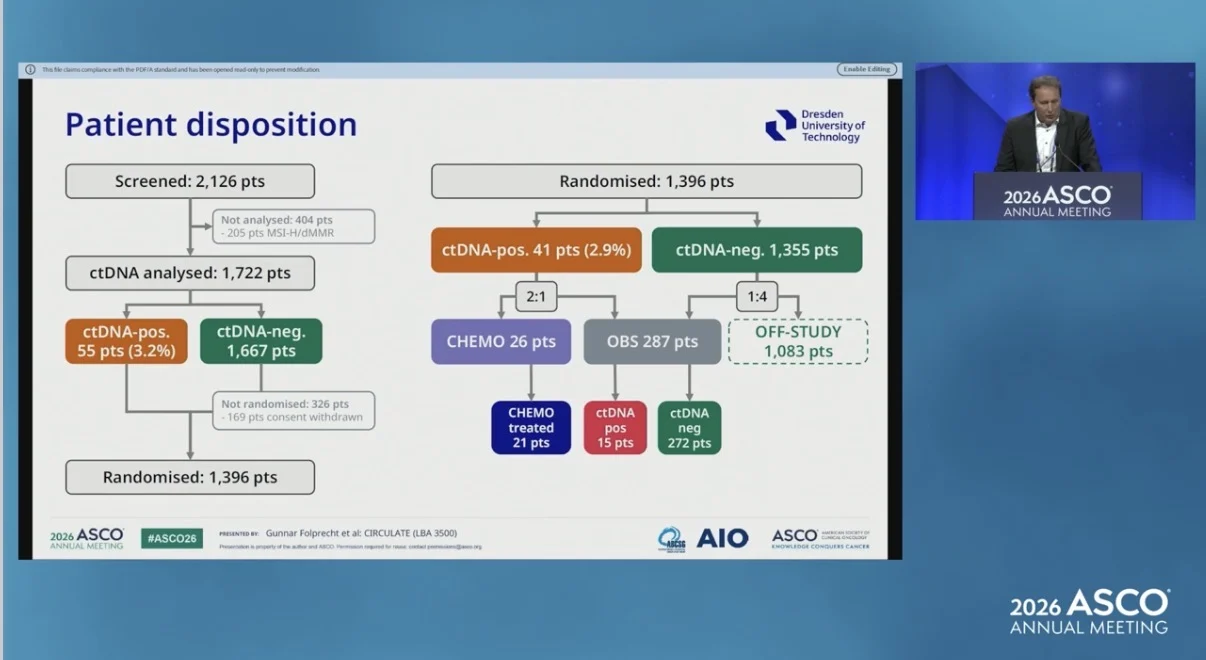
From June 2020 to July 2025, 2,126 patients were screened at 138 sites in Germany and Austria. Overall, 1,396 patients were randomized. Among randomized patients, 41 were ctDNA-positive, representing 2.9% of the randomized population, and 1,355 were ctDNA-negative.
Of these patients, 1,083 were assigned to off-study follow-up, 287 to observation, and 26 to chemotherapy. In the observation arm, 15 patients were ctDNA-positive and 272 were ctDNA-negative. The median age was 64 years, and 63% of patients were male. Classical risk factors were present in 9.5% of patients, including 4.8% with pT4 disease and 5.0% with emergency or unplanned resection.

Treatment Delivery
Among the 26 patients randomized to chemotherapy, 21 started treatment. Of those treated, 33% received oxaliplatin and 67% received capecitabine monotherapy. The median number of chemotherapy cycles was 6.
Key Results
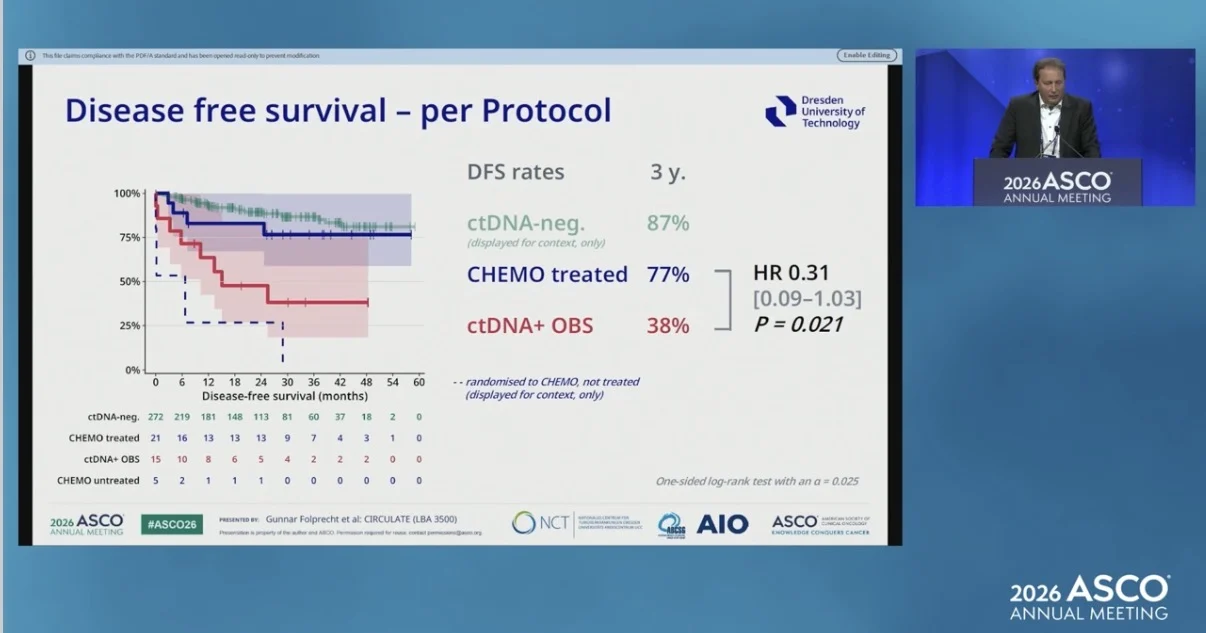
ctDNA status was highly prognostic in stage II colon cancer. In the observation arm, the 3-year disease-free survival rate was 87% in ctDNA-negative patients compared with 38% in ctDNA-positive patients. The 3-year overall survival rate was 98% in ctDNA-negative patients and 84% in ctDNA-positive patients.
Per-Protocol Analysis
In the per-protocol analysis, which excluded patients assigned to chemotherapy who did not start treatment, chemotherapy was associated with improved outcomes compared with observation in ctDNA-positive patients.
The 3-year recurrence rate was 19% with chemotherapy compared with 62% with observation. The hazard ratio for time to recurrence was 0.23, with a 95% confidence interval of 0.06 to 0.87 and p = 0.009. The 3-year disease-free survival rate was 77% with chemotherapy compared with 38% with observation. The hazard ratio for disease-free survival was 0.31, with a 95% confidence interval of 0.09 to 1.03 and p = 0.021.

Intention-to-Treat Analysis
In the intention-to-treat analysis, which included all patients randomized to chemotherapy, including those who did not start treatment, the primary endpoint was formally negative.
The 3-year recurrence rate was 35% with chemotherapy compared with 62% with observation. The hazard ratio was 0.48, with a 95% confidence interval of 0.17 to 1.33 and p = 0.075. The 3-year disease-free survival rate was 61% with chemotherapy compared with 38% with observation. The hazard ratio was 0.55, with a 95% confidence interval of 0.21 to 1.48 and p = 0.12. Among treated patients, 95% had any toxicity and 48% had grade 3 or higher toxicity. One treatment-related death was reported.
Limitations
The trial had a lower-than-expected ctDNA-positive rate of 2.9% among randomized patients. The several limitations, including that the ctDNA assay was designed 10 years ago with priority placed on high specificity, the panel was limited, testing was performed at a single postoperative time point, and the study population was relatively low risk.
Some patients randomized to chemotherapy did not start treatment, including because of metastases found on workup imaging triggered by unblinding or because of consent withdrawal. The trial also closed early because of funding expiry, resulting in wide confidence intervals and limited statistical power.
Takeaway
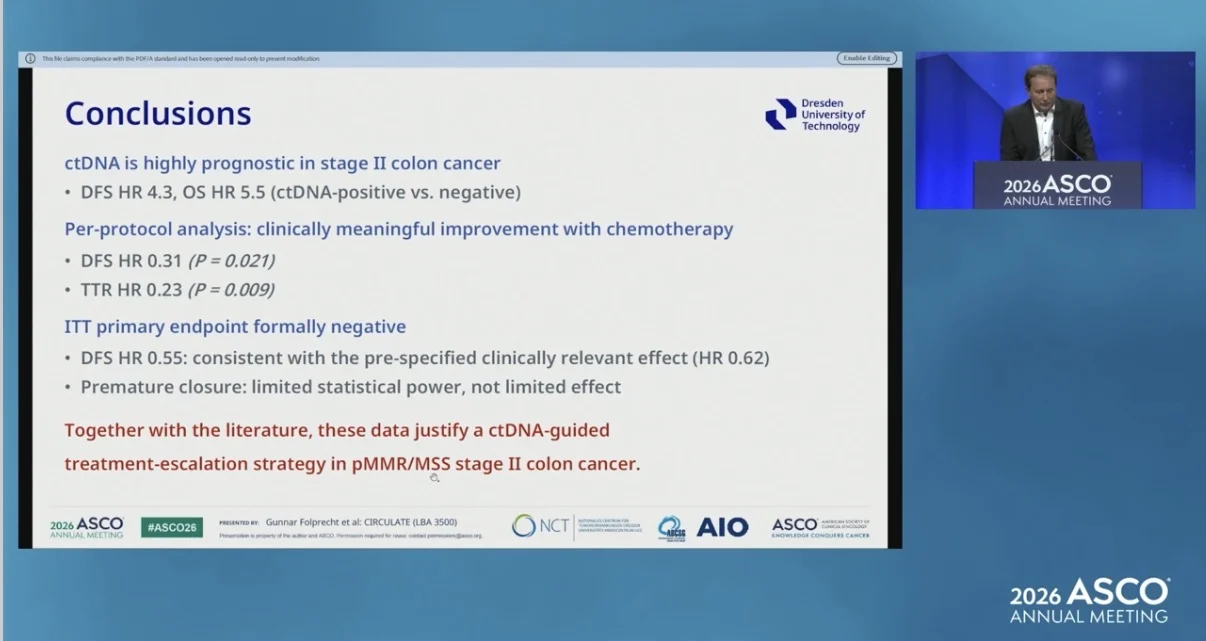
CIRCULATE showed that ctDNA was highly prognostic in stage II colon cancer. In the per-protocol analysis, chemotherapy was associated with clinically meaningful improvement in time to recurrence and disease-free survival among ctDNA-positive patients.

However, the intention-to-treat primary endpoint was formally negative. The observed effect was consistent with the prespecified clinically relevant effect, but the trial was limited by premature closure and reduced statistical power.Together with existing literature, these data support a ctDNA-guided treatment-escalation strategy in pMMR/MSS stage II colon cancer, while the low ctDNA-positive rate, early closure, and reliance on the per-protocol analysis remain important considerations.
The full abstract is available on the official ASCO website.
{kind=link}
{kind=link}
{kind=link}
{kind=link}