


A phase 2 study published in Clinical Breast Cancer evaluated whether combining tucatinib with trastuzumab deruxtecan could improve outcomes for patients with previously treated HER2-positive unresectable locally advanced or metastatic breast cancer.
The study, known as HER2CLIMB-04, showed that the combination had clinical activity, including in patients with brain metastases. However, the investigators concluded that a clear benefit beyond what has already been demonstrated with trastuzumab deruxtecan monotherapy was not observed.
The regimen was considered feasible and tolerable when given with antidiarrheal prophylaxis.
Why This Combination Was Tested
HER2-positive metastatic breast cancer has seen major treatment advances in recent years, especially with HER2-directed antibodies, antibody-drug conjugates, and tyrosine kinase inhibitors.
Trastuzumab deruxtecan, also known as T-DXd, has become a highly active HER2-directed antibody-drug conjugate across several treatment settings. Tucatinib is a HER2-selective tyrosine kinase inhibitor with demonstrated activity in HER2-positive metastatic breast cancer, including disease involving the central nervous system.
The biological rationale for combining the two agents was strong. Tucatinib targets the intracellular HER2 kinase domain, while T-DXd delivers a cytotoxic topoisomerase I inhibitor payload through HER2-directed antibody binding. Preclinical data suggested that tucatinib might enhance activity of HER2-targeted ADCs by increasing surface HER2 and improving ADC internalization.
HER2CLIMB-04 tested whether that rationale could translate into stronger clinical activity in patients whose disease had progressed after prior HER2-directed therapy and chemotherapy.

Study Design
HER2CLIMB-04 was a single-arm, open-label, multicenter phase 2 trial conducted in the United States.
The trial enrolled adults with HER2-positive unresectable locally advanced or metastatic breast cancer who had previously received trastuzumab and a taxane, and whose disease had progressed after prior systemic therapy or who were intolerant of previous treatment.
Patients with brain metastases were allowed, including those with stable or progressing treated brain metastases and selected patients with untreated brain metastases not requiring immediate local therapy.
A total of 70 patients received tucatinib 300 mg orally twice daily plus trastuzumab deruxtecan 5.4 mg/kg intravenously on day 1 of each 21-day cycle.
Among the enrolled patients, 43 had no brain metastases and 27 had brain metastases.
Response and Disease Control
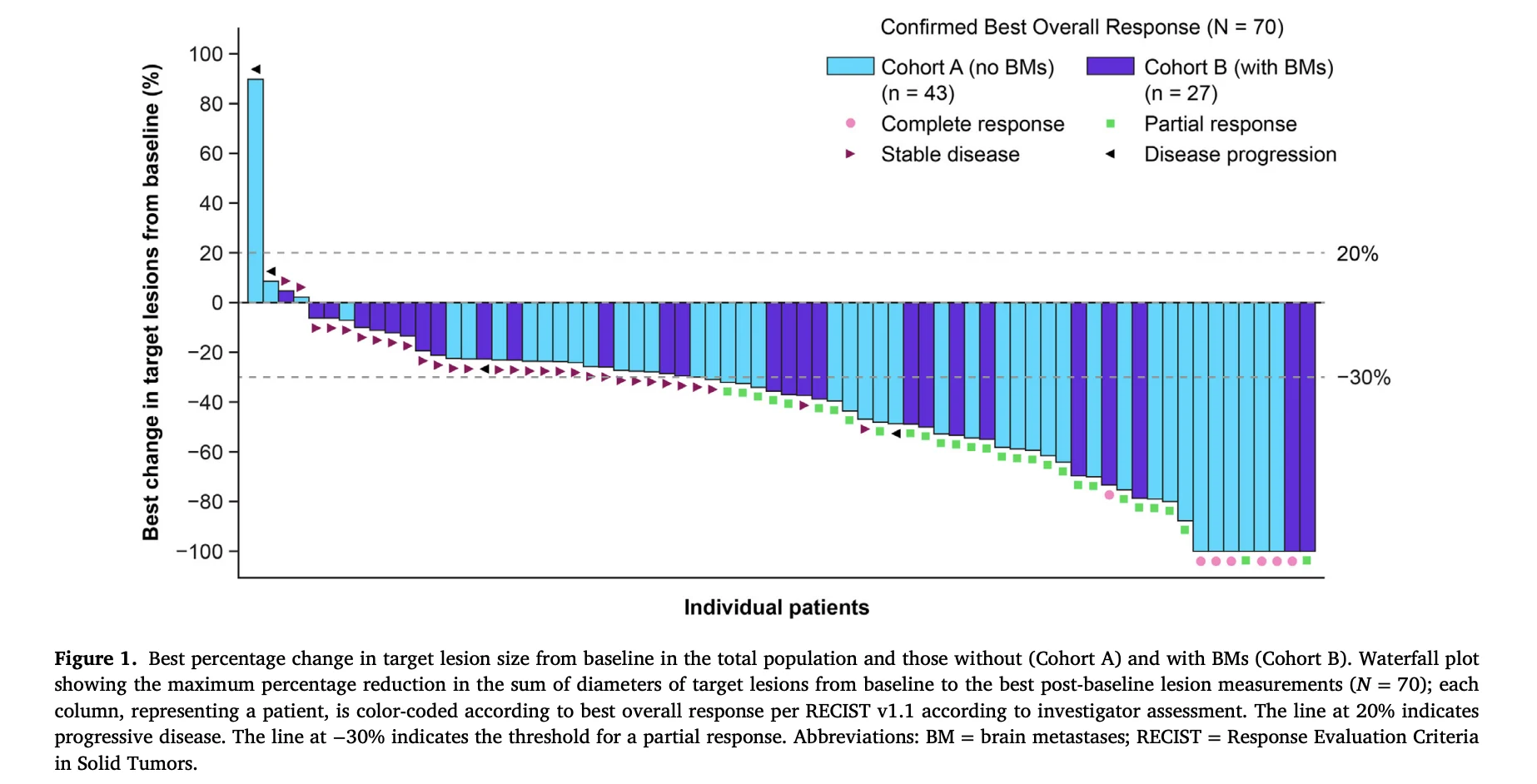
The confirmed objective response rate was 51.4% in the total population.
This included 7 complete responses and 29 partial responses. The disease control rate was 94.3%, and the median duration of response was 11.9 months.
Patients without brain metastases had a confirmed objective response rate of 55.8%, while those with brain metastases had a confirmed objective response rate of 44.4%.
The waterfall plot on page 5 shows tumor shrinkage across many treated patients, with several deep responses, including complete responses. However, the study authors noted that the response rate did not clearly exceed results previously reported with T-DXd monotherapy.

Progression-Free and Overall Survival
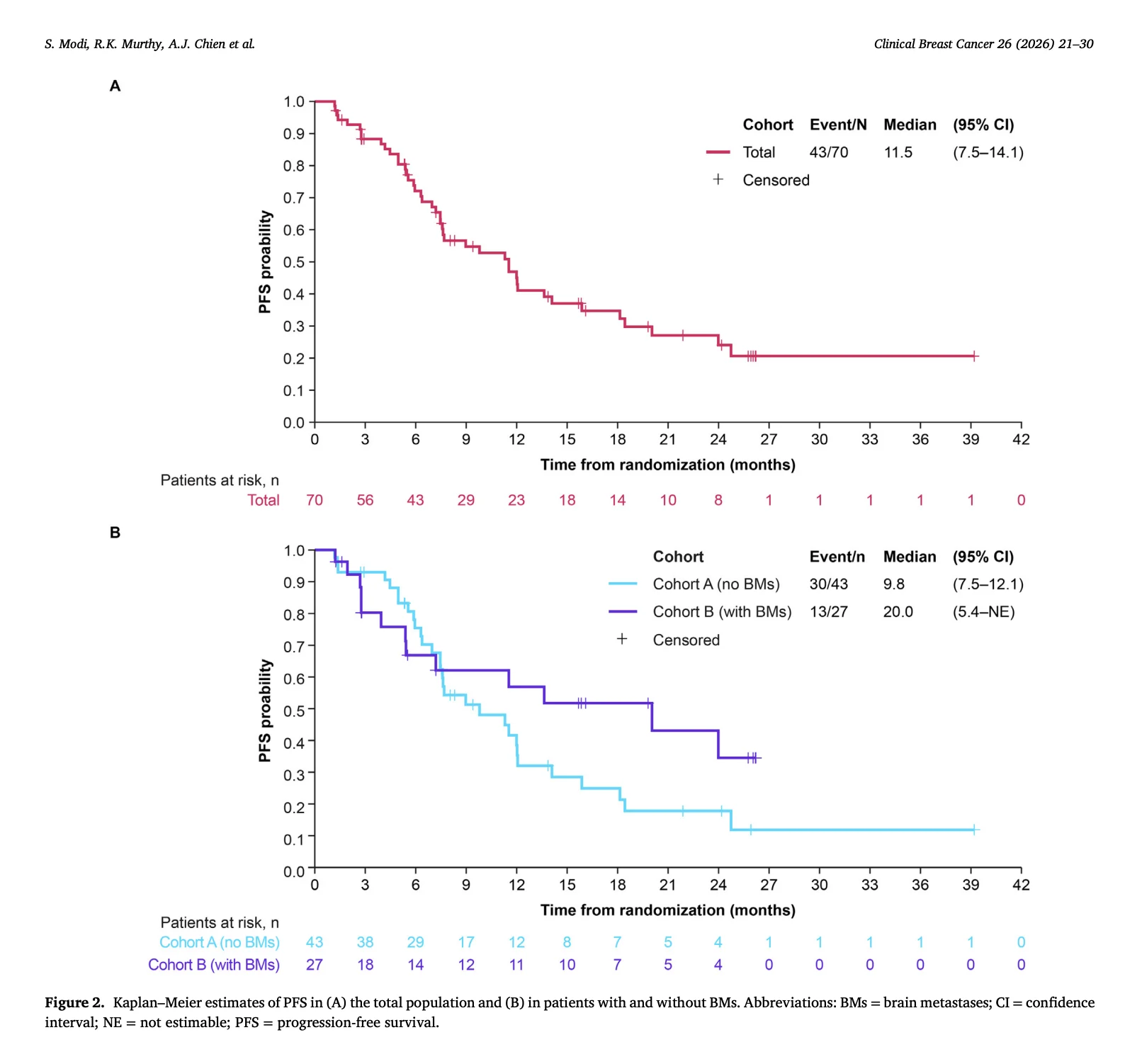
With a median follow-up of 27.3 months, median progression-free survival in the full study population was 11.5 months.
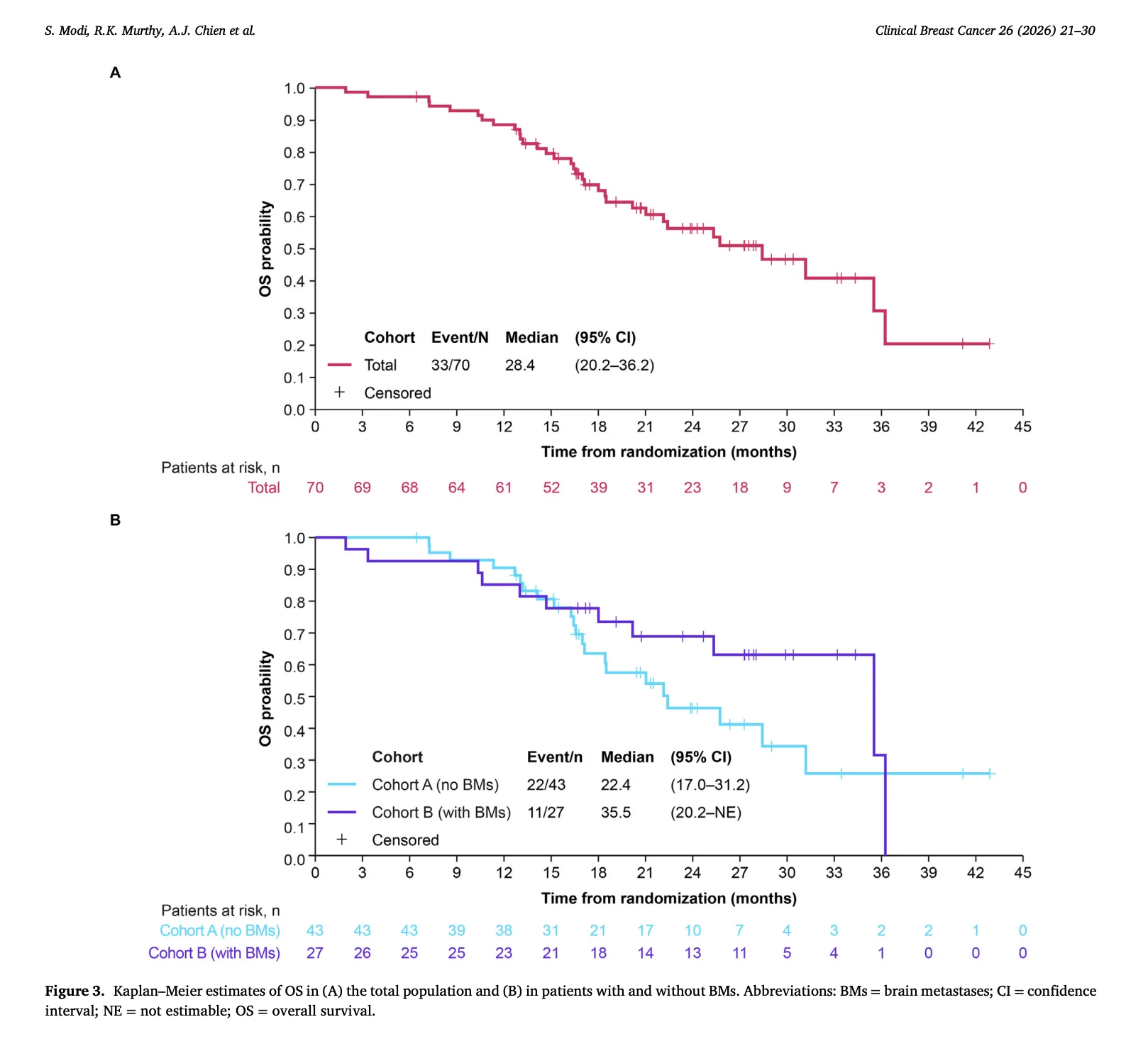
Median overall survival was 28.4 months.
Patients with brain metastases had numerically favorable outcomes. Median progression-free survival was 20.0 months in patients with brain metastases compared with 9.8 months in patients without brain metastases.
Median overall survival was 35.5 months in patients with brain metastases and 22.4 months in those without brain metastases.
The Kaplan-Meier curves on pages 7 and 8 show these PFS and OS patterns by brain metastasis status. The authors emphasized that these findings are encouraging but should be interpreted cautiously because the brain metastasis subgroup was small.
Brain Metastases Remain a Key Clinical Question
Brain metastases are common in HER2-positive metastatic breast cancer and remain a major clinical challenge.
In HER2CLIMB-04, patients with brain metastases represented 38.6% of the study population. Among them, 66.7% had treated stable brain metastases, 11.1% had treated progressive brain metastases, and 22.2% had untreated brain metastases.
The favorable survival outcomes in this subgroup reinforce the known CNS activity of tucatinib and T-DXd individually. However, because the trial was single-arm and did not include CNS-specific endpoints, it cannot prove that the combination provides added intracranial benefit beyond existing therapies.
Safety and the Role of Antidiarrheal Prophylaxis
All patients experienced at least one treatment-emergent adverse event, and 67.1% had a grade 3 or higher event.
The most common treatment-emergent adverse events were diarrhea, nausea, and fatigue. Diarrhea occurred in 80.0% of patients, nausea in 77.1%, and fatigue in 72.9%.
Interstitial lung disease occurred in 5.7% of patients, and pneumonitis occurred in 4.3% while on study treatment.
Early in the trial, diarrhea led to frequent dose modifications. The protocol was amended to require antidiarrheal prophylaxis with loperamide. After prophylaxis was introduced, any-grade diarrhea decreased from 88.5% to 75.0%, and grade 3 diarrhea decreased from 19.2% to 2.3%.
Importantly, no tucatinib discontinuations due to diarrhea occurred in the prophylaxis group, compared with 7.7% among patients who did not receive prophylaxis.
This finding is clinically relevant because it shows that supportive care can meaningfully affect tolerability when combining HER2-directed agents.
Why the Result Is Mixed
The study showed that tucatinib plus T-DXd is active, but the key question was whether the combination improves outcomes beyond T-DXd alone.
The authors concluded that a clear additional efficacy signal was not seen. Cross-trial comparisons must be interpreted cautiously, but previous T-DXd monotherapy studies have reported higher response rates and longer survival outcomes in some settings.
Several factors may have influenced the results. Only 58.6% of patients in HER2CLIMB-04 had HER2 IHC 3+ tumors, lower than in some major T-DXd trials. The study also included a relatively high proportion of patients with brain metastases, including active brain metastases.
Most importantly, the trial was small and single-arm, limiting the ability to determine additive benefit.

The Bottom Line
HER2CLIMB-04 showed that tucatinib plus trastuzumab deruxtecan has clinical activity in previously treated HER2-positive advanced or metastatic breast cancer.
The confirmed objective response rate was 51.4%, median progression-free survival was 11.5 months, and median overall survival was 28.4 months.
Patients with brain metastases had encouraging outcomes, with median PFS of 20.0 months and median OS of 35.5 months, although these subgroup results require caution.
The combination did not demonstrate a clear efficacy advantage over prior T-DXd monotherapy results, but it was feasible when antidiarrheal prophylaxis was used.
For HER2-positive metastatic breast cancer, the study adds useful safety and feasibility data, while reinforcing that future combination strategies need randomized evidence to define whether dual HER2 targeting can meaningfully improve outcomes.
References
- Modi S, Murthy RK, Chien AJ, Lin NU, McAndrew NP, Specht JM, et al. Tucatinib in combination with trastuzumab deruxtecan in patients with previously treated HER2+ unresectable locally advanced or metastatic breast cancer: an open-label phase 2 study. Clinical Breast Cancer. 2026;26:21-30. doi:10.1016/j.clbc.2026.05.010.
- Murthy RK, Loi S, Okines A, et al. Tucatinib, trastuzumab, and capecitabine for HER2-positive metastatic breast cancer. New England Journal of Medicine. 2020;382:597-609.
- Cortes J, Kim SB, Chung WP, et al. Trastuzumab deruxtecan versus trastuzumab emtansine for breast cancer. New England Journal of Medicine. 2022;386:1143-1154.
- Harbeck N, Ciruelos E, Jerusalem G, et al. Trastuzumab deruxtecan in HER2-positive advanced breast cancer with or without brain metastases: a phase 3b/4 trial. Nature Medicine. 2024;30:3717-3727.
- Lin NU, Murthy RK, Abramson V, et al. Tucatinib vs placebo, both in combination with trastuzumab and capecitabine, for previously treated HER2-positive metastatic breast cancer in patients with brain metastases. JAMA Oncology. 2023;9:197-205.
{kind=link}
{kind=link}
{kind=link}