


RENALC 2o24, the opening session of the ongoing RENALC-BLADDR-PROSCA 2024 Hybrid Global Forum on GU Oncology, took place on 26 (PM) November 2024.
This forum brings together experts from around the world to discuss the latest advancements in renal, bladder, and prostate cancer. The event features a hybrid format, combining in-person and virtual sessions, with a focus on translating new data into clinical practice. RENALC 24 specifically addresses cutting-edge topics in renal cancer, offering a platform for knowledge exchange and interactive discussions.
BLADDR is scheduled for 27 November 2024 (full day) and 28 November 2024 (AM), while PROSCA is scheduled for 29 November 2024 (full day) and 30 November 2024 (AM).
María Natalia Gandur Quiroga is a Medical Oncologist and Chief of the Division of Genitourinary Medical Oncology at the Ángel H. Roffo Oncology Institute in Buenos Aires, Argentina. She is a Professor of Medicine at the University of Buenos Aires at the Oncologists Post Graduates Studies. Her research focuses on clinical trials with aims to improve the treatment of patients with urologic tumors. She is an active member of the European Association for Cancer Research, Argentinian Medical Association and American Society of Clinical Oncology.
María Natalia Gandur Quiroga shared her insights from RENALC24:
“Highlights from RENALC24: RCC Management Insights for 2025 Looking ahead: RCC management in 2025
Moderator: Saeed Dabestani
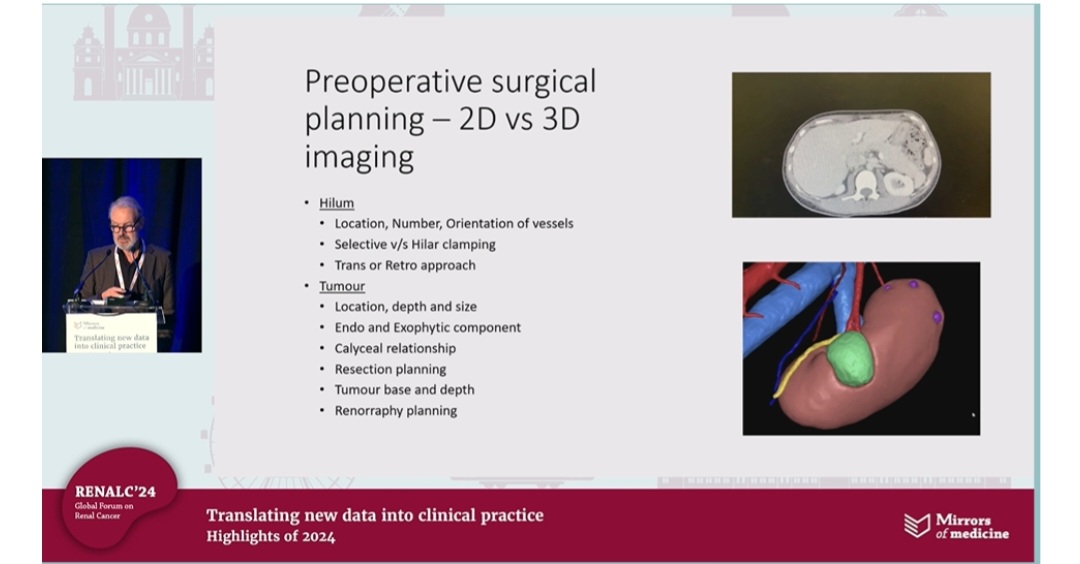
– Pre-op imaging: Transitioning from 2D to advanced 3D imaging for precise surgical planning. Key focus on tumor depth, size, and vessel orientation.
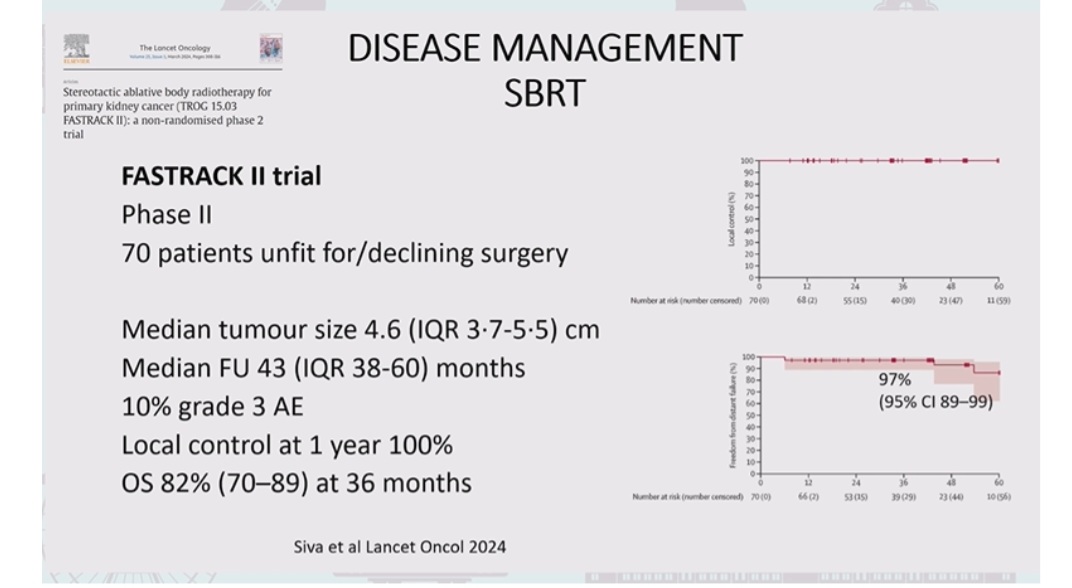
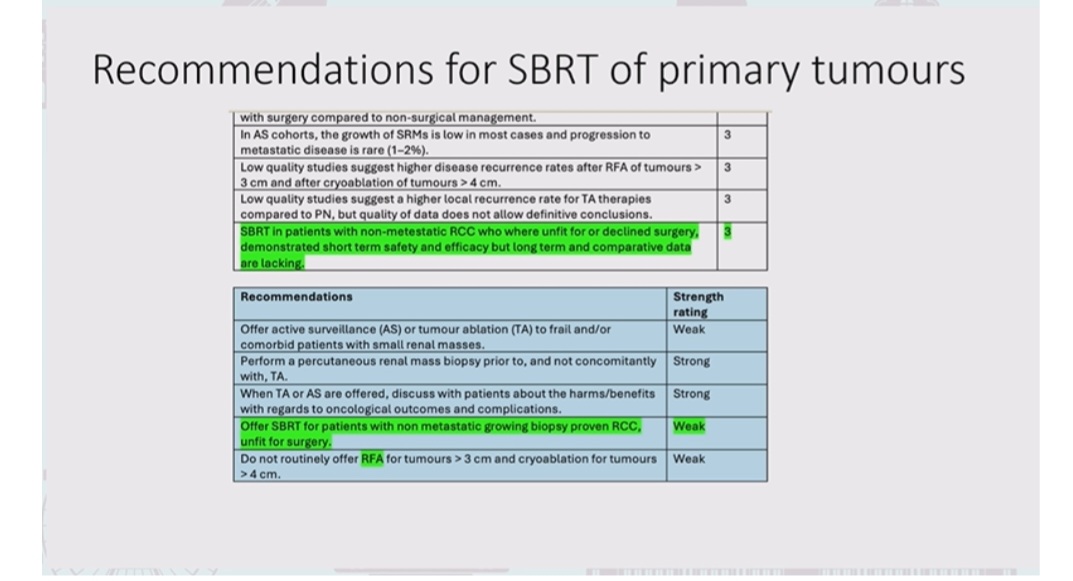
– SBRT advancements: New MRI LINAC studies emphasize safety and efficacy in non-surgical RCC patients.
– Updated DFS data: Pembrolizumab shows 35% recurrence despite use, but 57% cured by surgery alone.
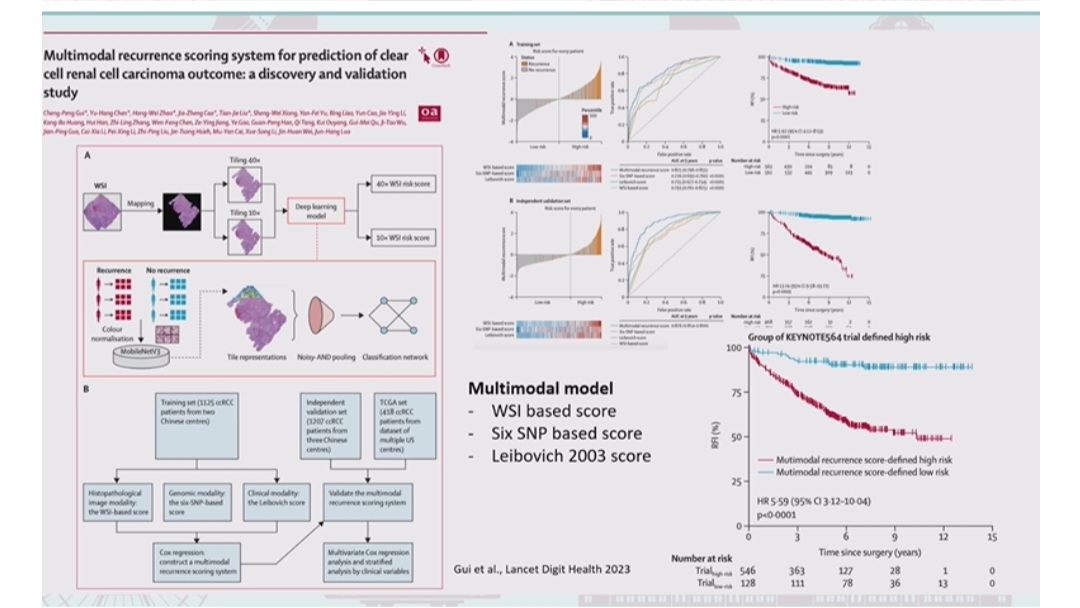
– Leibovich 2003 Validation: Improved risk discrimination in RCC survival metrics.
– Neoadjuvant RCC trials: 16 ongoing! Exploring PD-1/PD-L1 combos & innovative endpoints for better pathologic responses.
– NESCIo study design: 3-arms comparing nivolumab, ipilimumab, and relatlimab for high-risk RCC. Exciting phase II outcomes ahead!
– Atezolizumab DFS advantage: Particularly effective in KIM-1^high subgroup.
– Future view by urologists: Tailored approaches with focus on combined immunotherapy & targeted TKIs for advanced RCC.”

To operate or not? Axel Bex FOR YES:
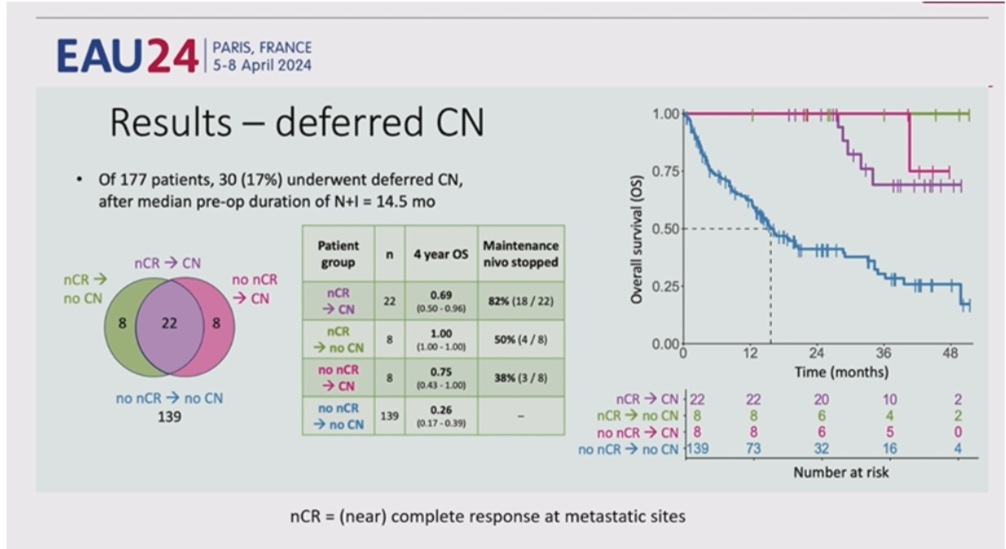
Debate: To operate or not? Deferred cytoreductive nephrectomy in the ICI era=
Axel Bex FOR YES and Pignot Géraldine FOR NO
FOR YES:
Key Points:
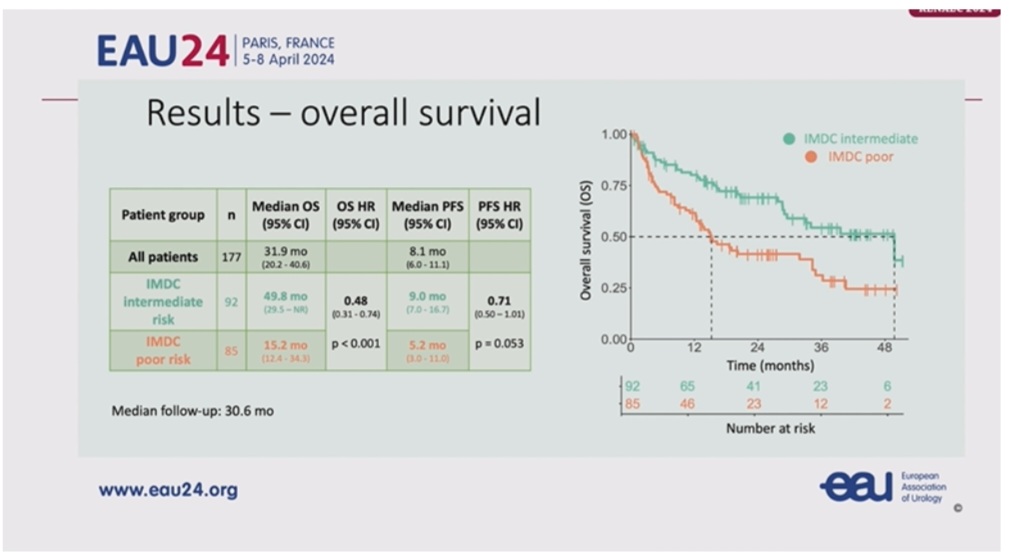
– Real-world data shows 17% underwent deferred CN with NIVO+IPI.
– Median OS: 31.9 months (intermediate risk: 49.8m, poor risk: 15.2m).
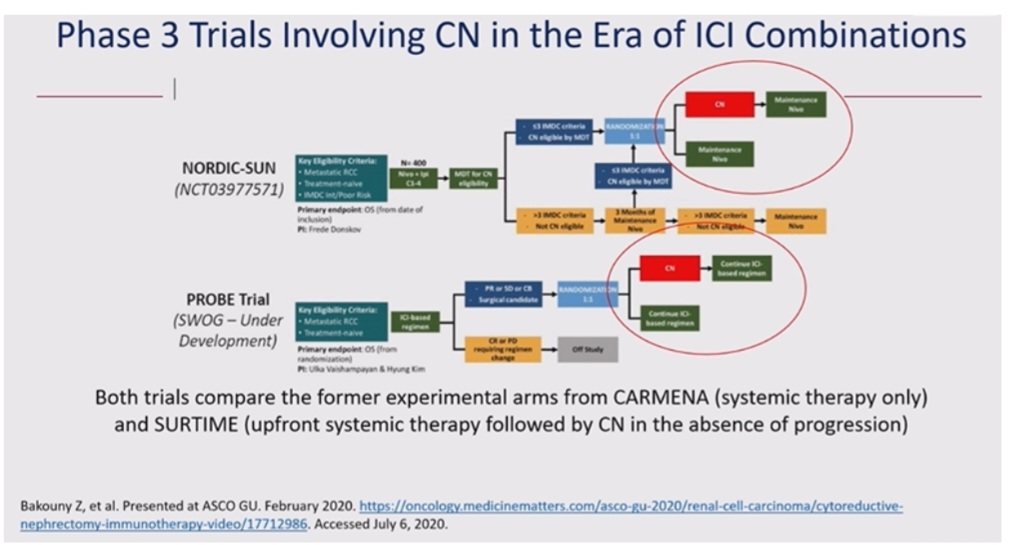
– Ongoing trials (NORDIC-SUN, PROBE) will clarify the role of deferred CN.”

To operate or not? Pignot Géraldine FOR NO:
“Debate: To operate or not? Deferred cytoreductive nephrectomy in the ICI era
Axel Bex FOR YES and Pignot Géraldine FOR NO
FOR NO:
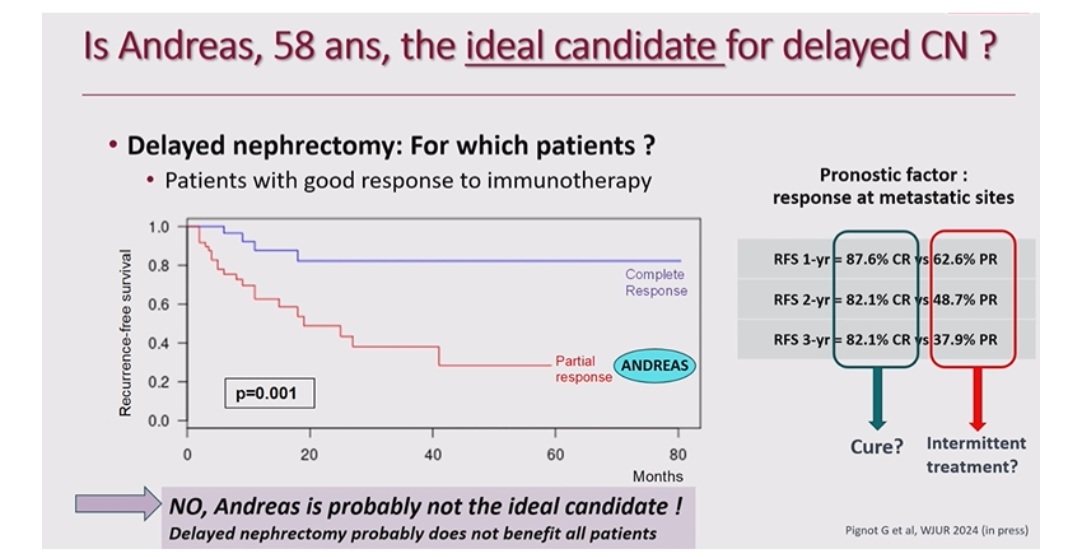
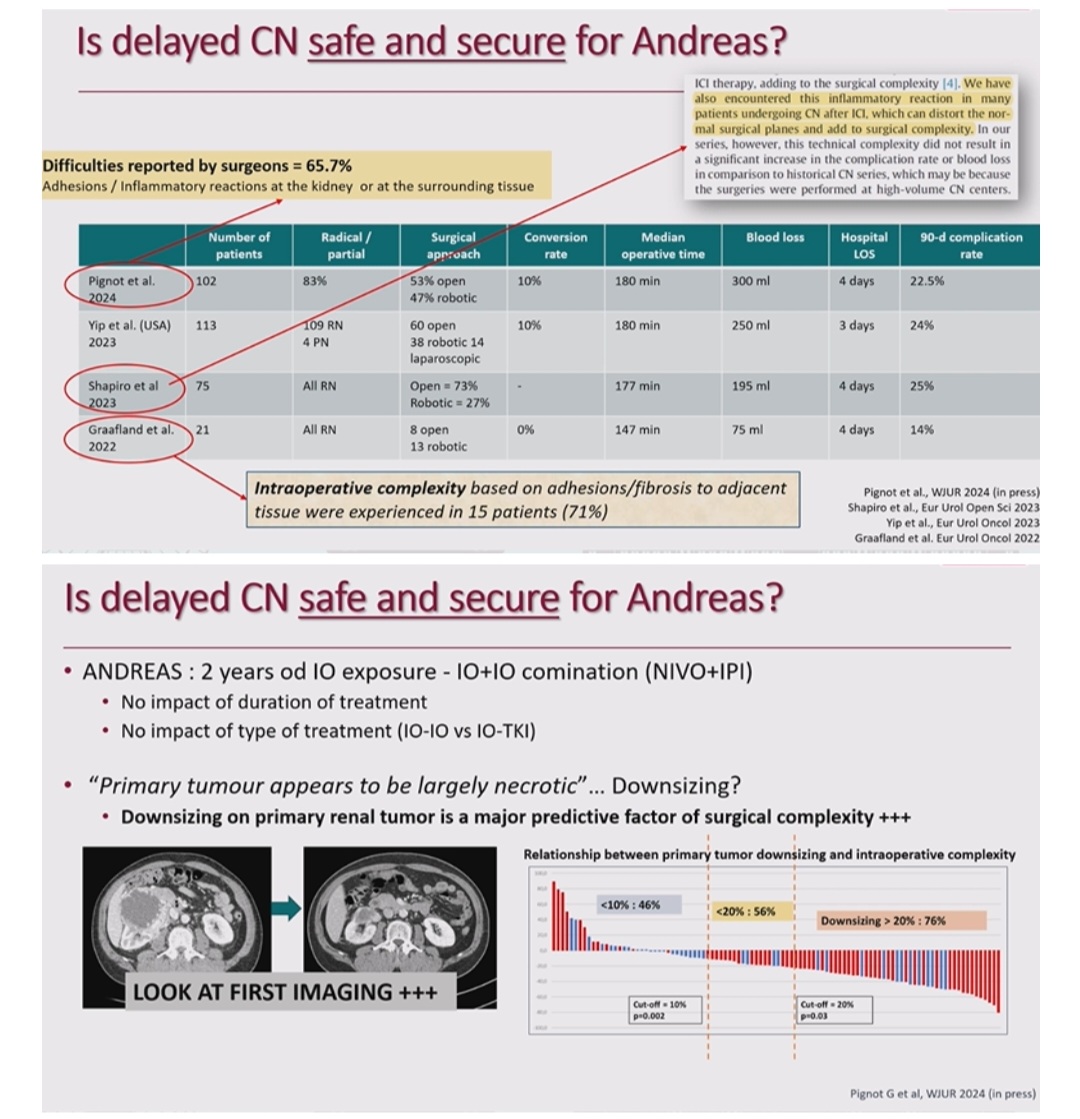
Delayed CN may benefit patients with complete response to immunotherapy but shows limited value for partial responders. Andreas is not ideal for delayed CN.
Surgical complexity is influenced by primary tumor downsizing (>20% = 76% complexity). Adhesions/fibrosis complicate 71% of surgeries.
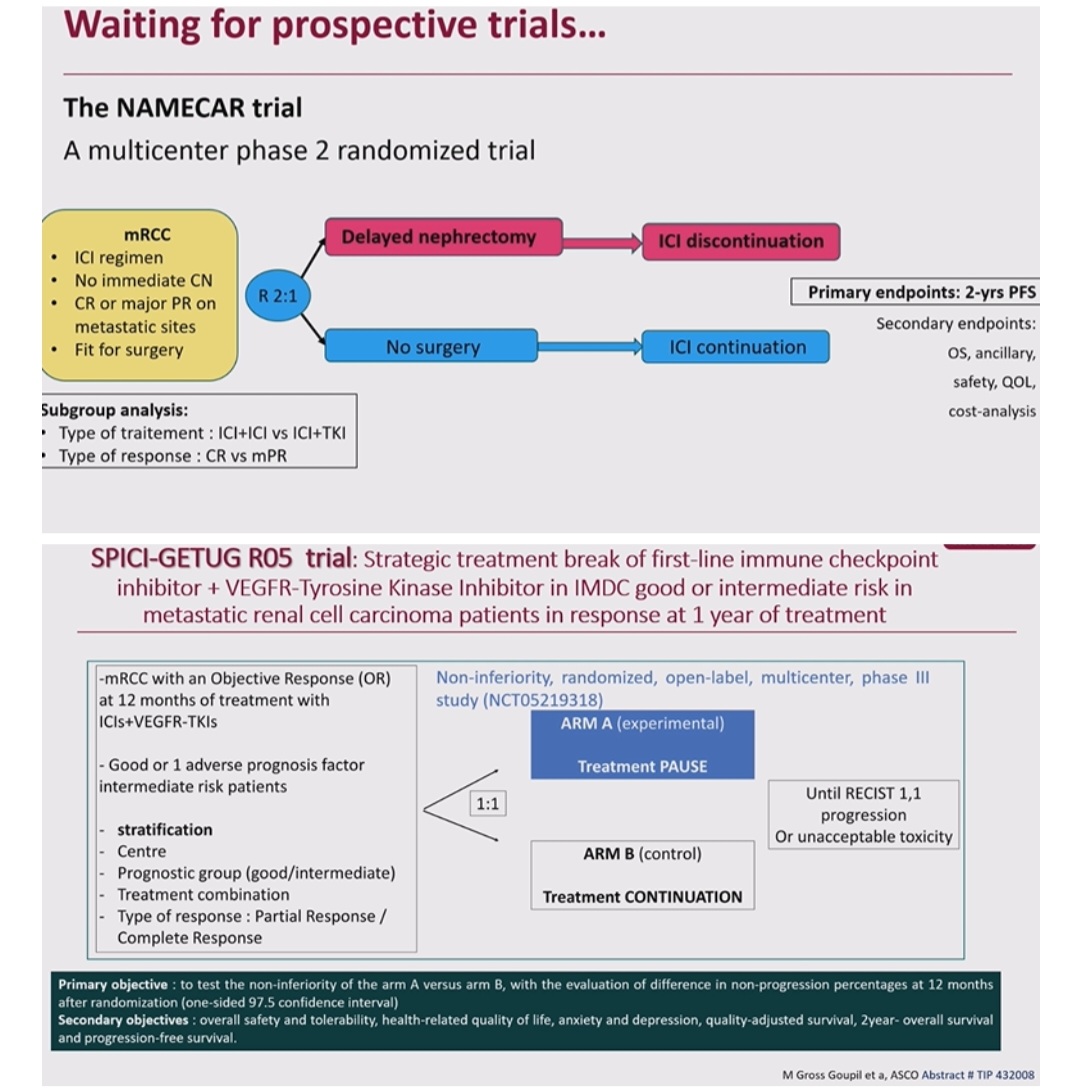
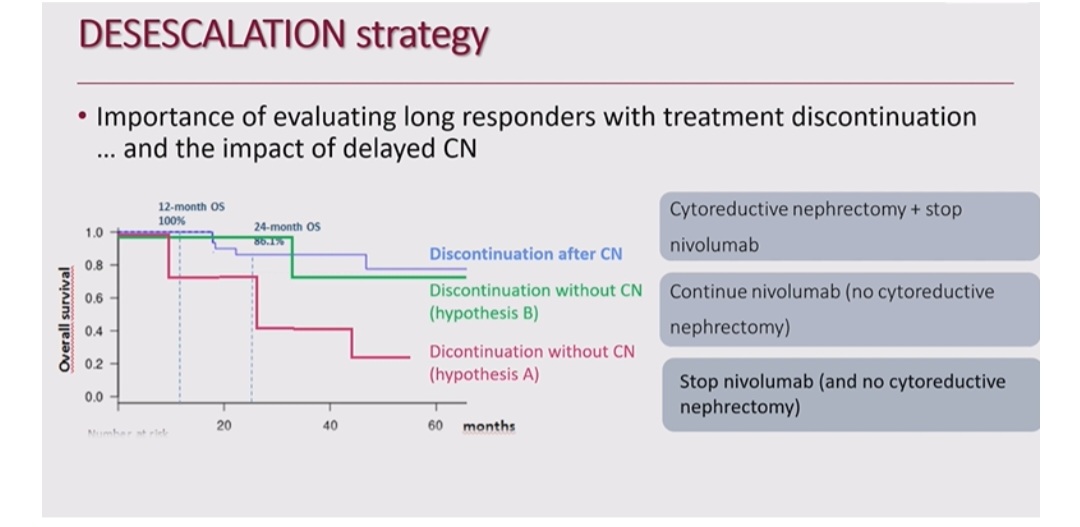
New strategies & trials (NAMECAR, SPICI-GETUG R05) explore treatment pauses and desescalation for select responders.
Personalized approaches to CN decision-making are evolving!”

Case presentation by Petros Grivas:
“SUPER Case presentation!! and enriching discussion!!
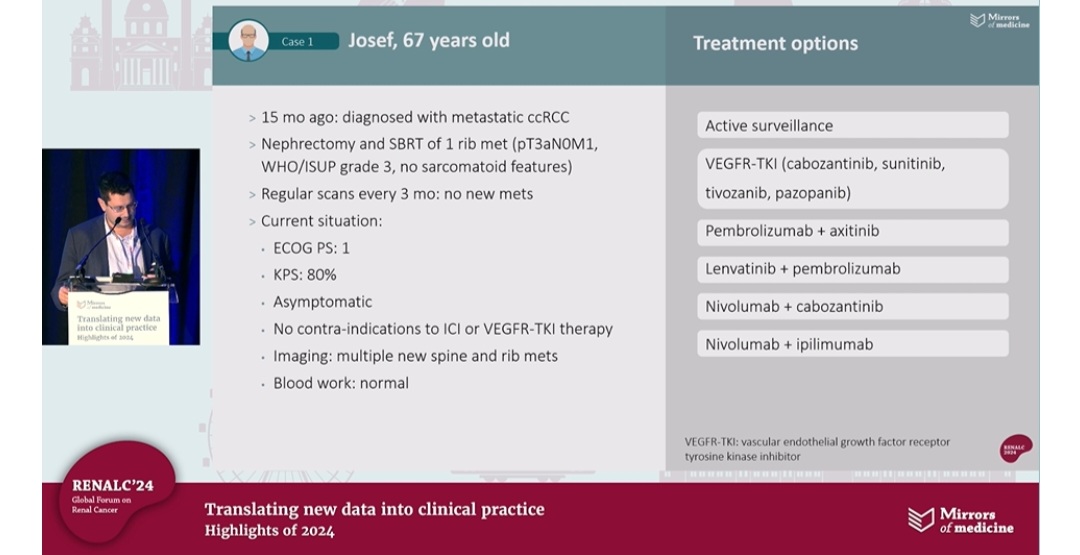
Case Study: Josef (67 years old). Diagnosed with metastatic ccRCC (15 months ago):
Nephrectomy & SBRT for 1 rib met.
ECOG PS: 1 | KPS: 80% | Asymptomatic.
Treatment Options:
– Active Surveillance
– VEGFR-TKI
– IO combinations: Nivolumab, Pembrolizumab, Ipilimumab.
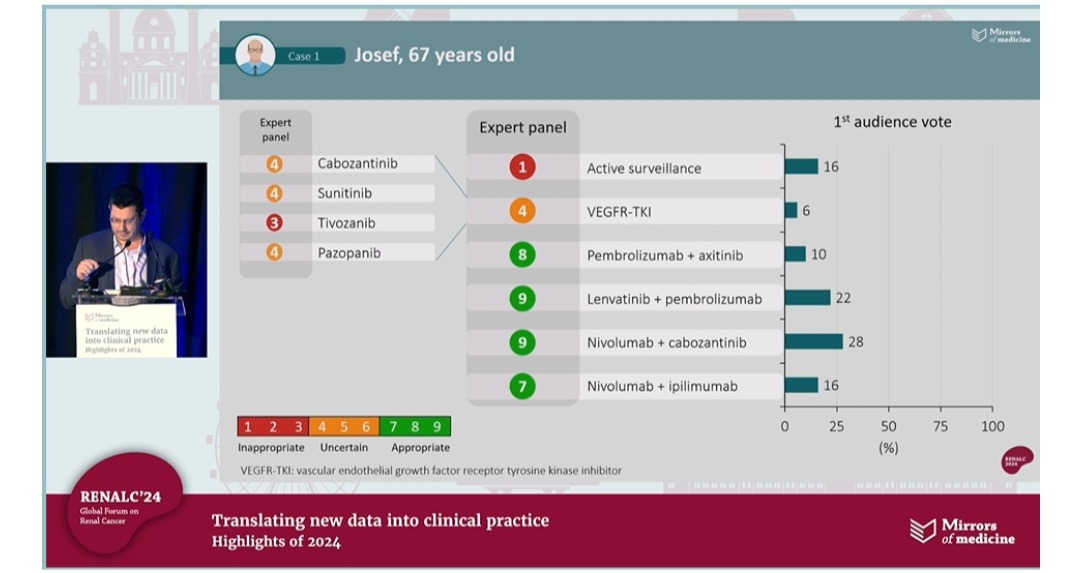
Audience Votes:
Top choice: Nivolumab + Cabozantinib (28%). Lenvatinib + Pembrolizumab (22%).
Panel Recommendations: Best-rated: Lenvatinib + Pembrolizumab & IO combos scored highly!”

Treatment options for patients with metastatic papillary RCC:
“Treatment options for patients with metastatic papillary RCC
Key insights on metastatic papillary RCC from RENALC24:
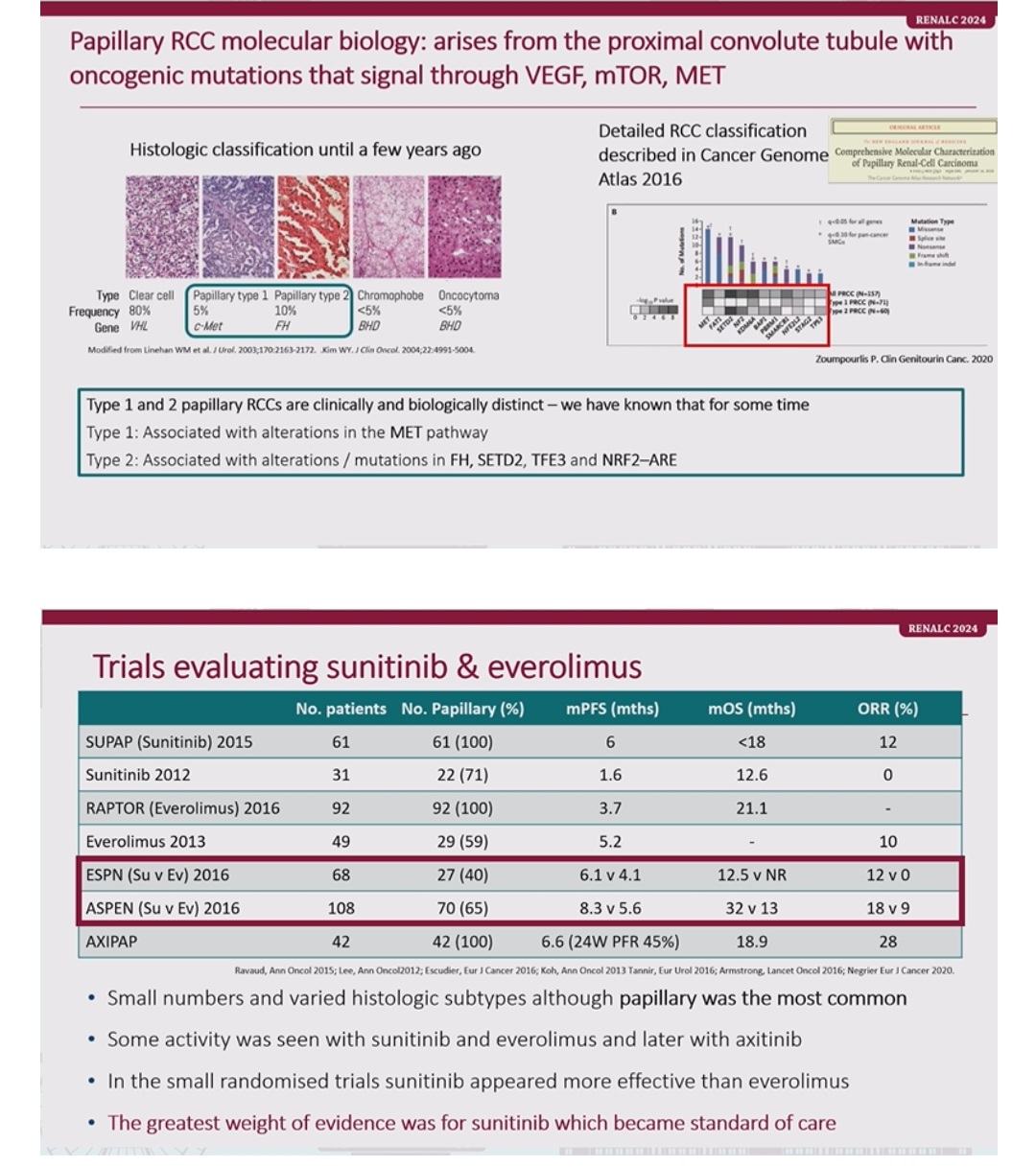
– Molecular insights: Papillary RCC arises through VEGF, MET, and mTOR pathways. Type 1 (MET mutations) vs Type 2 (FH, TFE3 alterations).
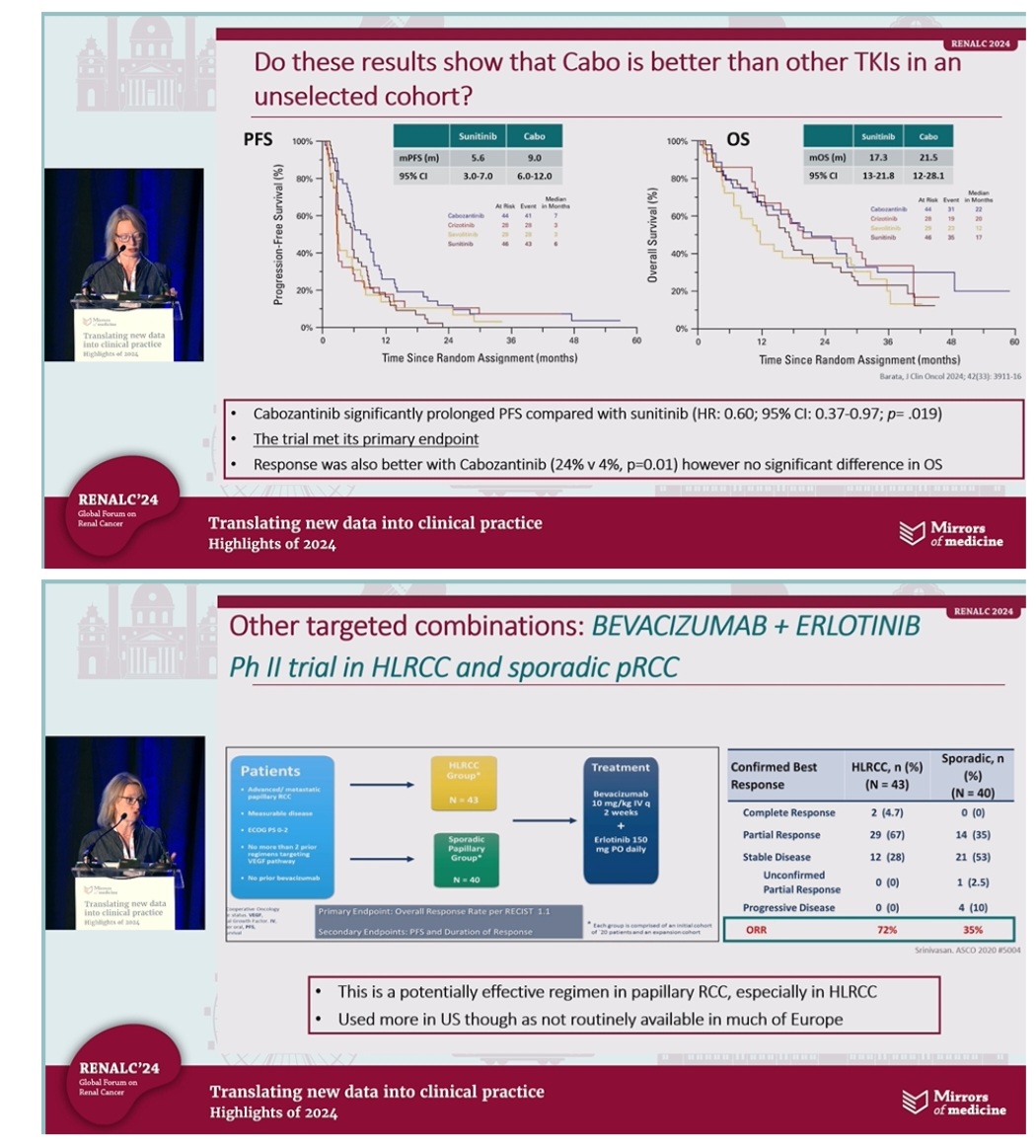
– Cabozantinib improves PFS (9 vs 5.6m) & ORR in unselected cohorts vs sunitinib (p=0.019).
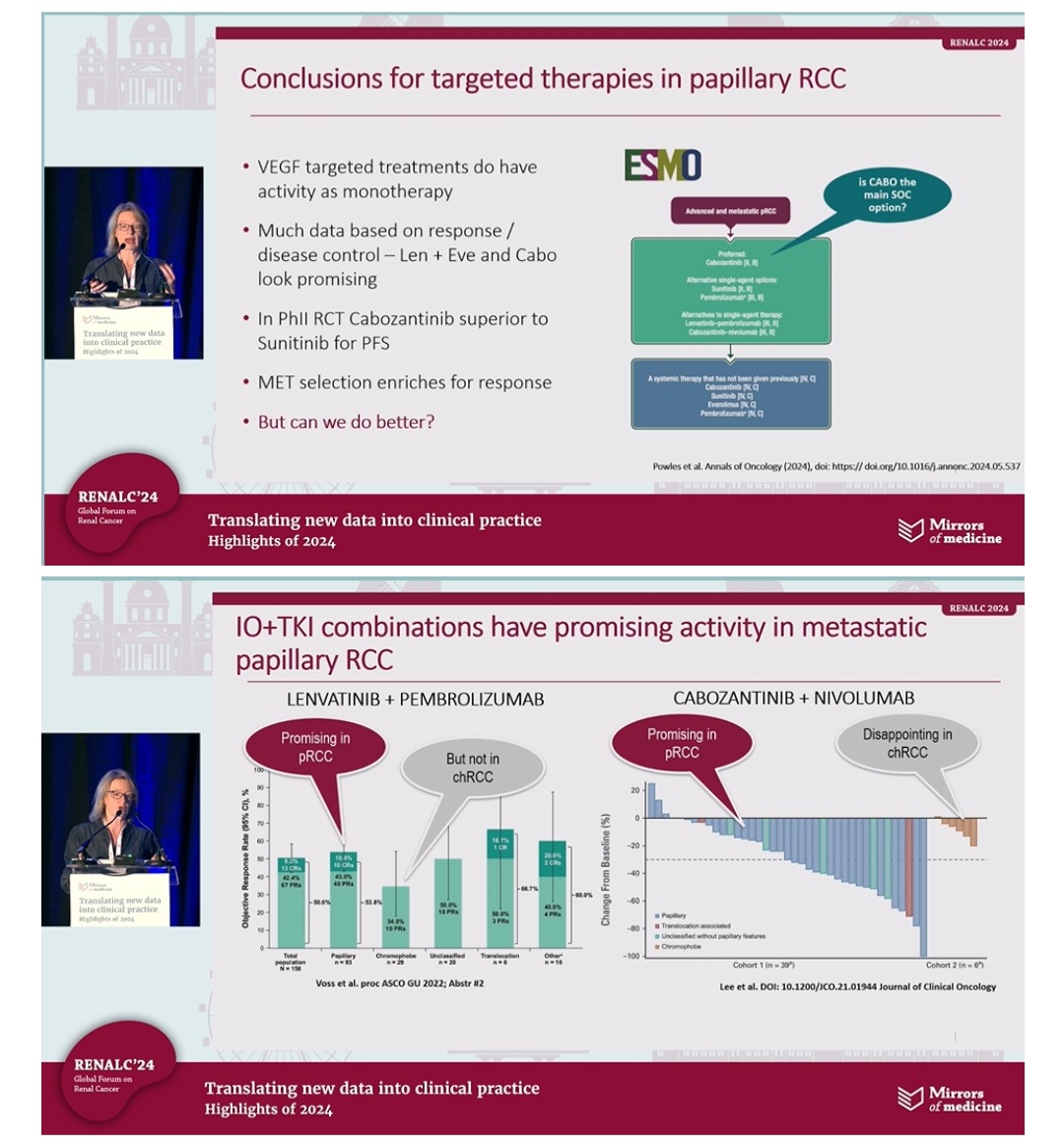
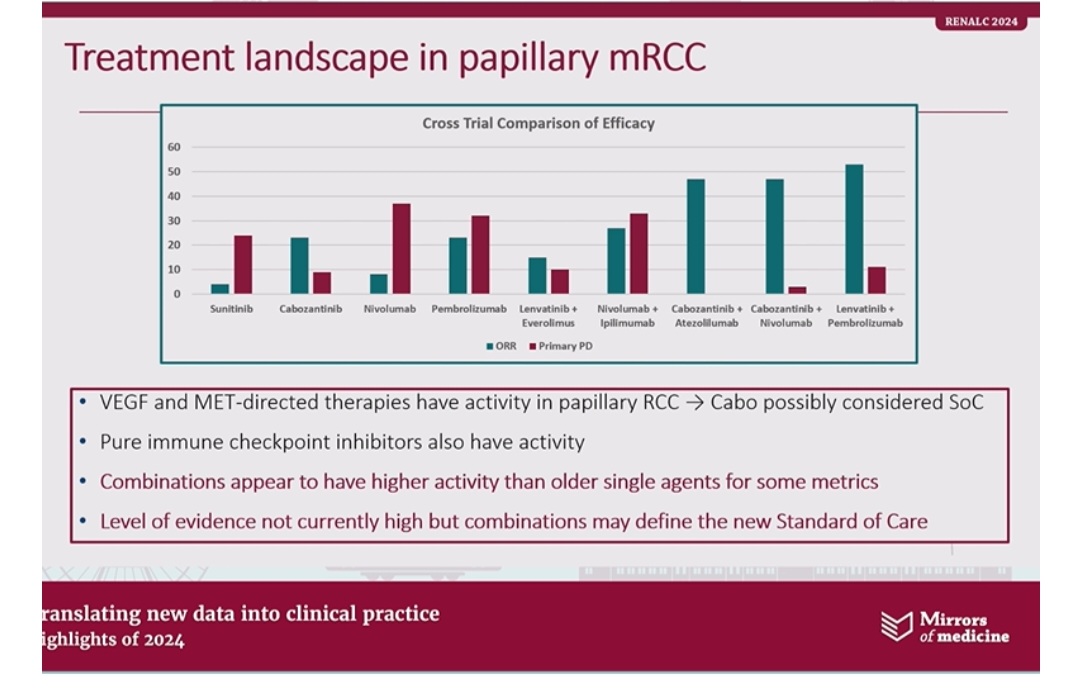
– VEGF-targeted therapies & combos like Lenvatinib+Eve/Cabo show promise in response rates.
– Promising IO-TKI: LenPem excels in pRCC; combos shaping new standards of care.
– Bevacizumab+Erlotinib: Highly effective in HLRCC (ORR 72%), less so in sporadic pRCC (35%).”

First-line treatment for advanced clear-cell RCC:
“Selecting first-line treatment for advanced clear-cell RCC
Highlights from RENALC24: Translating Data to Practice!
1. Local therapy matters in mRCC
– Surgery or radiotherapy improves survival: 106 vs 59 months.
– Systemic therapy received by 93% of patients.
– Key takeaway: Local interventions + systemic treatment = better outcomes.
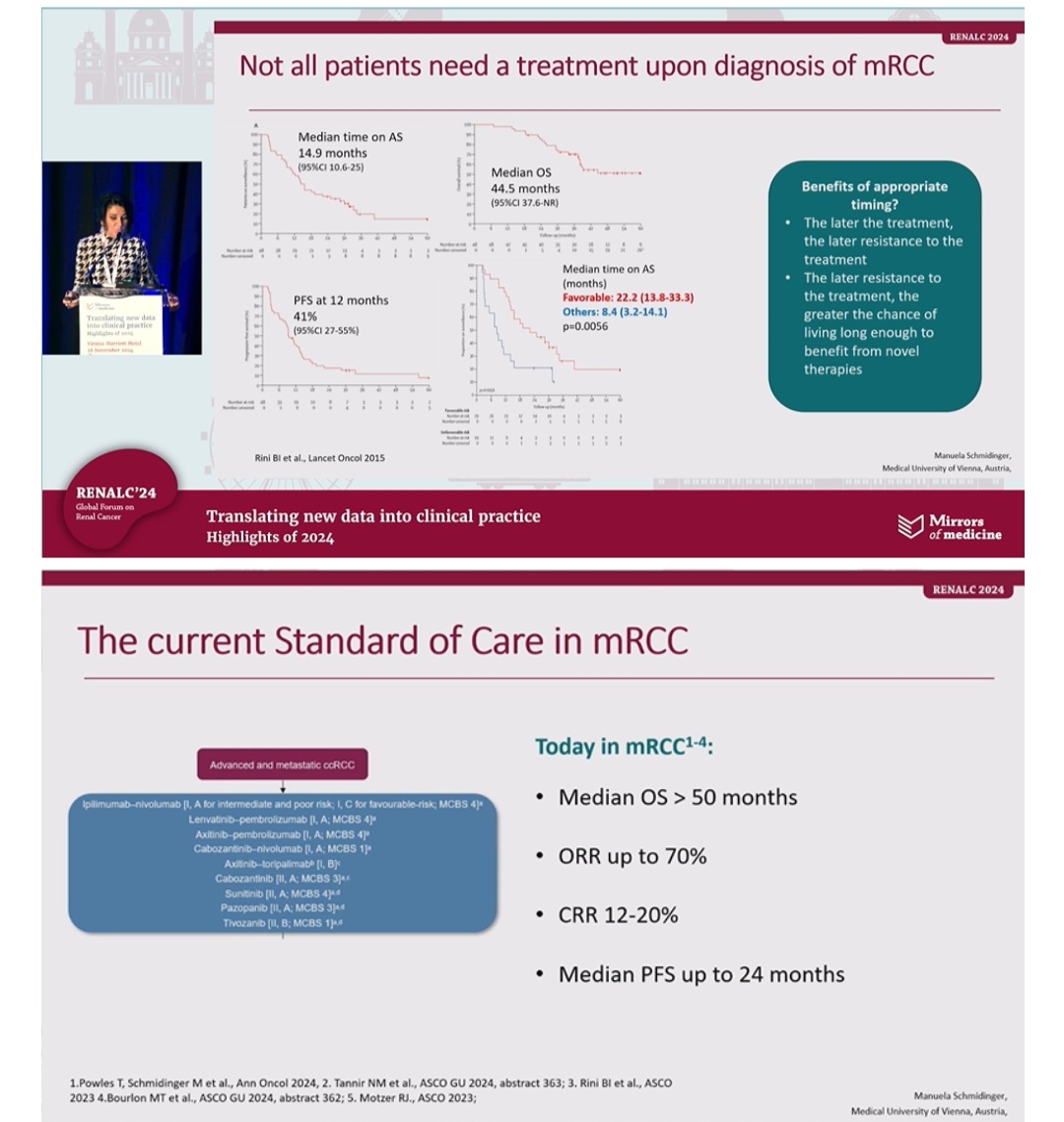
2. Timing in mRCC treatment
– Active surveillance (AS): Median time = 14.9 months. Median OS on AS = 44.5 months.
– Benefits of late treatment: Delayed resistance = greater benefit from novel therapies!
3. Current Standard of Care
– Median OS > 50 months. ORR up to 70%. PFS up to 24 months.
– Immunotherapy (ICI) combos remain pivotal!
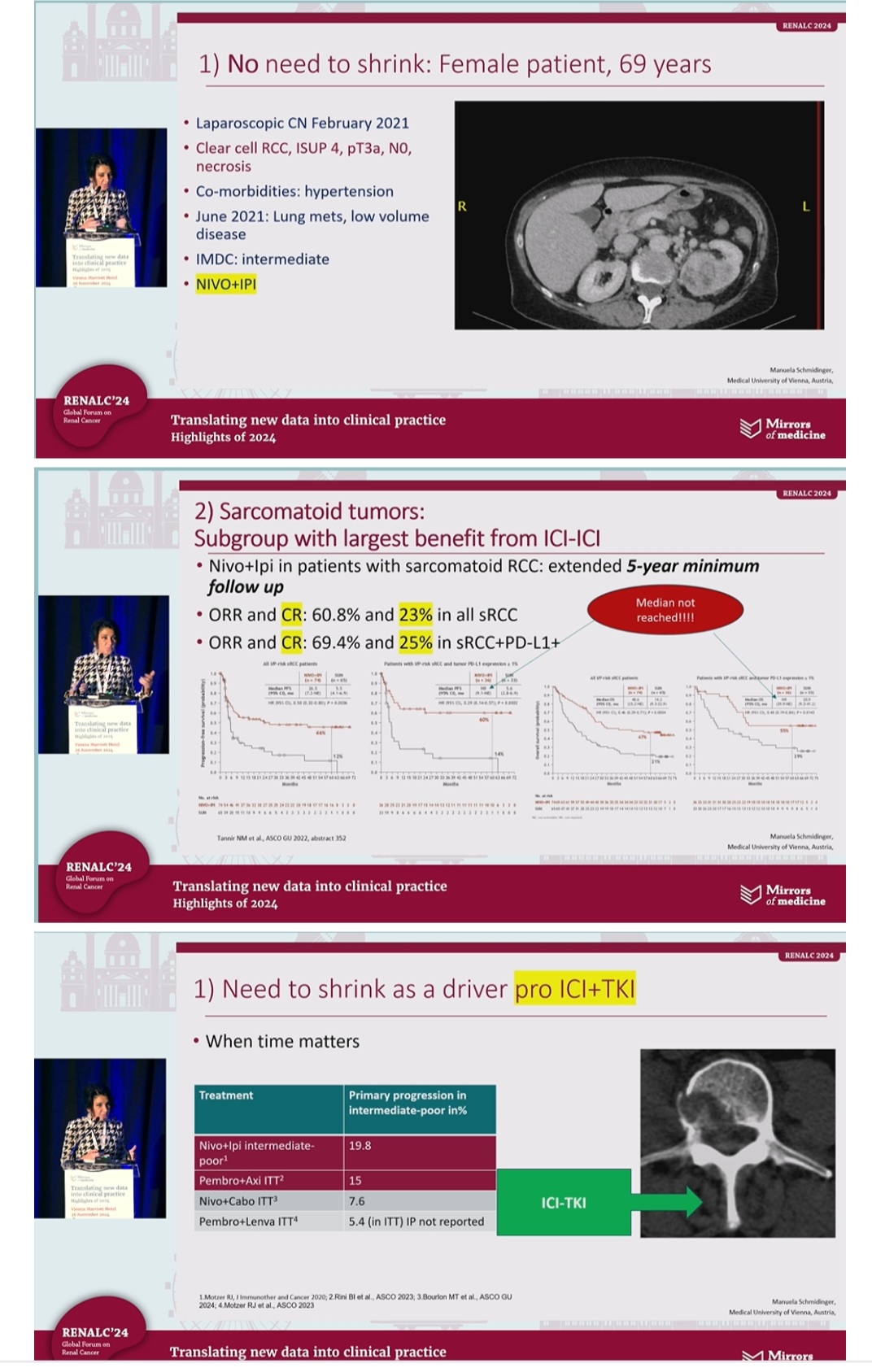
4. Sarcomatoid RCC patients
– Best responders to ICI-ICI (Nivo+Ipi):
– ORR: 60.8%, CR: 23% (all sRCC).
– ORR: 69.4%, CR: 25% (PD-L1+ sRCC).
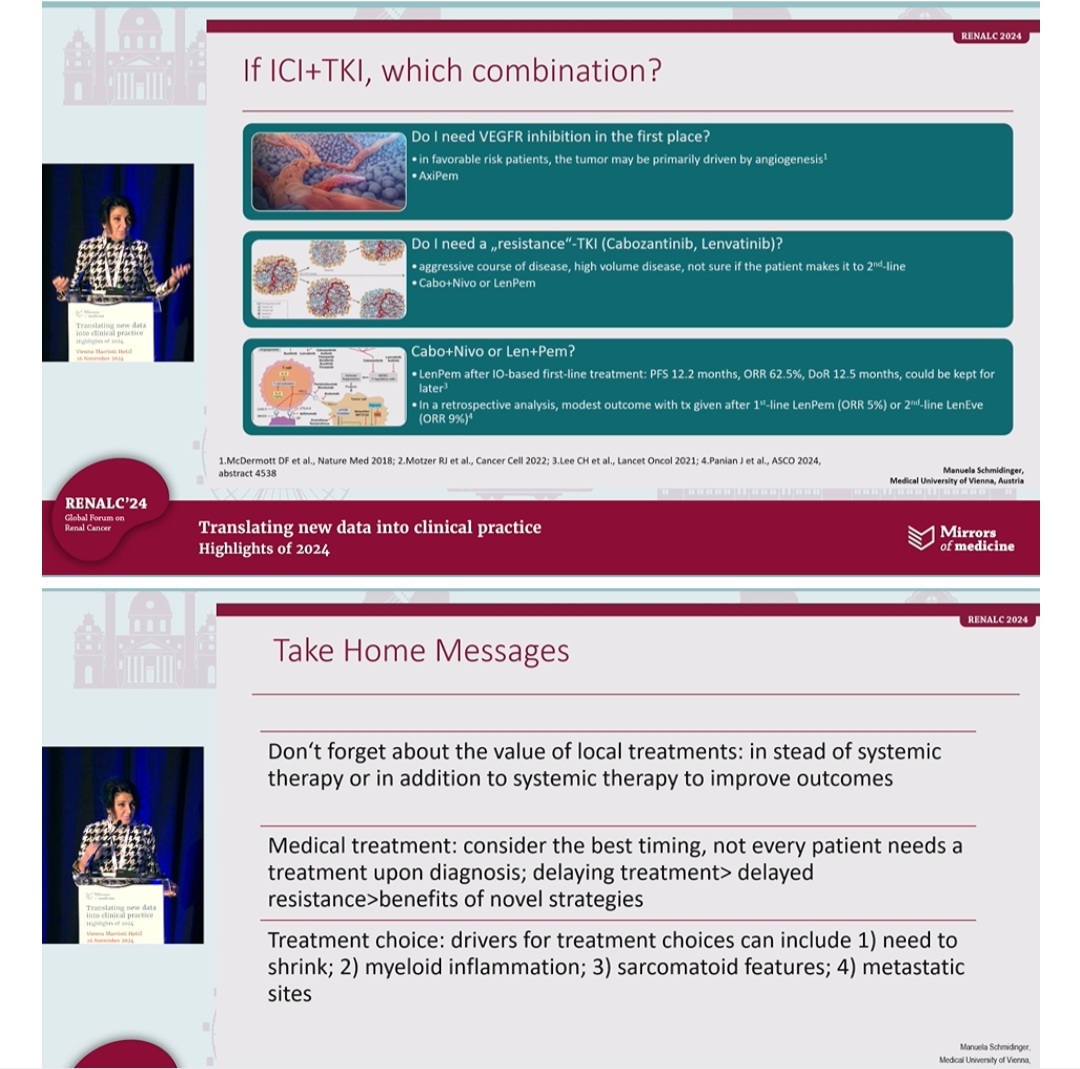
5. Brain & pancreatic mets impact treatment
– ICI-TKI > ICI or TKI alone for brain metastases.
– Pancreatic mets benefit more from ICI+TKI.
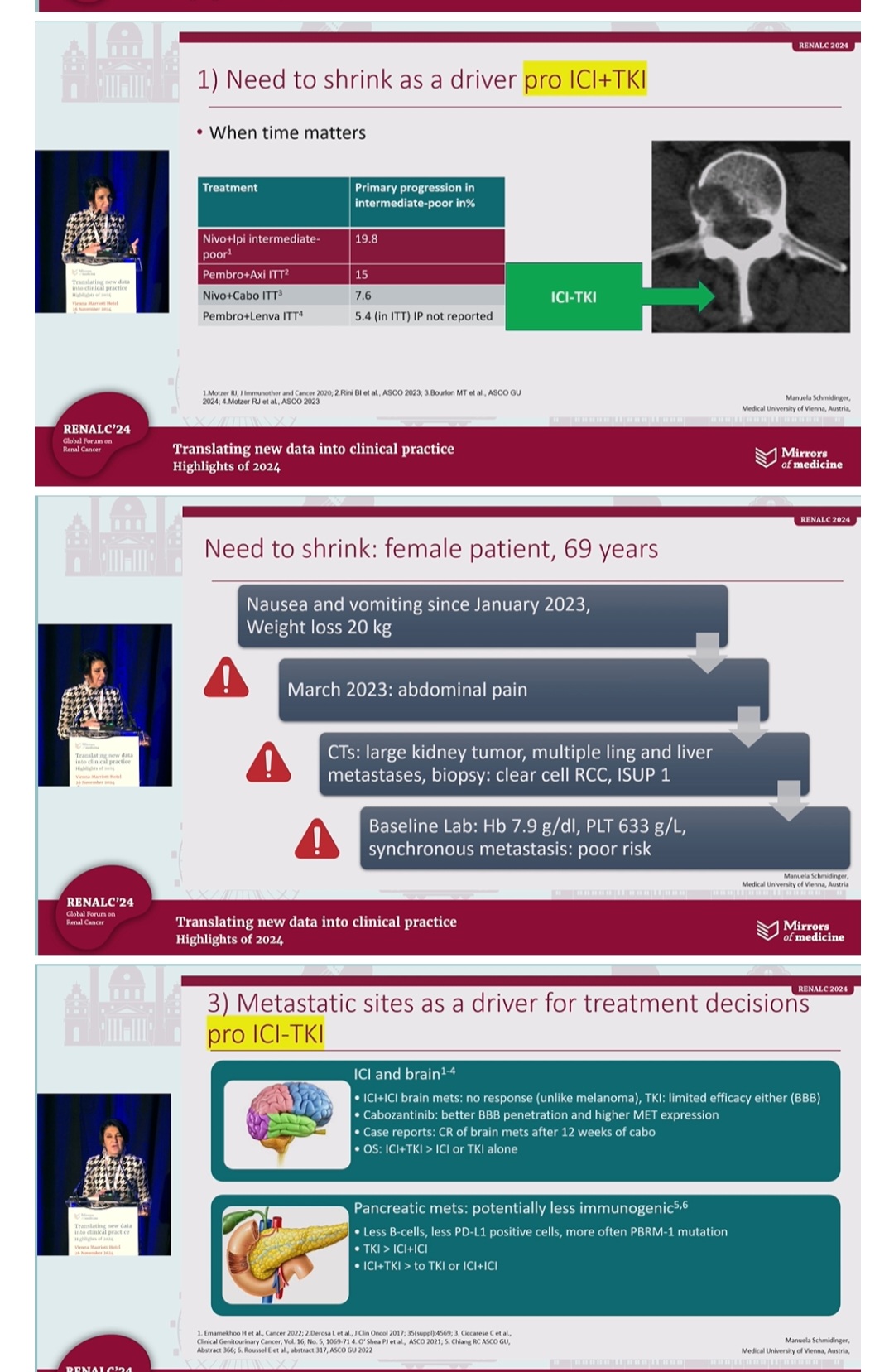
6. Choosing the right combo
– Favorable risk: VEGFR inhibition (Axi+Pem).
– Aggressive disease: Resistance-TKIs (Cabo+Nivo or Len+Pem).”

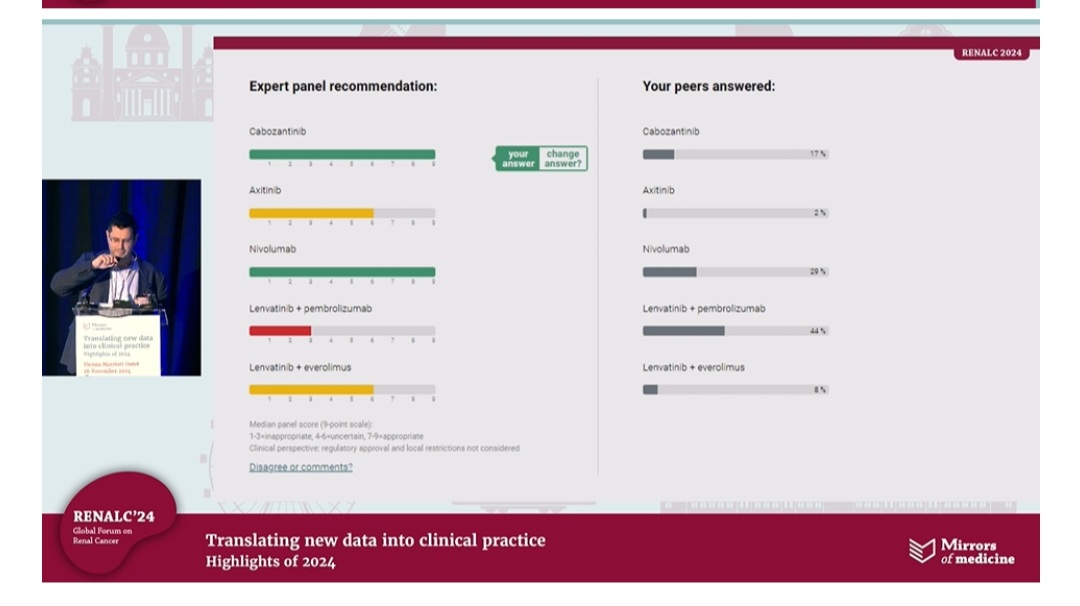
Case-based approach by Petros Grivas:
“Translating New Data into Clinical Practice: Case discussions highlight the role of evidence in decision-making! Key takeaways from RenalC24:
Mirrors of Medicine – case-based approach by Petros Grivas.
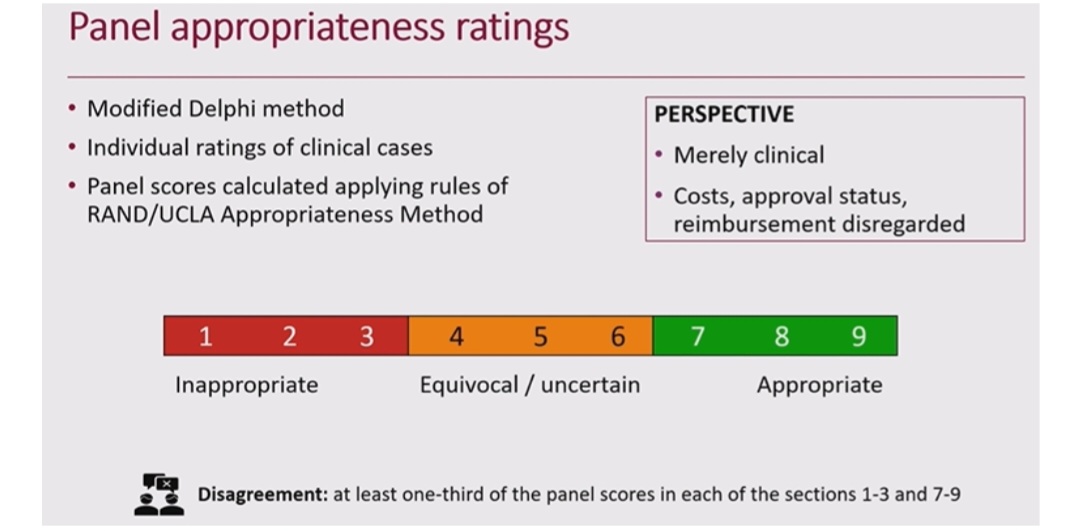
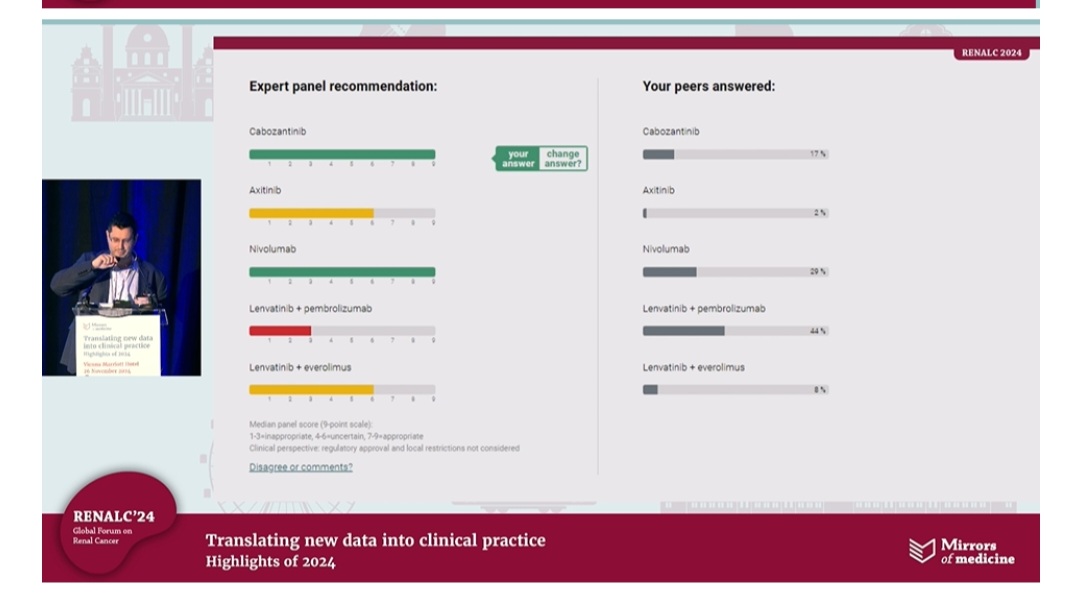
Panel ratings: Using the Delphi method to evaluate clinical cases with focus on appropriateness.
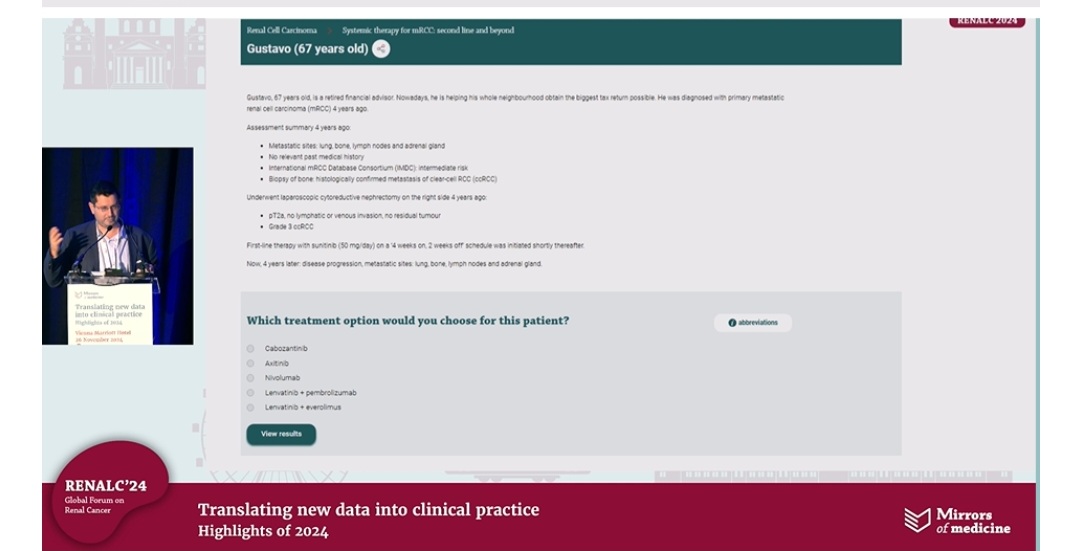
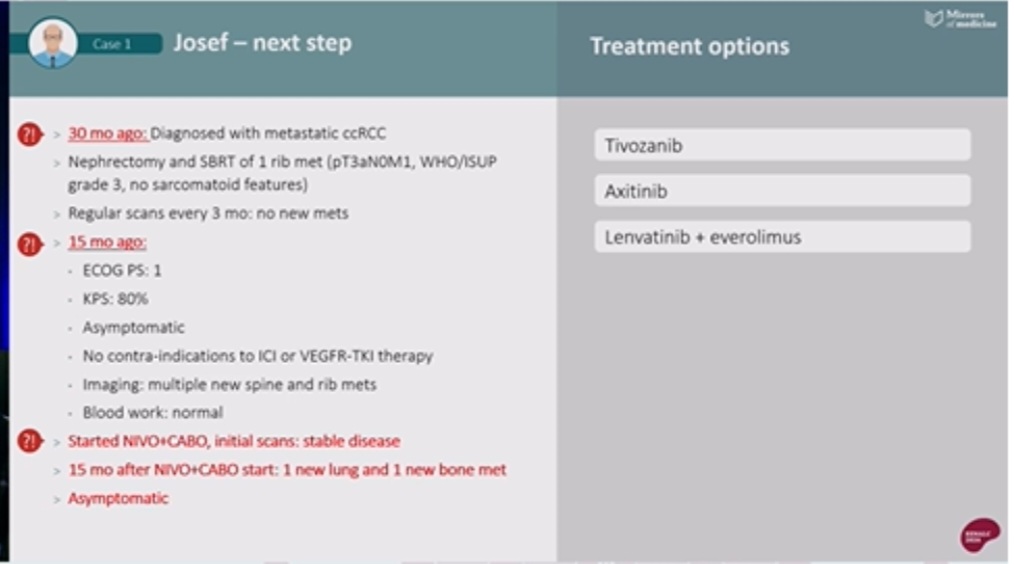
Josef’s case: Choices in metastatic ccRCC after ICI-TKI therapy—balancing risks & benefits.
Treatment pathways include: VEGFR-TKIs, dual ICI regimens, and combination therapies.
Clinical decision-making relies on panel recommendations vs peer opinions—bringing consensus to the forefront!”

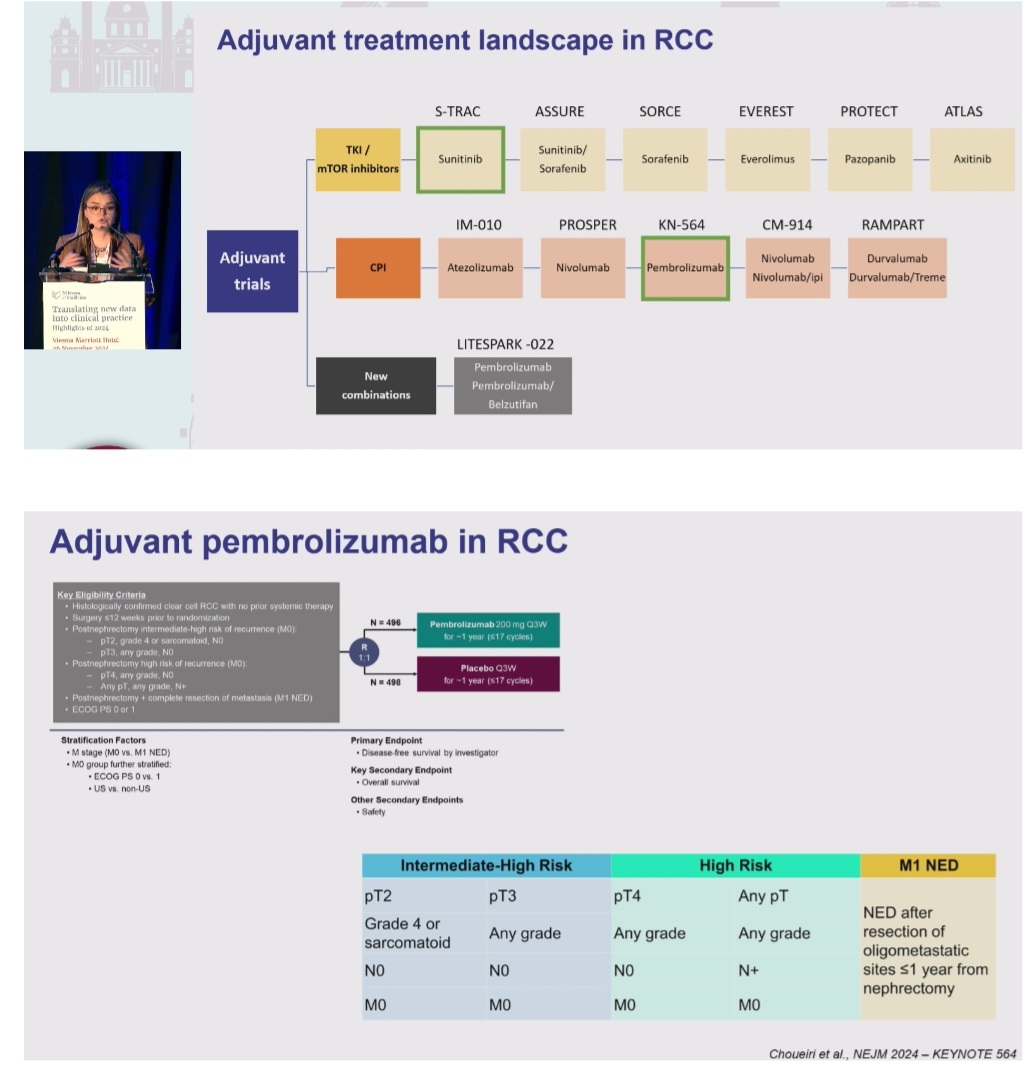
Congress highlights with impact on clinical practice:
“Congress highlights with impact on clinical practice
Moderator: Axel Bex
TKI/mTOR inhibitors: Trials include S-TRAC, ASSURE, SORCE, and more. Mixed outcomes!
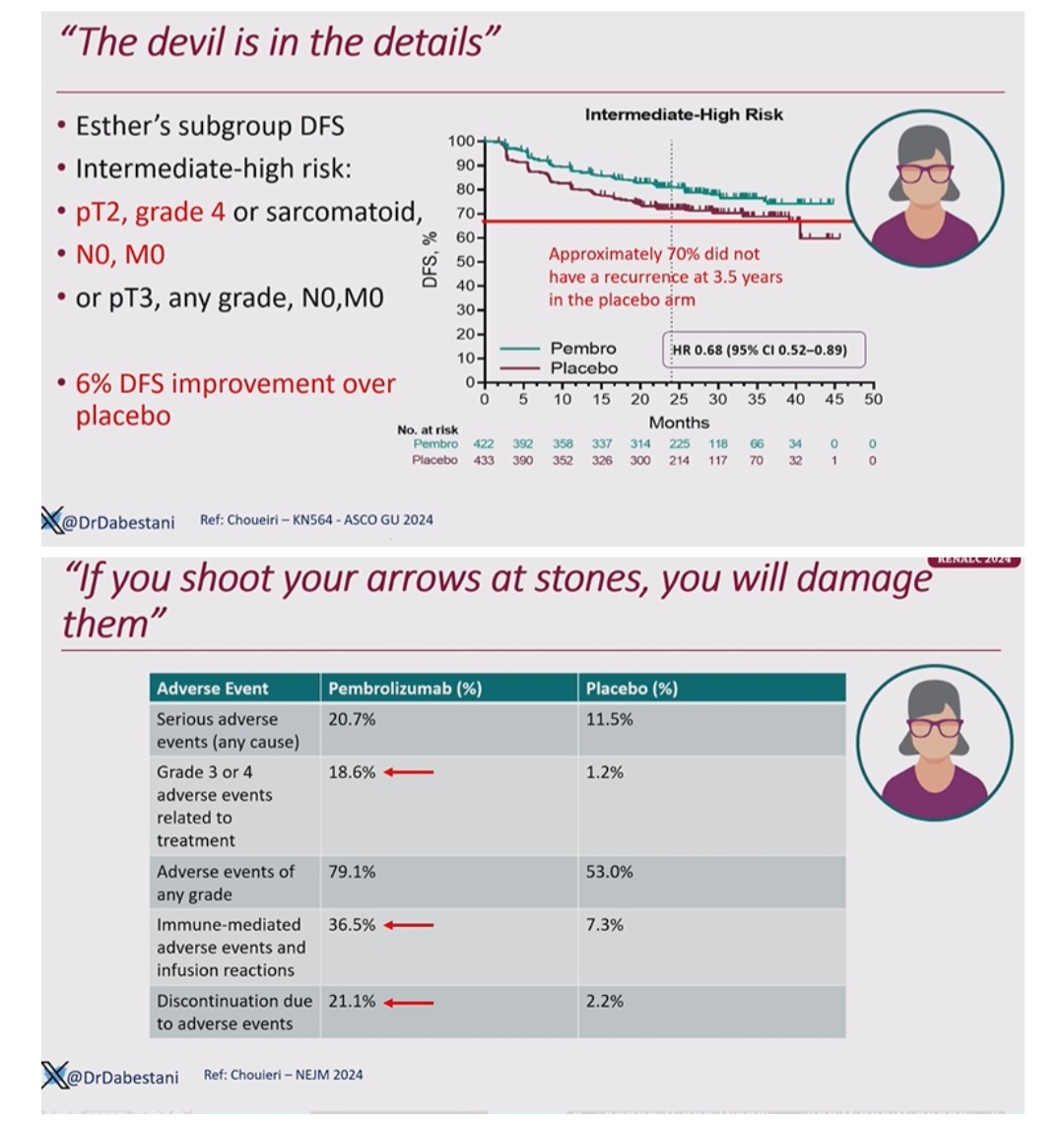
CPI therapies: PROMISING! KN-564 highlighted Pembrolizumab with proven efficacy.
What’s New: Combinations like LITESPARK-022 exploring Belzutifan + Pembrolizumab!
Focus on patient selection & tailored approaches.
Clear-cell RCC with high/intermediate risk of recurrence.
Primary endpoint met: Disease-Free Survival!
Significant OS benefit: HR 0.62, P = .002.
Pembrolizumab redefines adjuvant therapy standards!
Overall Survival in KN-564
– Median follow-up: 57.2 months.
– Pembrolizumab: OS significantly improved vs placebo (HR 0.62).
Takeaway: A GAME-CHANGER for adjuvant RCC therapy!
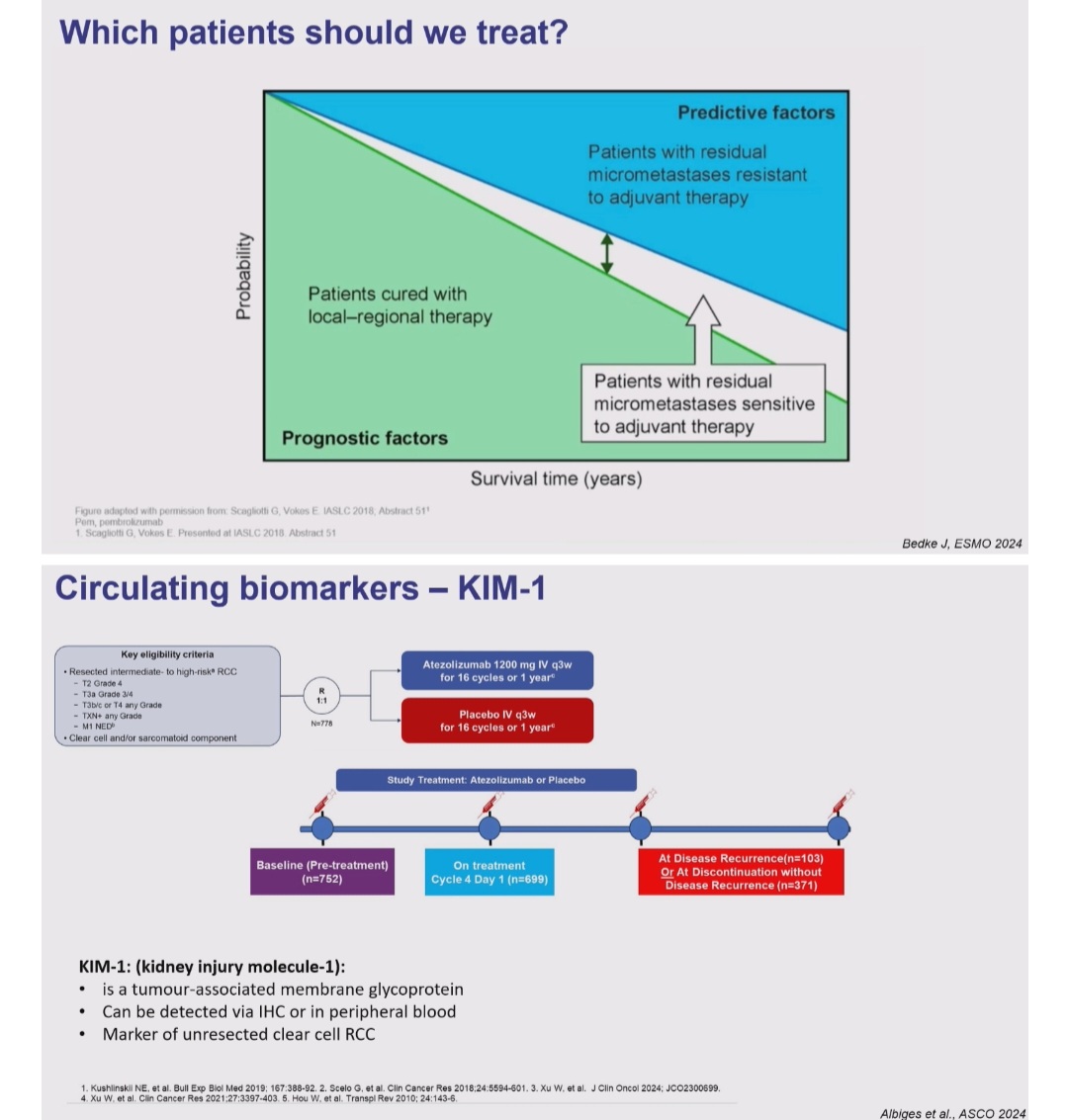
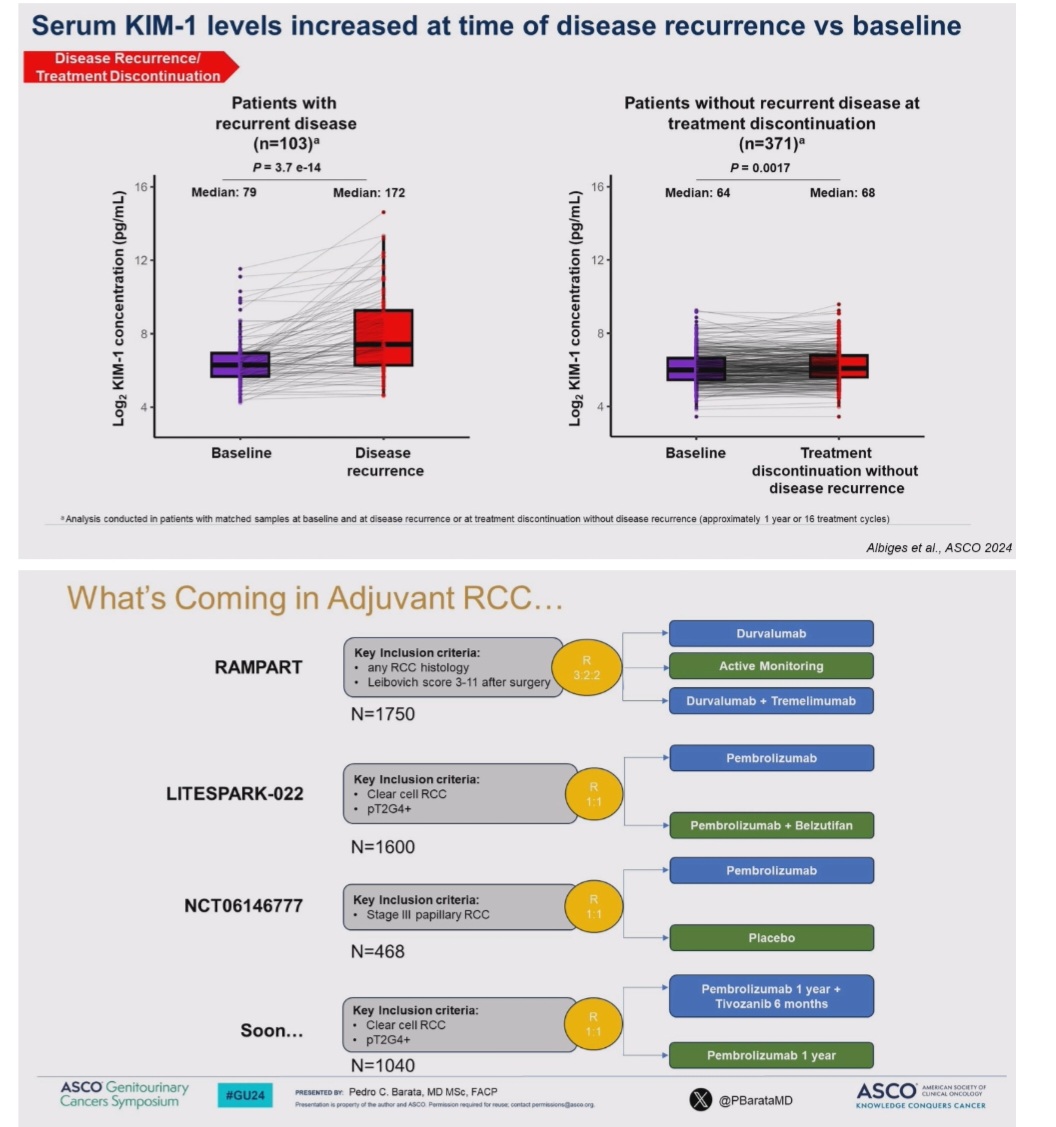
Biomarker KIM-1 (IMmotion010)
– KIM-1: A novel biomarker for RCC progression monitoring.
– Serum levels spiked at recurrence (Median: 172 vs 79 pg/mL).
– Could revolutionize RCC surveillance strategies!
What’s Coming in Adjuvant RCC?
– RAMPART: Durvalumab & Tremelimumab shaping new standards.
– LITESPARK-022: Pembrolizumab + Belzutifan in focus.
Upcoming trials: Novel combinations for better outcomes!”

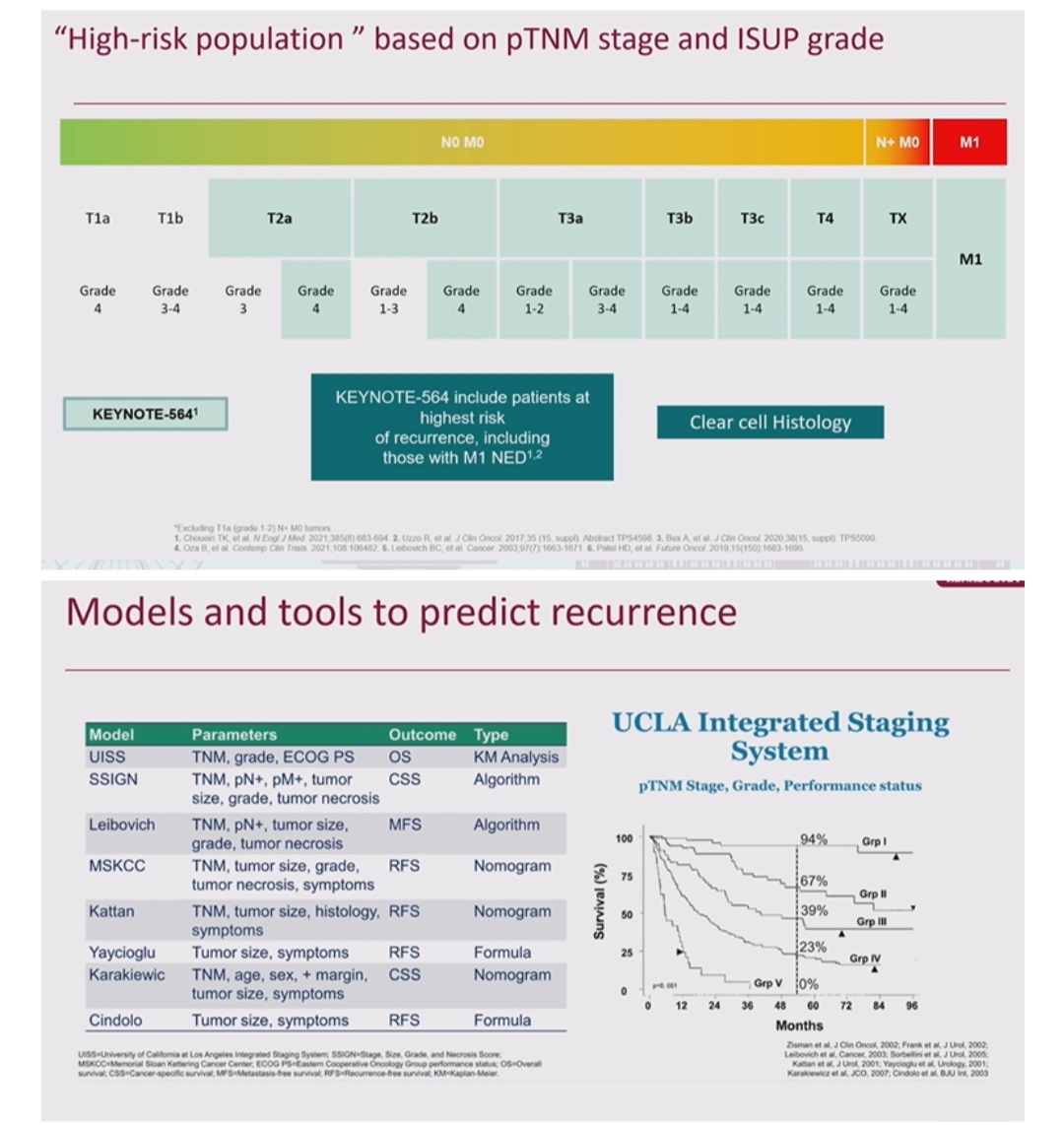
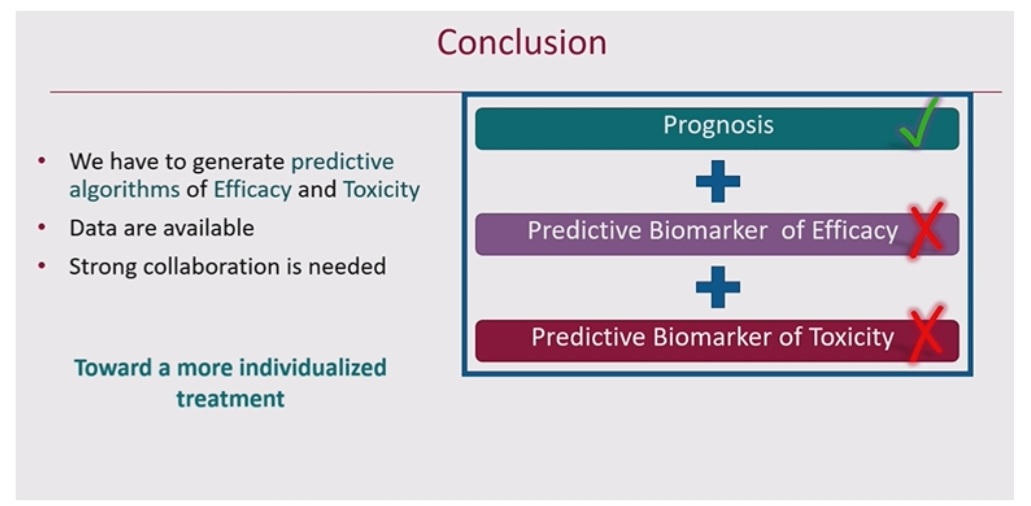
Risk assessment of post-nephrectomy patients:
“Risk assessment of post-nephrectomy patients
Presenter: Philippe Barthélémy
KN564: The ONLY positive trial for adjuvant RCC with significant OS and DFS benefits in clear-cell histology.
Risk Stratification: TNM stage and ISUP grade crucial for identifying high-risk patients eligible for adjuvant therapy.
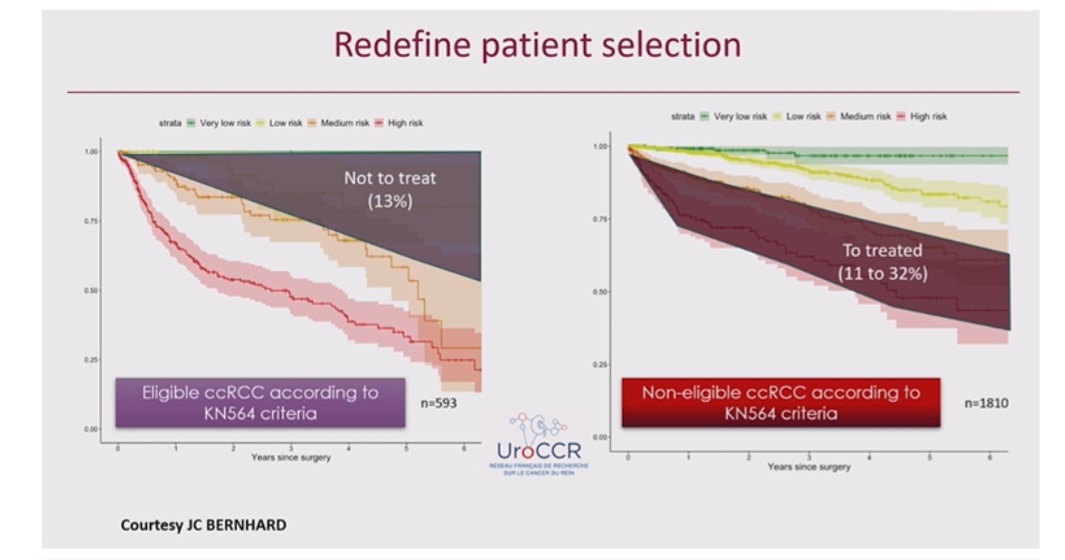
Prediction Models: Current tools (UISS, SSIGN) lack precision; real-world data highlights the need for personalized risk assessment.
UroPredict: Machine learning-based models show potential in refining recurrence risk prediction and patient selection.
Next Steps: Development of predictive biomarkers for efficacy and toxicity to achieve individualized treatments.”

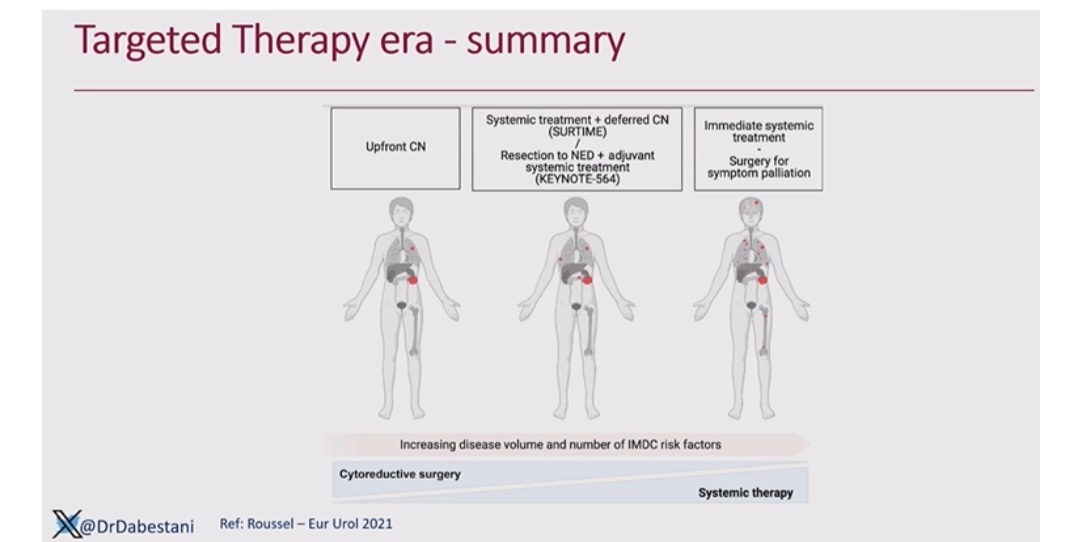
Saeed Dabestani on the history of Cytoreductive nephrectomy:
“Cytoreductive nephrectomy: The history
Presenter: Saeed Dabestani
Congress: RENALC24
2001 EORTC 30947: First RCT showed survival benefit of cytoreductive nephrectomy (CN) + IFN-α over IFN-α alone.
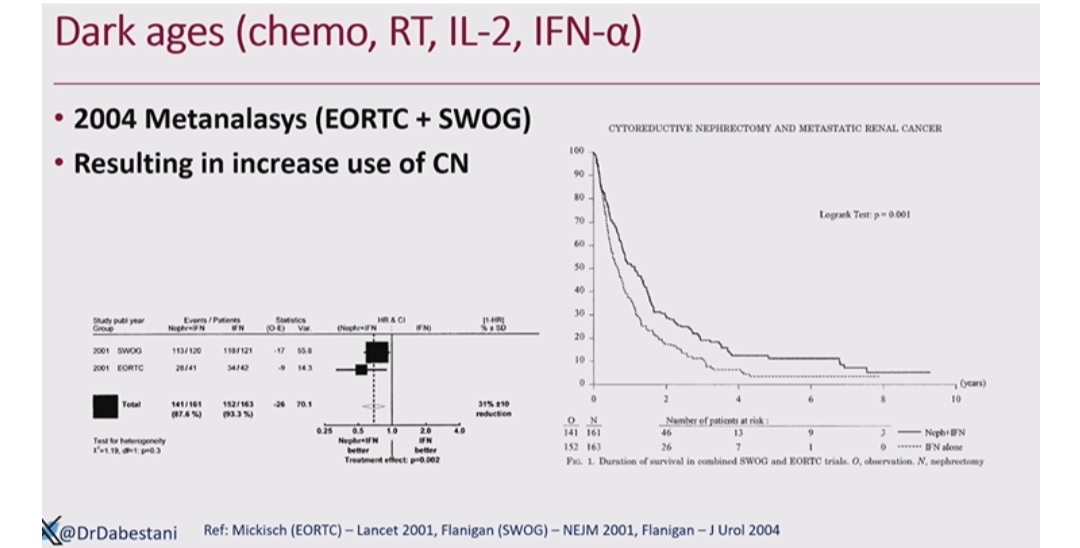
2004 Meta-analysis: Combined SWOG and EORTC data confirmed OS benefits of CN, increasing its use in mRCC management.
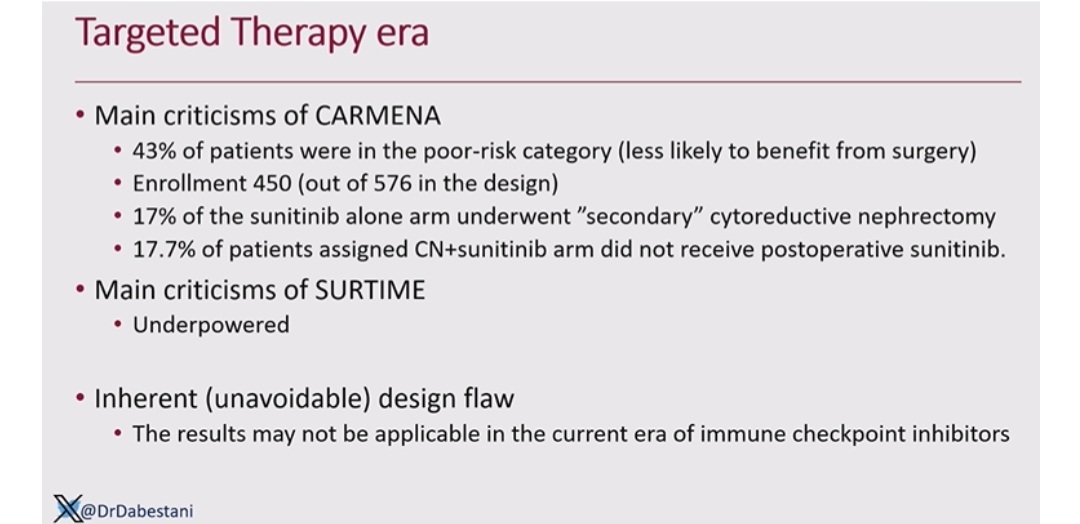
Targeted therapy era: Trials like CARMENA and SURTIME redefined the role of CN alongside systemic therapies like Sunitinib.
Key insights: Deferred CN (SURTIME) offers survival benefit in selected patients, highlighting the importance of patient selection.
Future directions: Integration with immune checkpoint inhibitors requires updated strategies for CN use.”

Weighing the pros and cons of adjuvant therapy:
“Debate: Weighing the pros and cons of adjuvant therapy
Speakers: Saeed Dabestani
KN564: Clear benefits in DFS and OS for high-risk RCC patients with Pembrolizumab.
Adverse events: 36.5% immune-related AEs and 21.1% discontinuation rates highlight toxicity concerns.
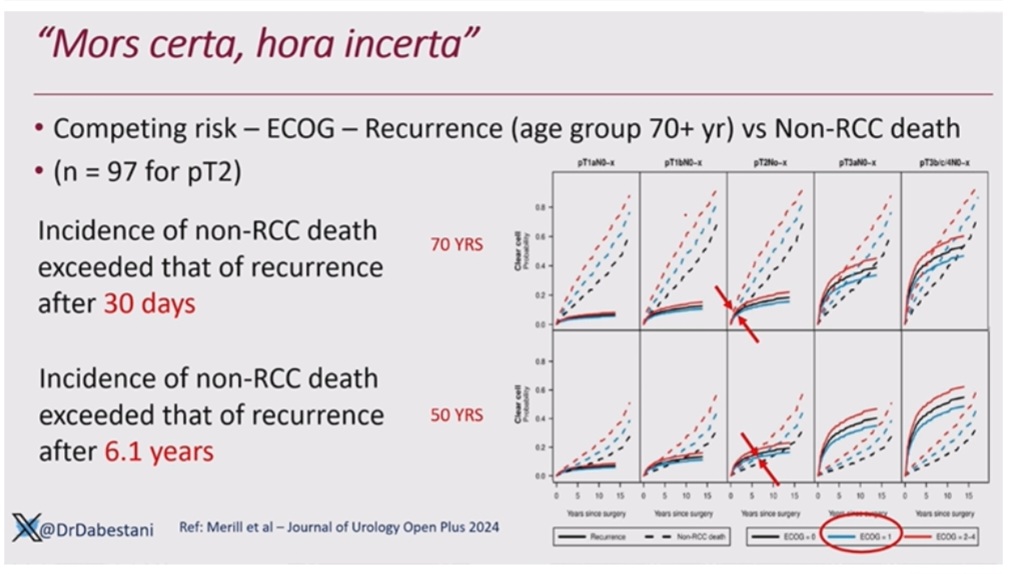
Risk stratification: Precise tools are needed to avoid overtreatment while maximizing outcomes.
Key message: Inform patients about risks and benefits to empower shared decision-making.
Future direction: Integrating biomarkers and AI-driven prediction models for individualized care.”

More posts featuring María Natalia Gandur Quiroga on oncodaily.com
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}