


The randomized phase 3 SENTRY trial evaluated whether adding selinexor to ruxolitinib could improve clinical and molecular outcomes in patients with JAK inhibitor-naïve myelofibrosis. The results were presented by John Mascarenhas, MD, at the 2026 ASCO Annual Meeting.
Clinical Context
Current frontline treatment with ruxolitinib improves splenomegaly and disease-related symptoms, however, depth and durability of spleen response remain limited, with modest direct impact on clonal burden and variant allele frequency.
XPO1-mediated nuclear export is involved in malignant MPN cell survival and has been associated with progressive disease biology and limited OS. Selinexor, an oral selective XPO1 inhibitor, restores tumor suppressor function, promotes apoptosis and reduces malignant clonal burden.
Preclinical MPN models have demonstrated synergistic activity between selinexor and JAK inhibition, supporting the potential of their dual targeting to enhance depth of response and disease control.

Myelofibrosis (MF) in 2026: Matching Therapy to the Dominant Clinical Problem
Study Population and Methods
SENTRY enrolled patients (across 20 countries) with JAK inhibitor-naïve primary or secondary MF who had active symptomatic disease, spleen volume ≥450 cm³, DIPSS intermediate-1 risk or higher, and platelet counts ≥100 ×10⁹/L.
Patients were randomized in a 2:1 ratio in this double-blind study to receive selinexor 60 mg once weekly plus ruxolitinib or placebo plus ruxolitinib, with stratification according to DIPSS risk category, baseline spleen volume, and platelet count.
The co-primary endpoints were:
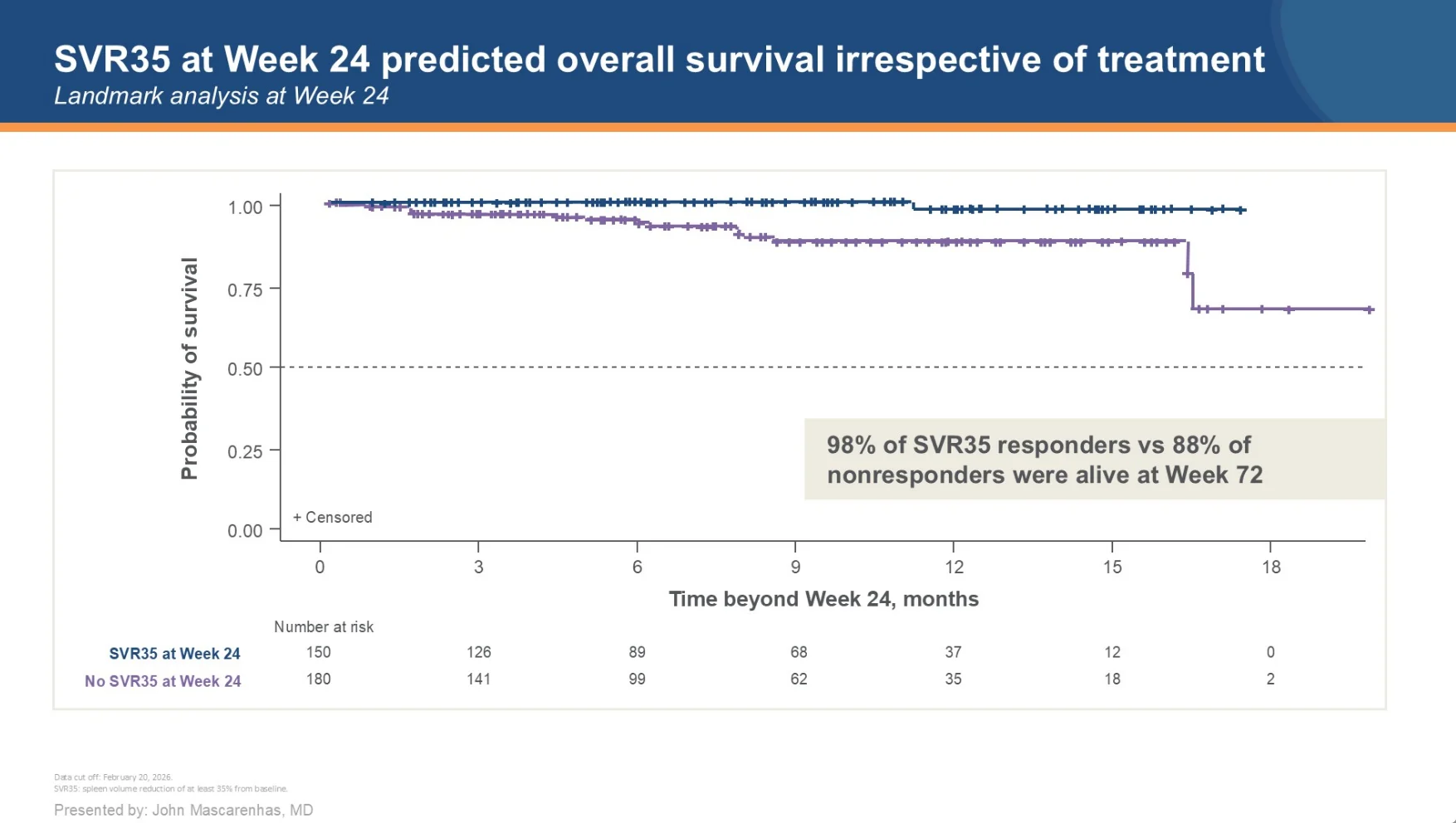
- Spleen volume reduction ≥35% (SVR35) at Week 24
- Absolute mean change in total symptom score (AbsTSS), excluding fatigue, at Week 24
SVR35 was assessed using a stratified Cochran-Mantel-Haenszel test, while symptom outcomes were analyzed using a mixed-effects repeated measures model. Secondary endpoints included safety and OS. Reduction in driver mutation VAF was assessed as an exploratory endpoint.
Efficacy and Safety
A total of 353 patients were randomized to S+R (n=235) or ruxolitinib alone (n=118). Baseline characteristics were generally balanced between treatment arms.
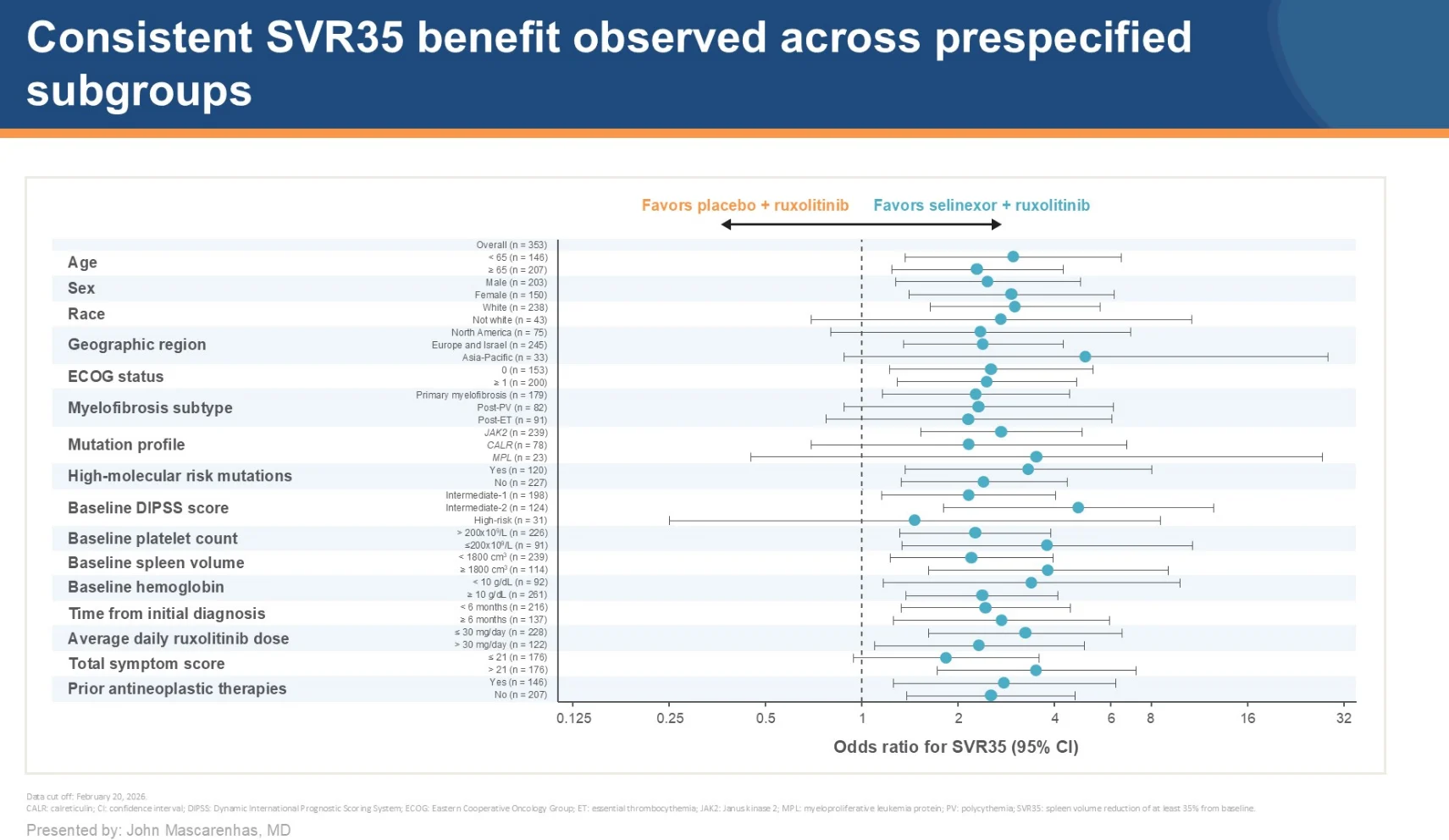
The trial met its primary spleen response endpoint. At Week 24, SVR35 was achieved in 49.8% of patients receiving S+R compared with 28.0% in the ruxolitinib-alone arm, corresponding to an absolute difference of 21.8% (OR 2.58; 95% CI 1.60-4.17; P < .0001).

The mean percentage reduction in spleen volume at Week 24 was −40.0% with S+R vs −26.7%. Notably, spleen responses emerged early and remained durable over time. At any time during treatment, SVR35 was achieved in 67.7% of patients vs 44.9% receiving ruxolitinib alone. Importantly, the benefit was consistent across prespecified subgroups.
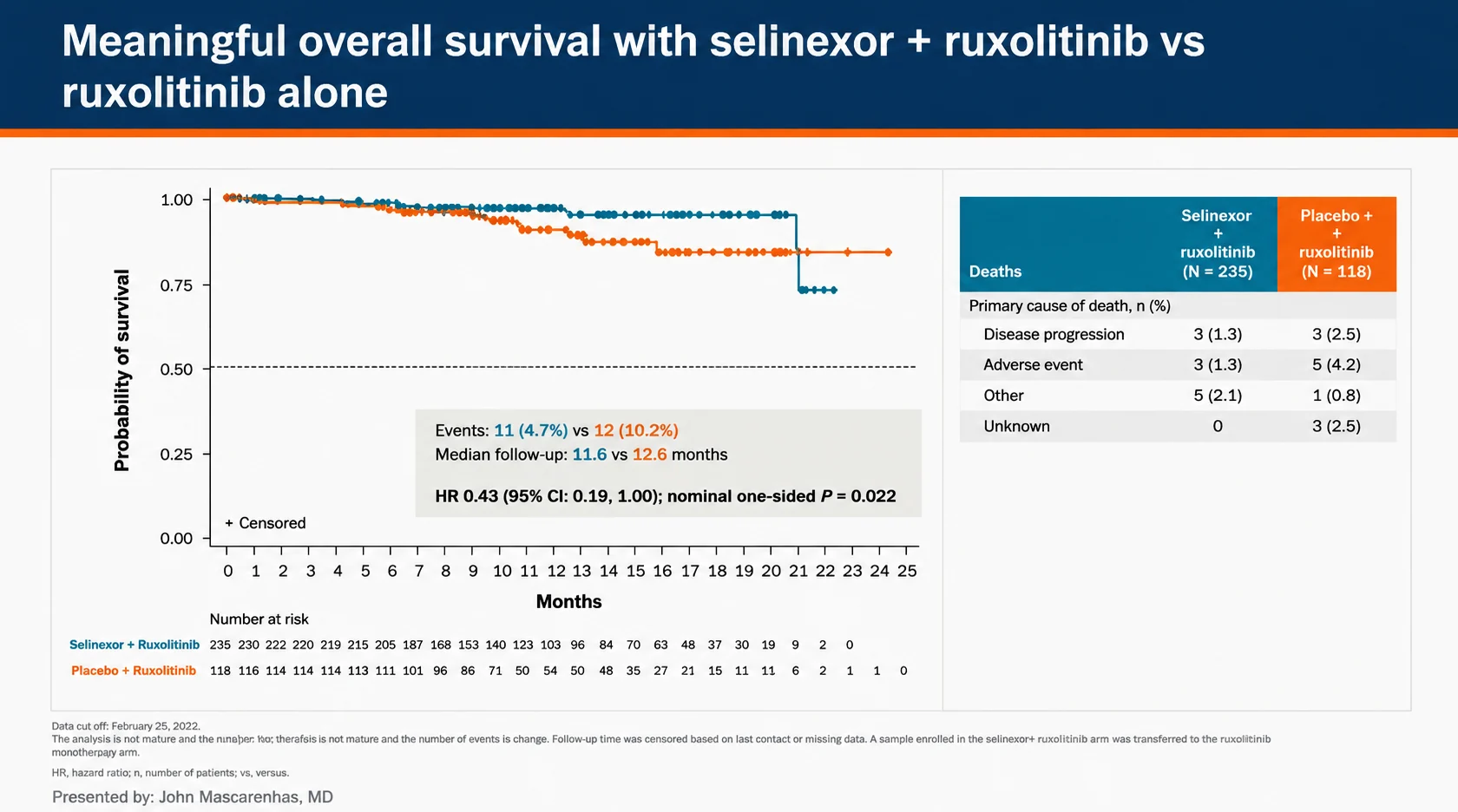
Symptom improvement was comparable between treatment groups. Mean AbsTSS change at Week 24 was −9.9 in the S+R arm and −10.9 in the control arm. An early OS signal favoring S+R was observed, with a lower estimated risk of death compared with ruxolitinib alone (HR 0.43).

VAF reduction ≥20% at Week 24 occurred in 32.0% of patients receiving S+R vs 23.9%, and correlated with SVR35 response.
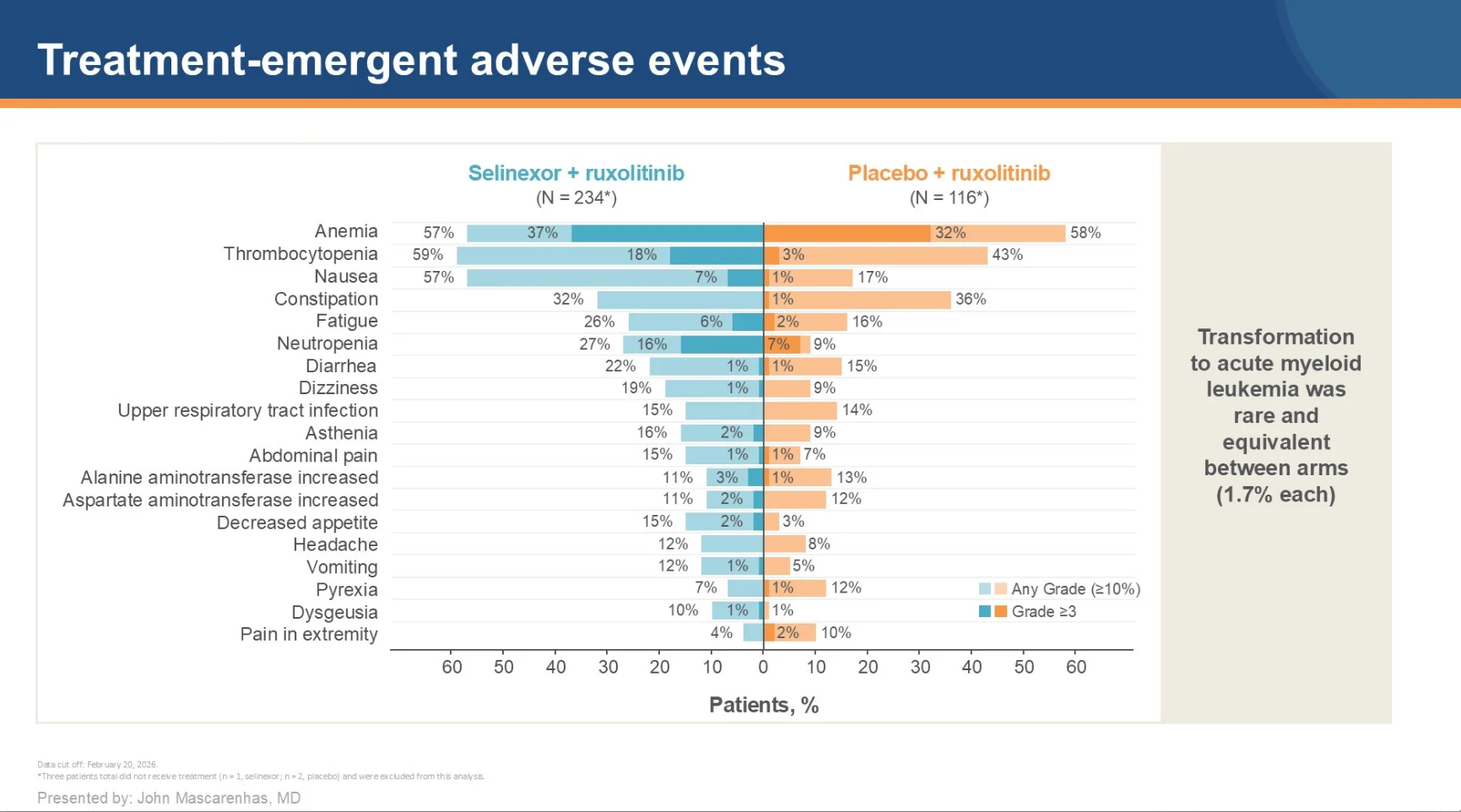
Grade ≥3 TEAEs with S+R occurred in 70.1% vs 50.0% of patients, while discontinuation rates remained relatively low (14.5% vs 8.6%). TEAEs leading to death occurred in 0.9% vs 2.6%, and leukemic transformation rates were identical in both arms (1.7%).
Contextualizing the Findings
The phase 3 SENTRY reinforces the emerging concept that dual targeting may improve depth of spleen responses in MF. It also highlights the ongoing challenge of demonstrating clear superiority over ruxolitinib with respect to symptom control, as absolute mean change in TSS at Week 24 was comparable between treatment groups.
This pattern closely mirrors findings observed with prior frontline combination approaches in MF, particularly pelabresib in MANIFEST-2 and navitoclax in TRANSFORM-1. Both studies demonstrated improved spleen responses when added to ruxolitinib, while improvements in symptom burden were either modest or less clearly differentiated from ruxolitinib monotherapy.
It is also important to note that, for patients proceeding to allogeneic transplantation, the rapid spleen volume reduction observed with S+R may help spare patients from conventional spleen-directed modalities. This adds to the growing rationale for incorporating such endpoints into future MF clinical trials.

Take-Home Messages
The SENTRY trial demonstrated that S+R produced significantly higher spleen response rates compared with ruxolitinib alone. The combination demonstrated earlier, deeper, and more sustained spleen reductions, with exploratory evidence of improved molecular responses supporting the possibility of biologic activity.
Toxicities were increased with S+R but treatment discontinuation and treatment-related mortality rates were relatively low, indicating that the regimen may be clinically manageable.
Although symptom improvement was comparable between groups, the findings support selinexor plus ruxolitinib as a novel treatment strategy in MF and merit further long-term evaluation of survival outcomes, durable disease modification, and tolerability.
{kind=link}
{kind=link}
{kind=link}
{kind=link}