


A common treatment sequence in chronic lymphocytic leukemia involves frontline covalent BTK inhibitor followed by fixed-duration venetoclax-rituximab (VR) at relapse, though prospective data supporting this sequence are limited.
Pirtobrutinib, a highly selective non-covalent BTKi with activity in both wild-type and C481-mutated BTK, has expanded options for patients previously treated with cBTKis.
Early studies of fixed-duration pirtobrutinib-venetoclax-rituximab (PVR) showed encouraging efficacy and tolerability, leading to the phase 3 BRUIN CLL-322 trial, results of which were presented by Matthew Davids during the Late-Breaking Abstract session at EHA 2026.
Methods
This global, multicenter, open-label phase 3 study enrolled patients across 22 countries. Eligible patients had R/R CLL/SLL requiring treatment according to iwCLL 2018 criteria and had received at least one prior line of therapy.
Prior cBTKi exposure was permitted, while prior non-covalent BTKi or BCL2 inhibitor exposure was not. Patients were randomized 1:1 to fixed-duration PVR or VR. Randomization was stratified by del(17p) status and prior cBTKi exposure.
The PVR arm received pirtobrutinib for 28 cycles, including a 3-cycle pirtobrutinib-rituximab lead-in before venetoclax initiation. Both groups received venetoclax for 25 cycles and rituximab for 6 cycles.
The primary endpoint was independent review committee-assessed PFS. Secondary endpoints included OS, investigator-assessed PFS, time to next treatment, ORR, and safety. MRD was assessed as an exploratory endpoint.
Study Population
A total of 639 patients were randomized (PVR:321, VR:318). The study population was representative of contemporary R/R CLL, with a median age of 68 years and a median of two prior lines of therapy.
Approximately 80% of patients had received a prior covalent BTK inhibitor, and more than half had discontinued BTKi therapy because of progressive disease.
High-risk disease features were common, including unmutated IGHV, complex karyotype, and TP53 aberrations. Baseline characteristics were balanced between treatment groups.
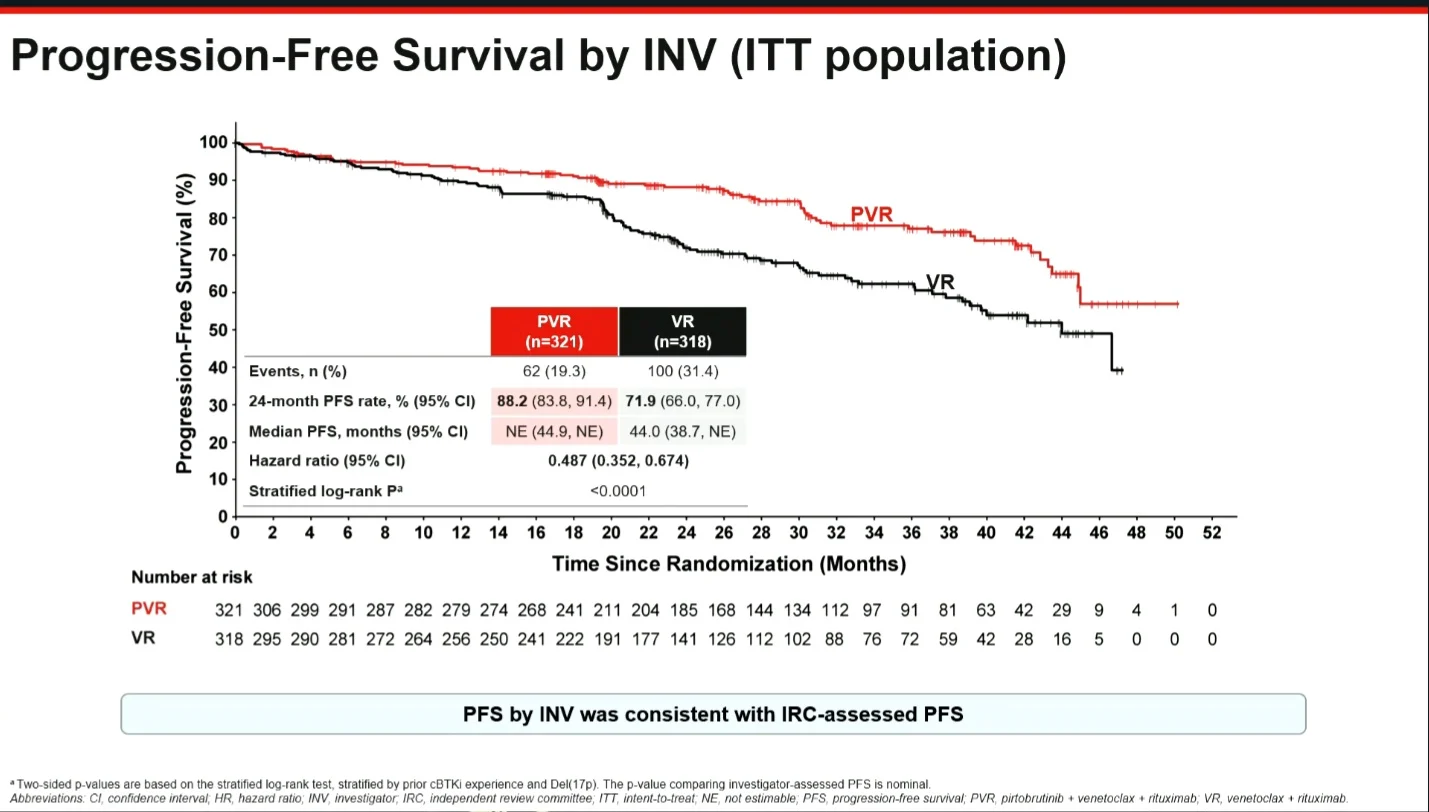
Progression-Free Survival
The primary endpoint was met. At a median follow-up of 27.3 months, PVR significantly improved IRC-assessed PFS compared with VR.
The risk of progression or death was reduced by approximately 45% (HR 0.547, P=0.0001). The 24-month PFS rate was 86.9% with PVR vs 71.8% with VR. Median PFS was not reached with PVR and was 39.7 months with VR. Investigator-assessed analyses showed similar results.

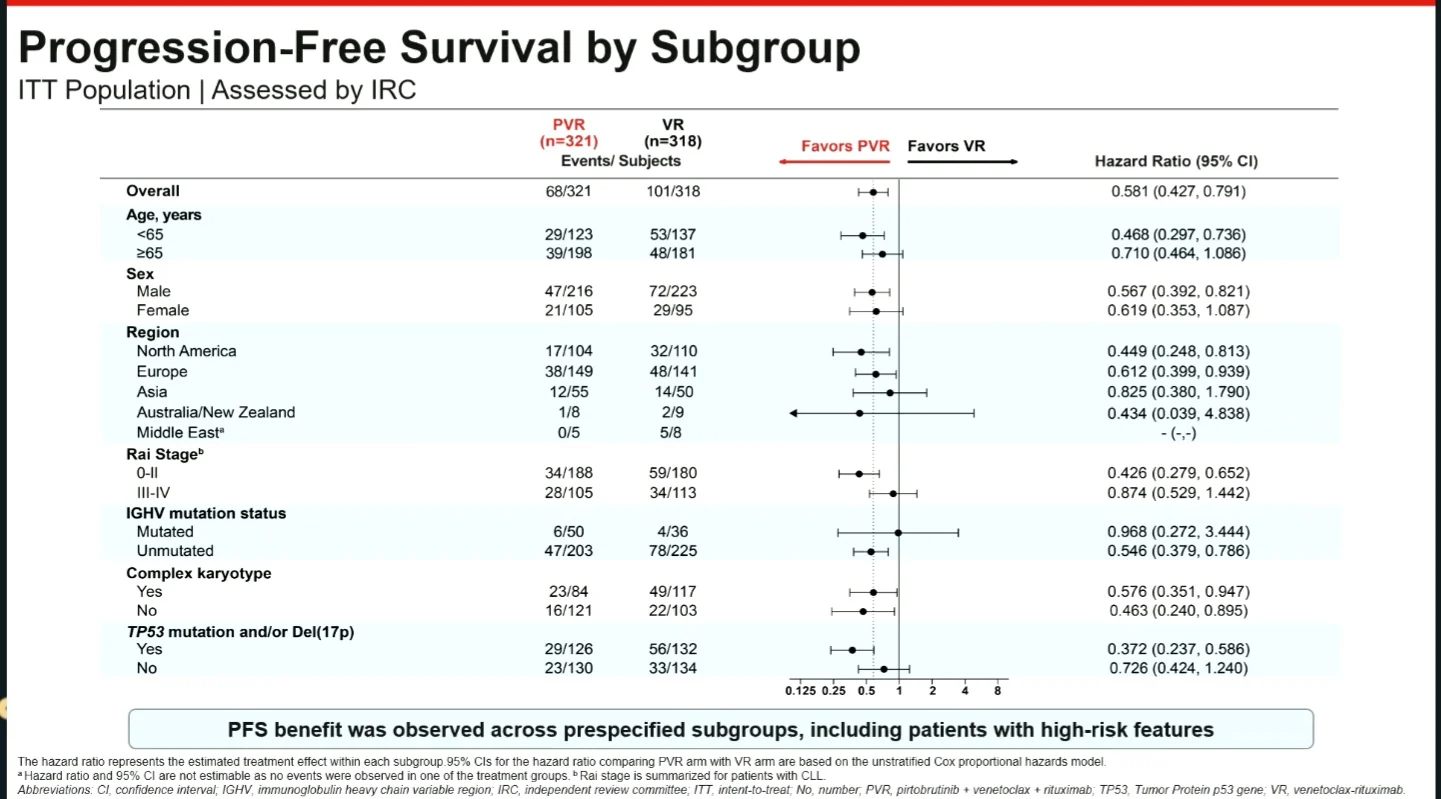
PFS Across Subgroups
The PFS benefit was observed across prespecified subgroups, including with unmutated IGHV, complex karyotype, and TP53 aberrations.
Among patients previously treated with a covalent BTKi, PVR continued to outperform VR, including in those who discontinued prior BTKi therapy because of disease progression.
The greatest separation between treatment arms was observed among patients whose only prior therapy was a covalent BTK inhibitor and who subsequently progressed. In this subgroup, the 24-month PFS rate was 88.4% with PVR versus 51.6% with VR.

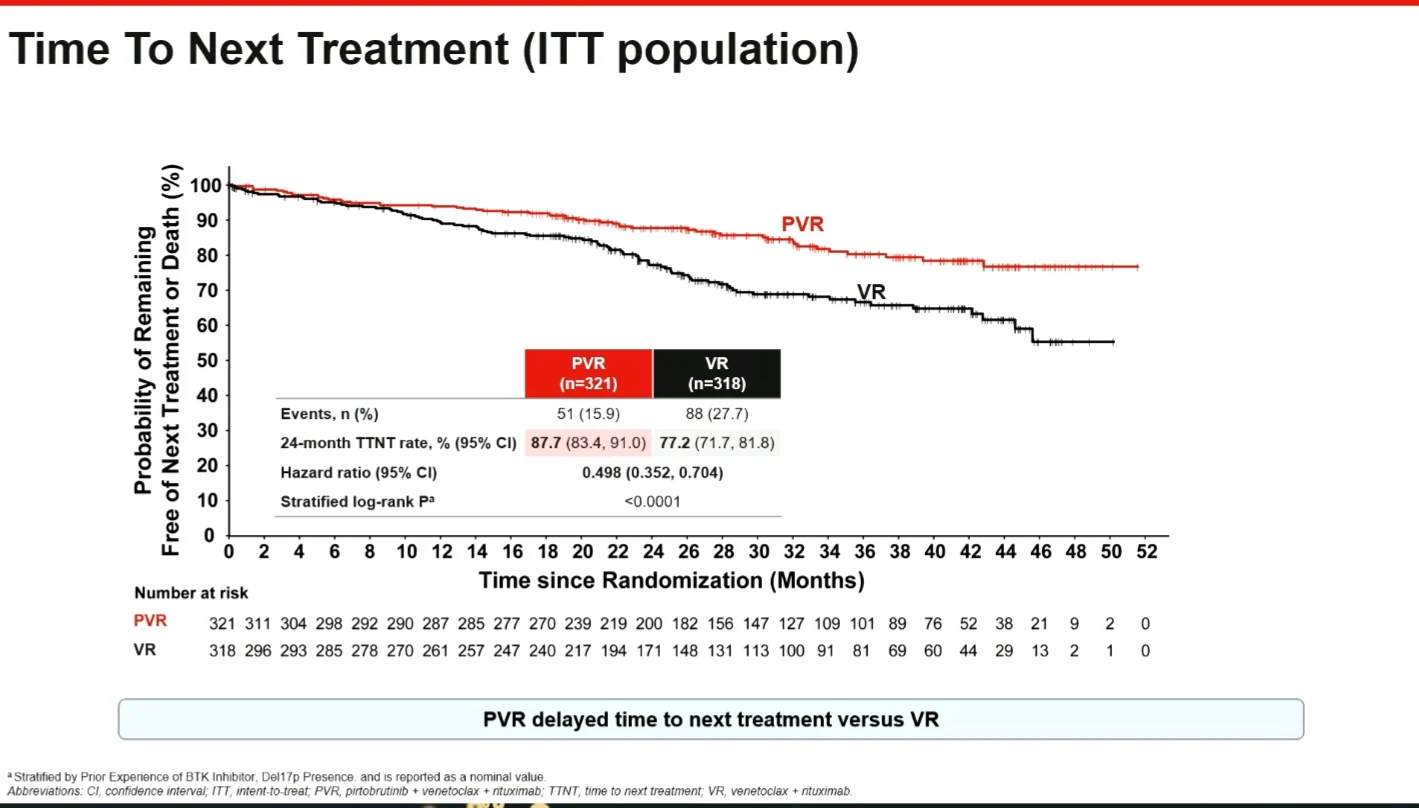
Time to Next Treatment
PVR significantly delayed the need for subsequent therapy. The risk of requiring next treatment or death was reduced by approximately 50% (HR 0.498). At 24 months, 87.7% of patients receiving PVR remained free from subsequent therapy or death vs 77.2% receiving VR.
Depth of Response and Survival
Overall response rates were high in both groups. ORR was 88.5% with PVR and 83.3% with VR. Deeper responses were observed with the triplet regimen, with complete responses achieved in 31.8% of patients receiving PVR vs 23.3% receiving VR.
This translated into higher rates of MRD negativity. Among patients with evaluable end-of-treatment samples, uMRD4 was achieved in 86.3% of patients treated with PVR vs 60.7% treated with VR. Higher rates of deeper MRD responses were also observed with PVR.
Overall survival data remain immature. At the time of analysis, the 24-month OS rate exceeded 89% in both treatment groups, and no statistically significant difference in OS had emerged. The impact of PVR on OS remains to be determined.

Safety
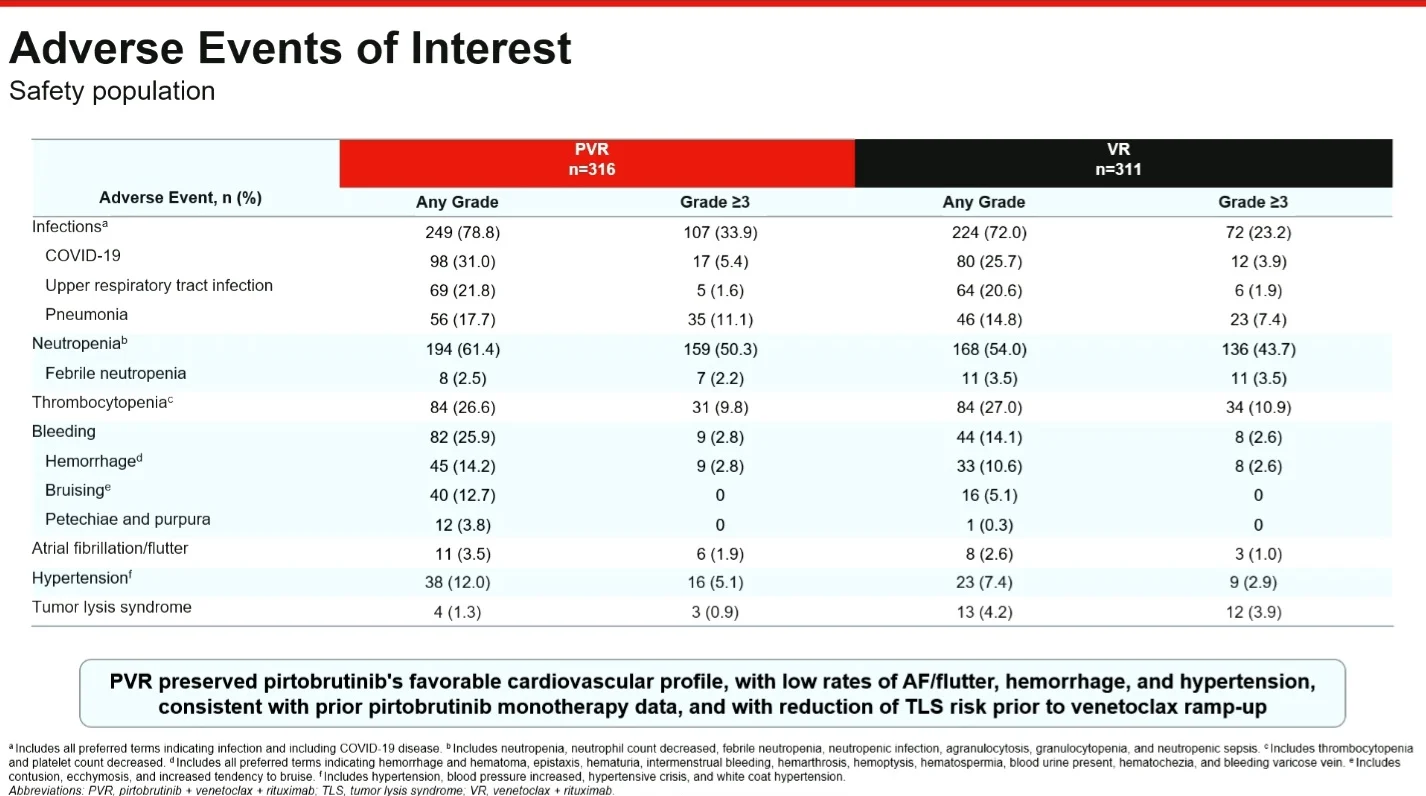
The overall safety profile of PVR was generally similar to that of VR. Grade ≥3 adverse events occurred in 78.8% of patients receiving PVR and 73.0% receiving VR. Treatment discontinuation due to treatment-related adverse events was uncommon and comparable between groups.
Neutropenia was the most common grade ≥3 adverse event in both arms. Infections were frequent but generally manageable, with low rates of febrile neutropenia.
Rates of atrial fibrillation/flutter, hypertension, and clinically significant hemorrhage were low and consistent with previous pirtobrutinib experience. Tumor lysis syndrome occurred less frequently with PVR than with VR, potentially reflecting the pirtobrutinib lead-in before venetoclax initiation.
Bottom Line
BRUIN CLL-322 provides the first phase 3 evidence supporting the addition of a non-covalent BTKi to a fixed-duration venetoclax-based regimen in relapsed/refractory CLL. PVR improved disease control, deepened responses, and prolonged treatment-free intervals compared with VR, with benefits observed across clinically important patient subgroups. These efficacy gains were achieved without new safety signals supporting fixed-duration PVR as a potential new SOC for R/R CLL.

{kind=link}
{kind=link}
{kind=link}
{kind=link}