


Updated results from inMMyCAR, the ongoing first-in-human phase 1 study of an investigational in vivo BCMA-directed CAR-T therapy in RRMM, were presented during a Rapid Oral Session at ASCO 2026 by P. Joy Ho, PhD, MBBS.
The Rise of inMMyCAR
The rationale for in vivo CAR-T development lies in overcoming several major limitations of conventional ex vivo CAR-T manufacturing, including high production costs, complex logistics, treatment delays and the need for lymphodepleting chemotherapy.
By enabling direct in vivo generation of CAR-T cells through lentiviral gene delivery, this strategy aims to simplify treatment administration while potentially preserving T-cell fitness by avoiding ex vivo culture.
KLN-1010 is a modified lentiviral vector-based platform designed to generate anti-BCMA CAR-T cells in vivo through targeted T-cell transduction, including detargeted fusogen modifications and T-cell retargeting molecules to enhance CD3-directed tropism.
The CAR construct incorporates a proprietary fully human BCMA scFv linked to 4-1BB and CD3ζ signaling domains. Overall, this approach may broaden access to CAR-T therapy by reducing manufacturing complexity and improving scalability for patients with RRMM.

Patient Eligibility and Study Design
The study employs a dose-escalation 3+3 design with backfill cohorts for dose optimization, followed by expansion cohorts at the recommended phase 2 dose. Eligible patients had received at least 3 prior lines of therapy, including a PI, IMiD, and anti-CD38 monoclonal antibody, with ECOG performance status 0-1 and adequate bone marrow and end-organ function.
The primary endpoints included safety, tolerability, and RP2D determination, while secondary endpoints assessed CAR T-cell expansion and persistence, ORR, MRD, DOR, and PFS. Patients were enrolled across study sites in Australia and the United States.
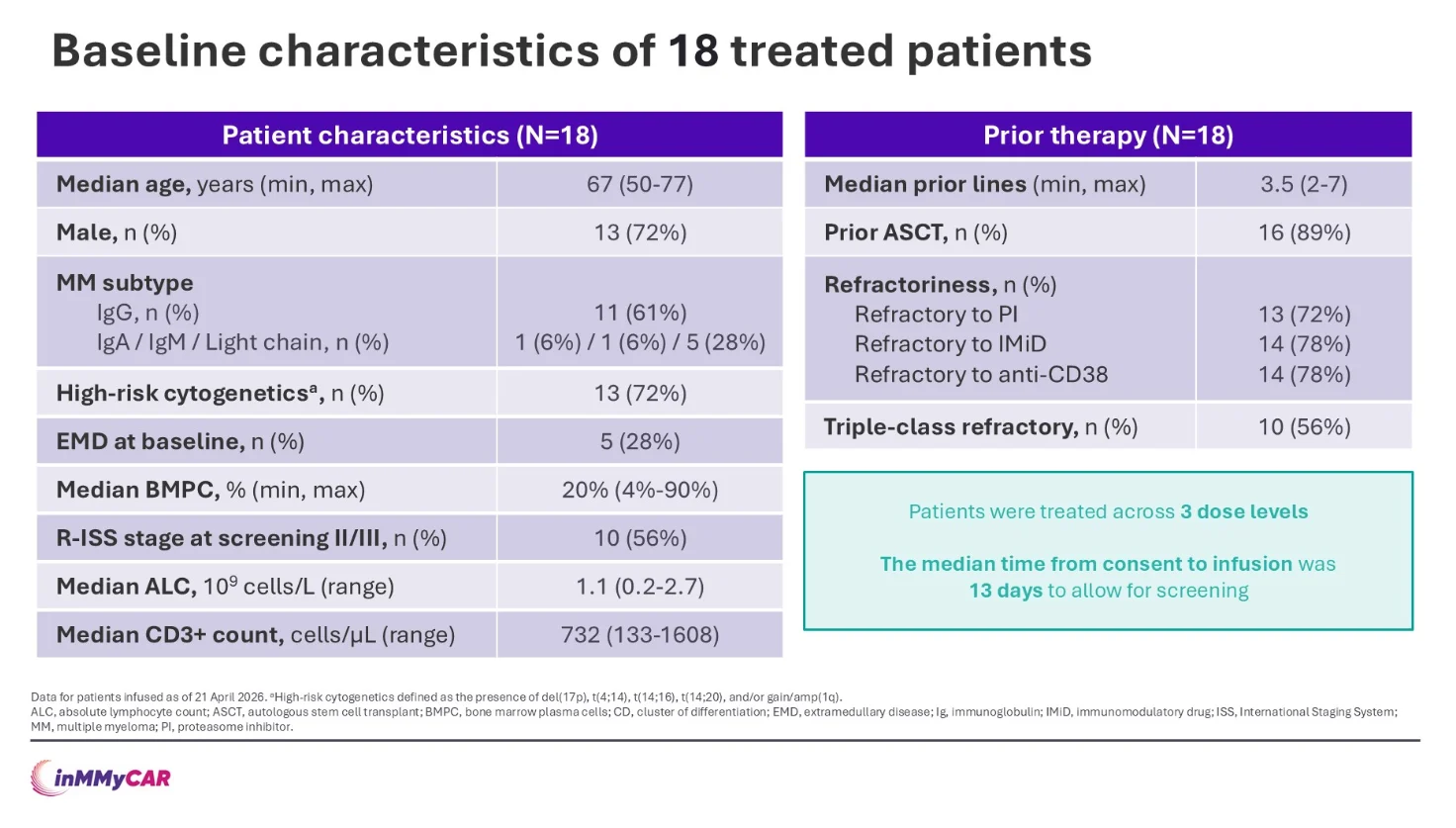
At the time of analysis, 18 patients had been treated across 3 dose levels. Patients were previously treated, with a median of 3.5 prior lines of therapy, and more than half were triple-class refractory. Most patients had previously undergone ASCT.
High-risk cytogenetics were present in the majority, and a subset had extramedullary disease at baseline. The median age was 67 years, and the median time from consent to infusion was 13 days to allow for screening.
Early Outcomes in Focus
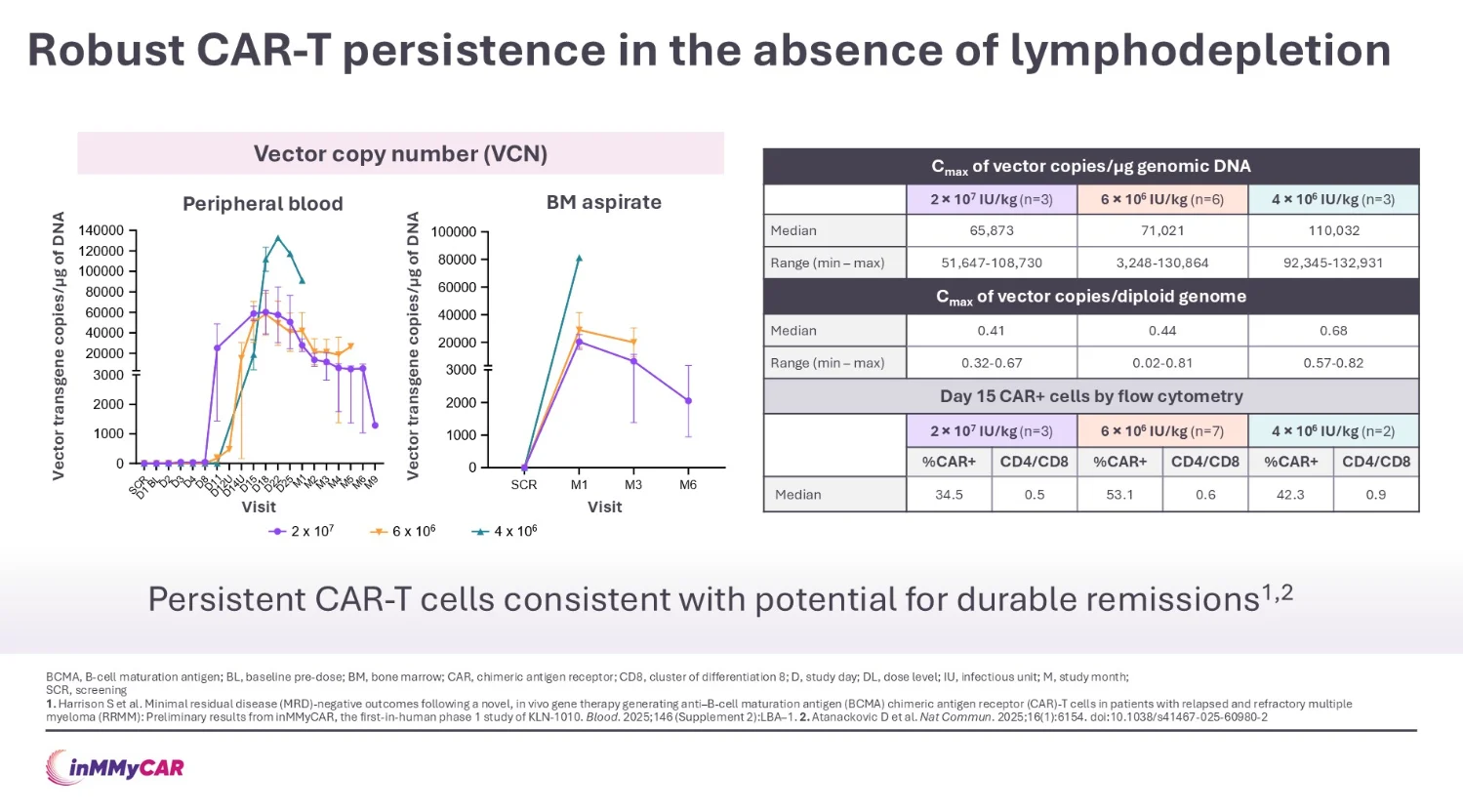
Peak lymphocyte expansion was observed between days 13 and 22, with CAR-T cells remaining detectable in peripheral blood throughout follow-up. Notably, CAR-T persistence was achieved without lymphodepleting chemotherapy, supporting sustained in vivo CAR-T generation following KLN-1010 infusion.

Clinical responses were observed across all treated patients and deepened over time. Among patients with at least 4 months of follow-up, all achieved an objective response, including complete and stringent CR.
Bone marrow MRD negativity was observed in all evaluable patients, mostly at a sensitivity of 10⁻⁶, with ongoing responses seen with longer follow-up. Best IMWG responses included stringent CR, VGPR, and PR. Notably, a patient with extramedullary disease achieved complete radiologic resolution by month 1.

Safety Observations
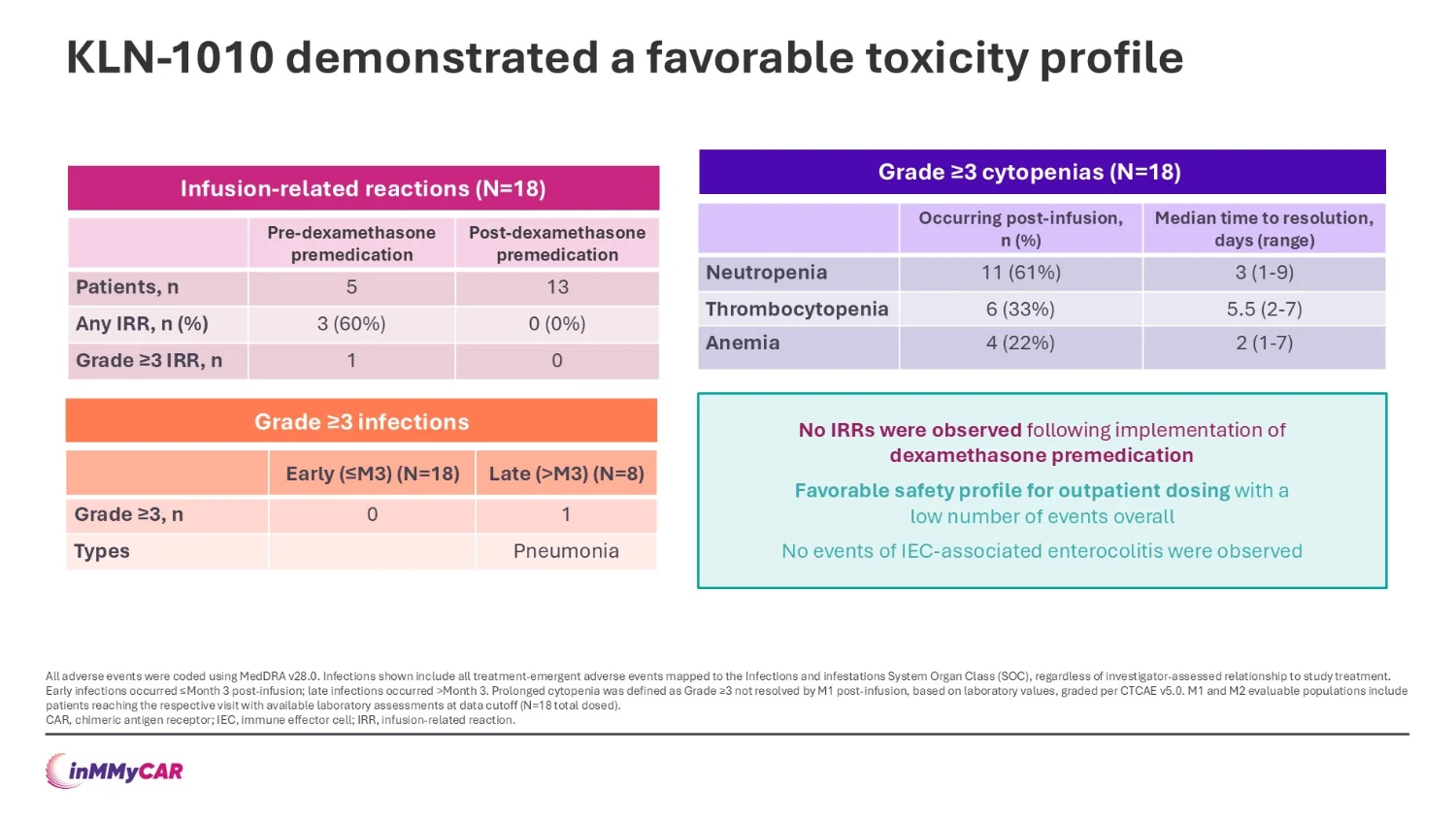
Treatment-emergent adverse events were generally manageable, supporting the feasibility of outpatient dosing. Following dexamethasone premedication, no further infusion-related reactions were observed.
CRS events were consistent with those seen with ex vivo CAR-T therapies and showed a relatively later onset. All CRS events were grade 1-2 and manageable with standard supportive care. One grade 3 ICANS event was successfully managed with methylprednisolone and anakinra, resolving within 3 days. No delayed neurotoxicity was observed.

Outlook
Updated findings from the inMMyCAR study appear favourable in this clinically fit RRMM population. KLN-1010 demonstrated a manageable safety profile without the need for lymphodepletion.
A clinically relevant observation was the short median interval from consent to infusion, reflecting a more streamlined approach.
Although follow-up remains limited and the cohort size is relatively small, the findings support the concept of in vivo CAR-T therapy as a more accessible and outpatient-friendly strategy in RRMM.
You Can Watch More on OncoDaily TV.
{kind=link}
{kind=link}
{kind=link}