


The story of AML over the last decade has largely been one of expanding molecularly targeted therapies and the establishment of venetoclax-based regimens in frontline treatment for older and unfit patients.
VIALE-A positioned azacitidine-venetoclax as the backbone of therapy in this setting, while AGILE demonstrated that outcomes could be improved further with ivosidenib plus azacitidine in patients with IDH1-mutated AML. Subsequently, the Paradigm trial raised an even broader question by suggesting that azacitidine-venetoclax may rival intensive chemotherapy in selected patients.
These studies have shifted attention toward how targeted therapies can be incorporated into established treatment paradigms. The goal is straightforward: deepen remissions, increase rates of MRD negativity, and prolong survival without compromising tolerability.
At the 2026 ASCO Annual Meeting, investigators from The University of Texas MD Anderson Cancer Center presented two studies that address this concept by evaluating the addition of mutation-specific targeted agents to HMA-venetoclax in molecularly defined AML subsets.

Acute Myeloid Leukemia (AML) in 2026: The Current Landscape and Future Perspectives
A Multicenter Phase Ib/II Trial of Azacitidine, Venetoclax, and Ivosidenib in IDH1-Mutated AML
IDH1 mutations occur in approximately 7-8% of newly diagnosed AML cases and contribute to leukemogenesis through production of the oncometabolite 2-hydroxyglutarate, resulting in epigenetic dysregulation and blockade of myeloid differentiation. Therapeutic targeting of mutant IDH1 with ivosidenib has become an established treatment approach in this molecular subgroup.
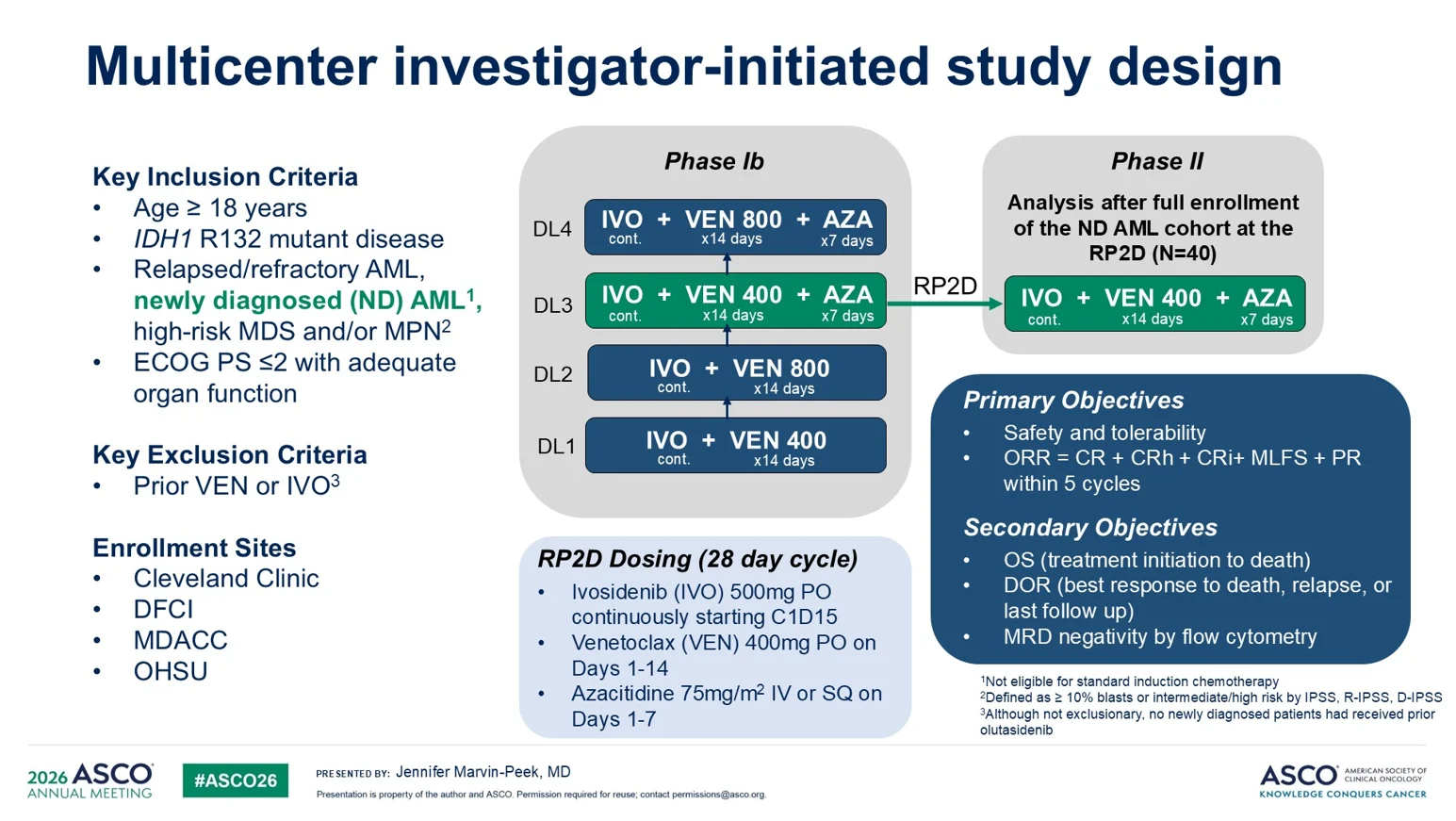
Presented by first author Jennifer Marvin-Peek, MD, this investigator-initiated multicenter phase Ib/II trial (NCT03471260) enrolled patients with newly diagnosed IDH1-mutated AML who were ineligible for intensive induction chemotherapy and had an ECOG performance status ≤2 and adequate organ function. Key exclusion criteria were prior exposure to venetoclax or ivosidenib.
The study was conducted across four U.S. academic centers: Cleveland Clinic, Dana-Farber Cancer Institute, The University of Texas MD Anderson Cancer Center, and Oregon Health & Science University.
Study Design
The phase Ib evaluated escalating combinations of venetoclax and azacitidine with continuous ivosidenib to establish the RP2D, followed by a phase II expansion cohort using the RP2D. The analysis included those treated at the recommended phase II dose.
Primary objectives
- Safety and tolerability.
- Overall response rate (ORR), defined as CR + CRh + CRi + MLFS + PR within five cycles.
Secondary objectives: OS, DOR, MRD negativity by flow cytometry.
Therapy consisted of:
- Azacitidine 75 mg/m² on days 1-7
- Venetoclax 400 mg on days 1-14
- Ivosidenib 500 mg daily beginning on cycle 1 day 15
Dose modifications during remission were permitted to reduce prolonged myelosuppression.
A total of 40 patients were enrolled, the median age was 72 years (range, 51-80), and 65% were male. Disease was classified as de novo AML (53%), secondary AML (38%), and therapy-related AML (10%). Prior hypomethylating-agent exposure was reported in 15% of patients.
Key Findings
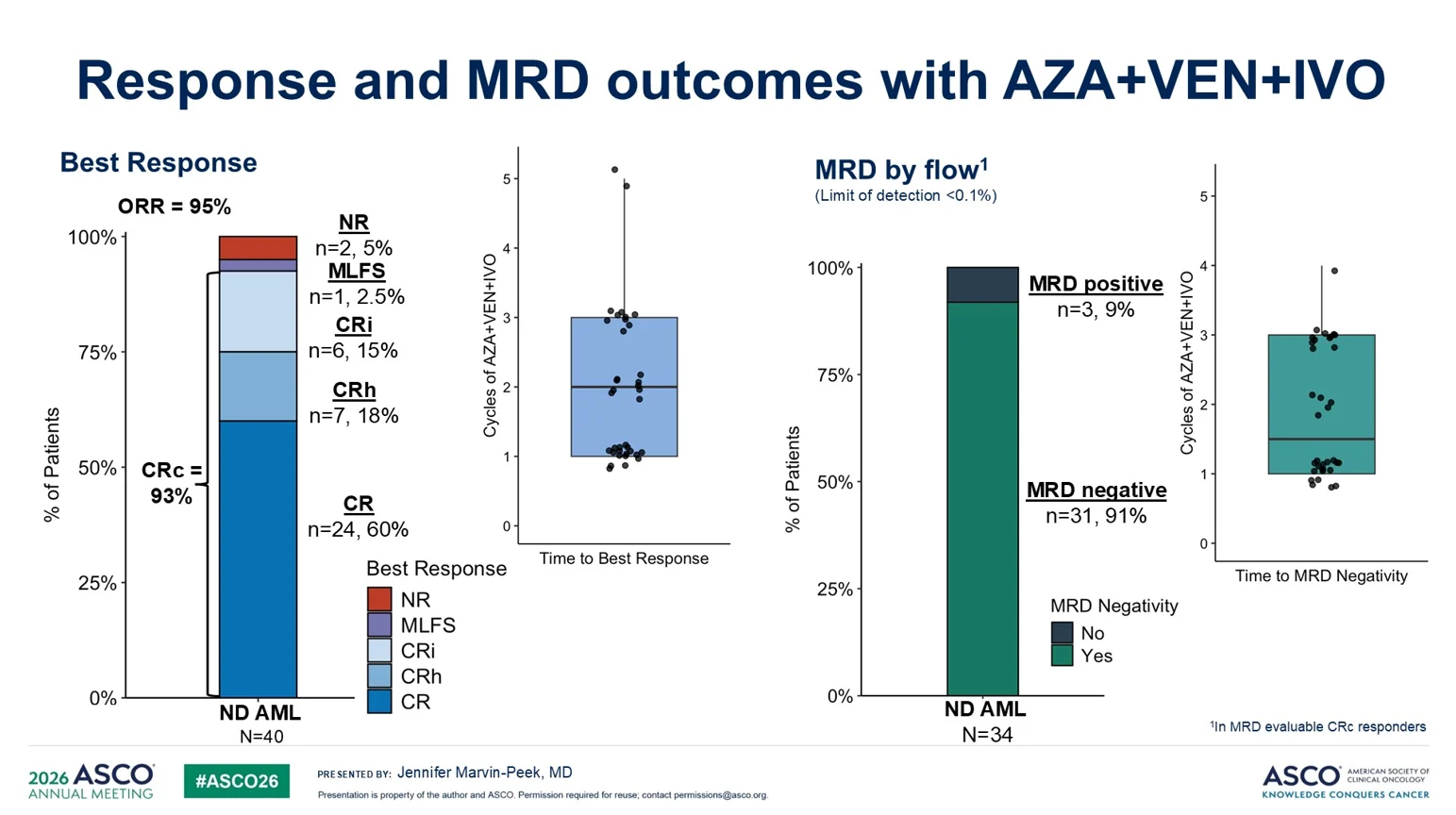
The AZA+VEN+IVO triplet achieved an ORR of 95%. A composite complete remission (CRc; CR + CRh + CRi) was observed in 93% of patients, including CR in 60%, CRh in 18%, and CRi in 15%. Responses were rapid, with a median time to best response of two treatment cycles. Among MRD-evaluable responders, 91% achieved MRD-negative remission.

After a median follow-up of 35 months, median OS and DOR had not been reached. The estimated 3-year OS and DOR rates were 79% and 83%, respectively. Relapse was observed in 7.5% of patients, corresponding to a 3-year cumulative incidence of relapse of 9%, and all relapse events were associated with the emergence of IDH1-negative clones. At the time of analysis, 30% of patients remained on study, while 45% had proceeded to allogeneic HSCT.

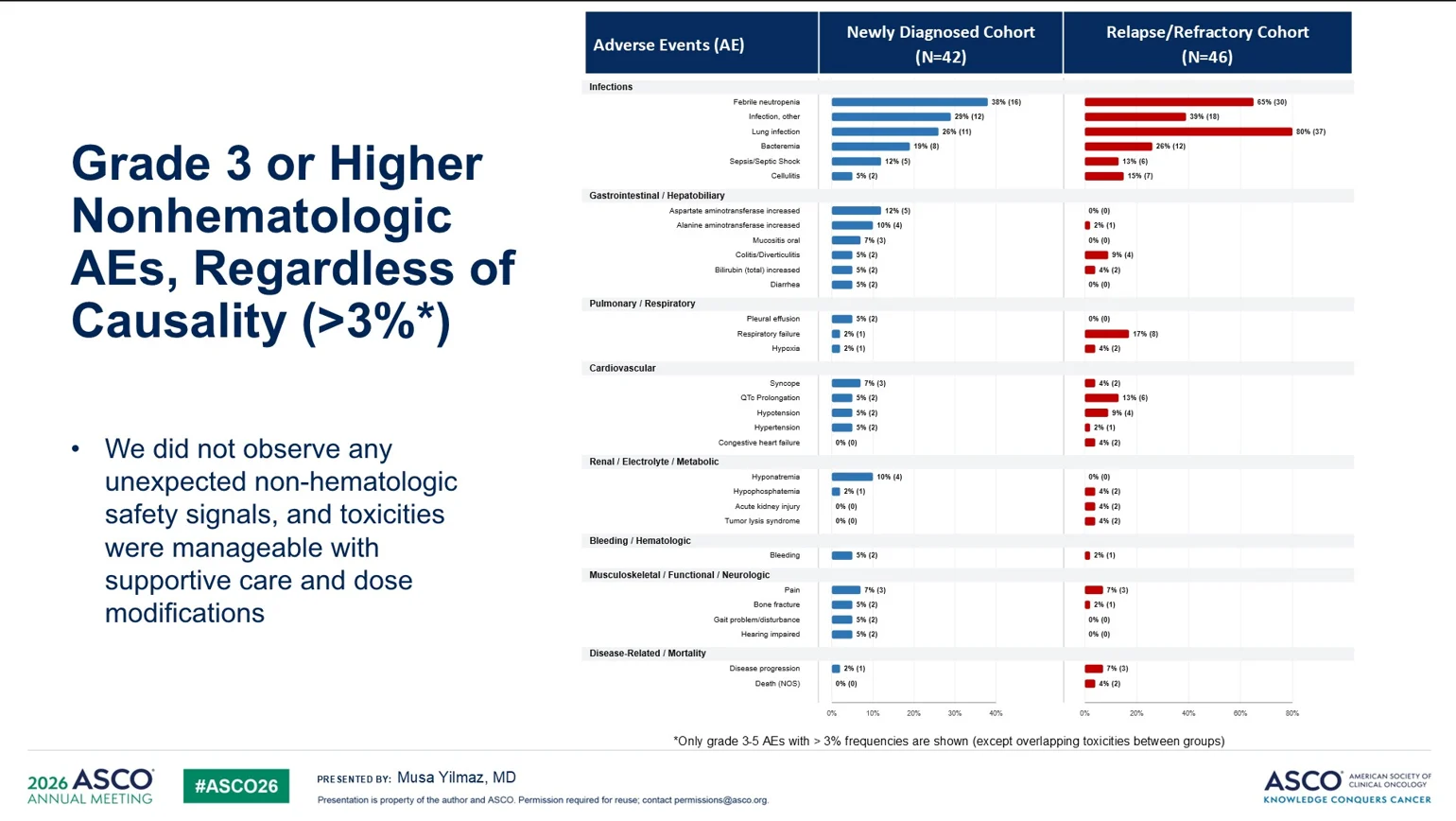
The regimen was generally well tolerated, with grade 3-4 non-hematologic adverse events reported in 30% of patients. Severe infections were the most common toxicity (15%), while tumor lysis syndrome (7.5%), QTc prolongation (5%), and differentiation syndrome (2.5%) were infrequent. No 30-day or 60-day mortality occurred.
Exploratory Analyses
Exploratory analyses identified co-occurring signaling pathway mutations as a potential adverse prognostic factor. Patients lacking signaling mutations achieved higher CRc rates (100% vs 80%; p=0.046) and superior 3-year OS (95% vs 54%; p=0.037). A trend toward improved remission durability was also observed (3-year DOR: 90% vs 66%).
The triplet regimen also demonstrated activity in therapy-related AML. Although CRc rates were lower than in non-tsAML patients (71% vs 97%), estimated 3-year OS and DOR remained favorable at 60% and 66%, respectively.

Bottom Line
In this multicenter study, triplet therapy with AZA+VEN+IVO achieved high MRD-negative response rates and durable remissions with a median follow-up of 35 months. Ongoing randomized studies, including EVOLVE-1 (NCT07075016), will clarify whether adding venetoclax to AZA+IVO should be incorporated into future treatment standards for IDH1-mutated AML.
Quizartinib in Combination With Decitabine and Venetoclax for Newly Diagnosed and Relapsed/Refractory FLT3-Mutated AML
FLT3-ITD mutations occur in approximately 20% of AML cases and are associated with constitutive FLT3 signaling, aggressive disease biology, and inferior outcomes. In patients treated with HMA-venetoclax, median OS remains approximately 9.9 months. Quizartinib is a potent second-generation FLT3 inhibitor with demonstrated survival benefits across multiple FLT3-mutated AML settings.
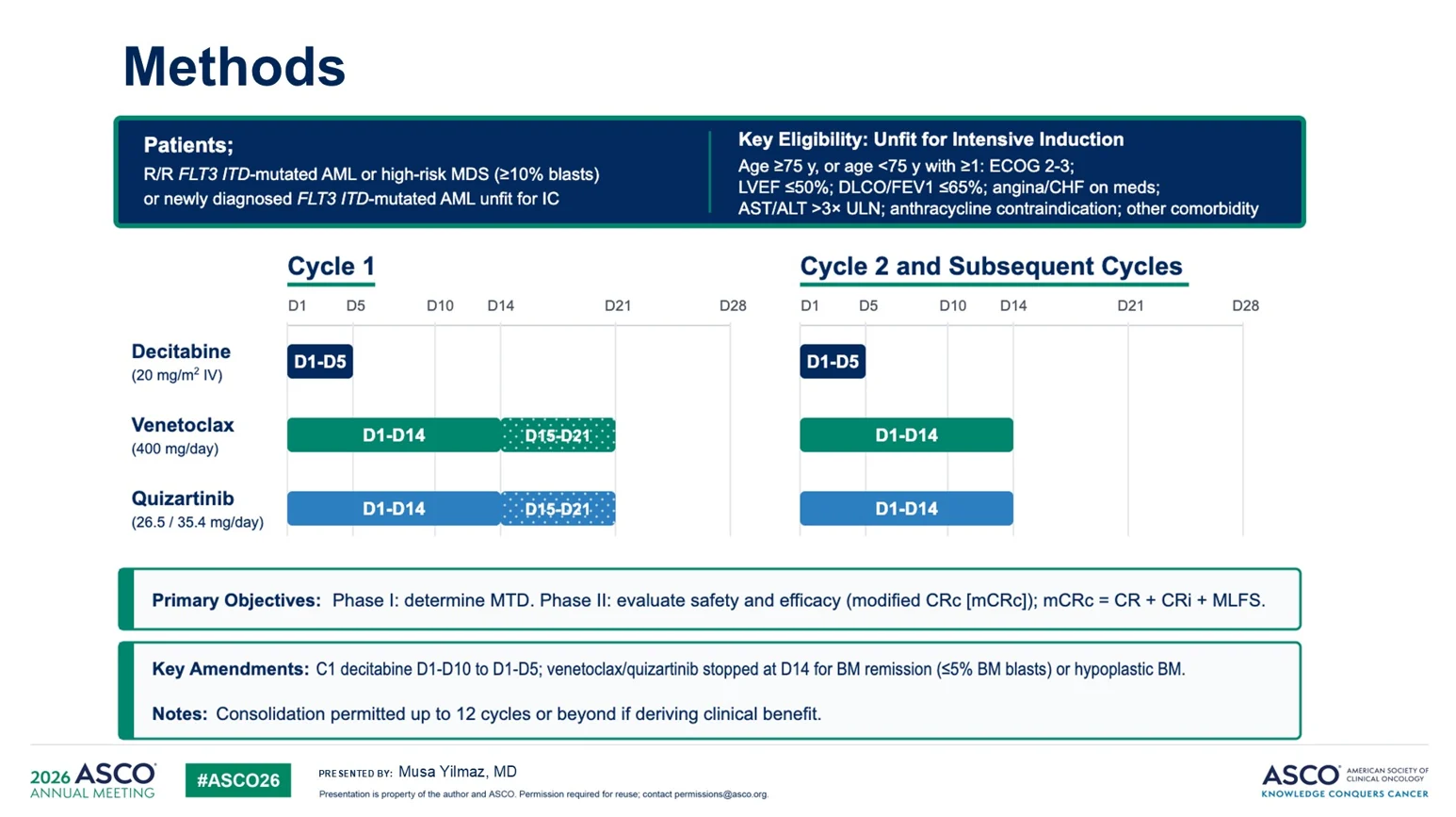
Presented by first author Musa Yilmaz, MD, this Phase I/II study (NCT03661307) evaluated the addition of quizartinib to decitabine and venetoclax in patients with newly diagnosed FLT3-ITD AML who were ineligible for intensive chemotherapy, as well as those with relapsed or refractory disease.
Study Design
Primary endpoints were maximum tolerated dose and overall response rate.
Treatment was administered in 28-day cycles:
- Decitabine 20 mg/m² on days 1-5
- Venetoclax 400 mg daily on days 1-14
- Quizartinib 26.5 or 35.4 mg daily on days 1-14
Phase I evaluated two quizartinib dose levels, with 26.5 mg/day selected as the recommended phase II dose (RP2D). Efficacy was assessed using mCRc (CR + CRi + MLFS), and MRD by MFC and FLT3-targeted NGS.
Results
A total of 88 patients were enrolled, including 42 with newly diagnosed (ND) FLT3-ITD AML and 46 with relapsed/refractory (R/R) disease. In Phase I, quizartinib 26.5 mg/day was selected as the RP2D after grade 4 myelosuppression was observed at the higher dose level.

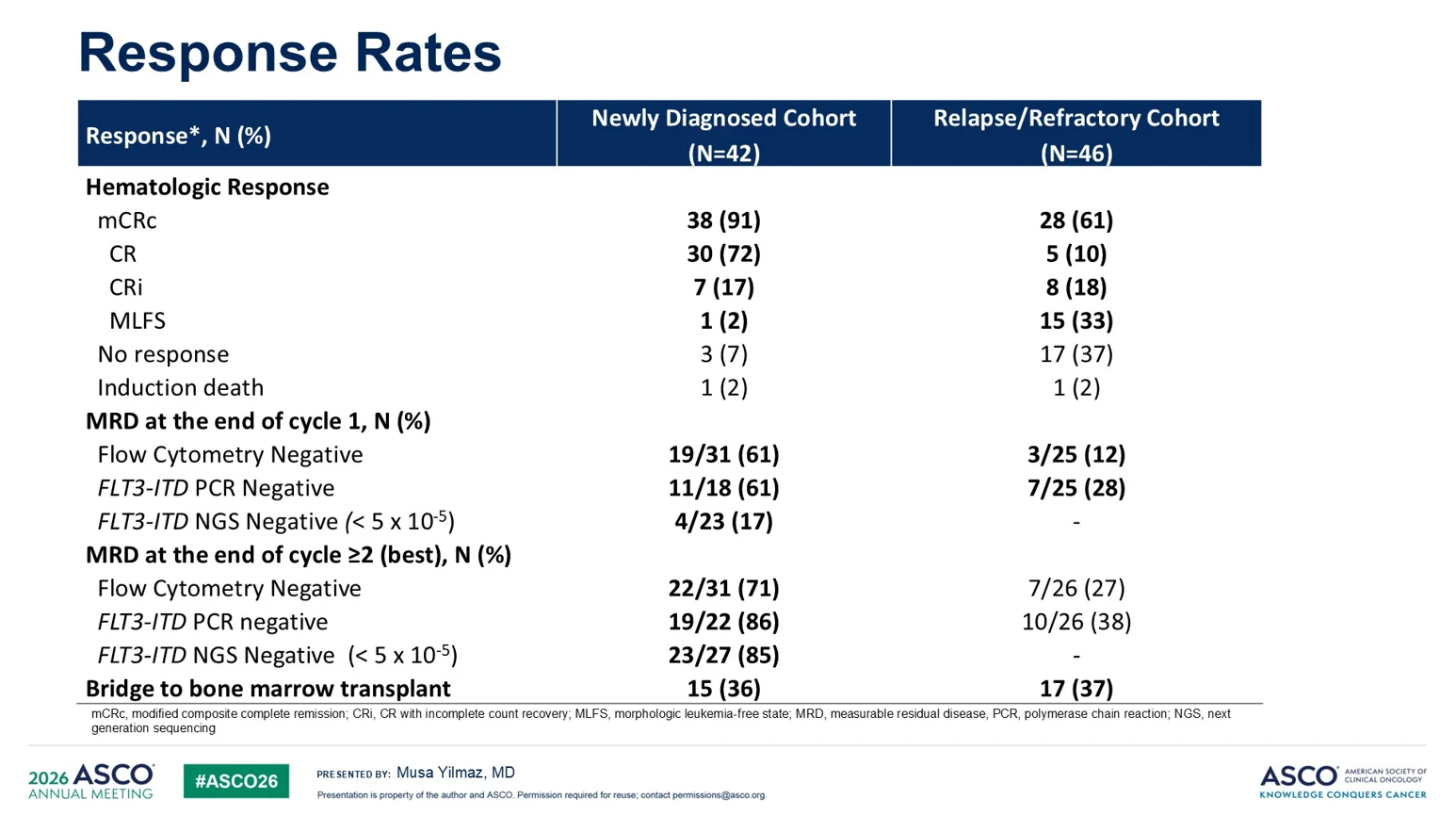
Newly diagnosed cohort:
- mCRc rate: 91% (CR 72%, CRi 17%, MLFS 2%)
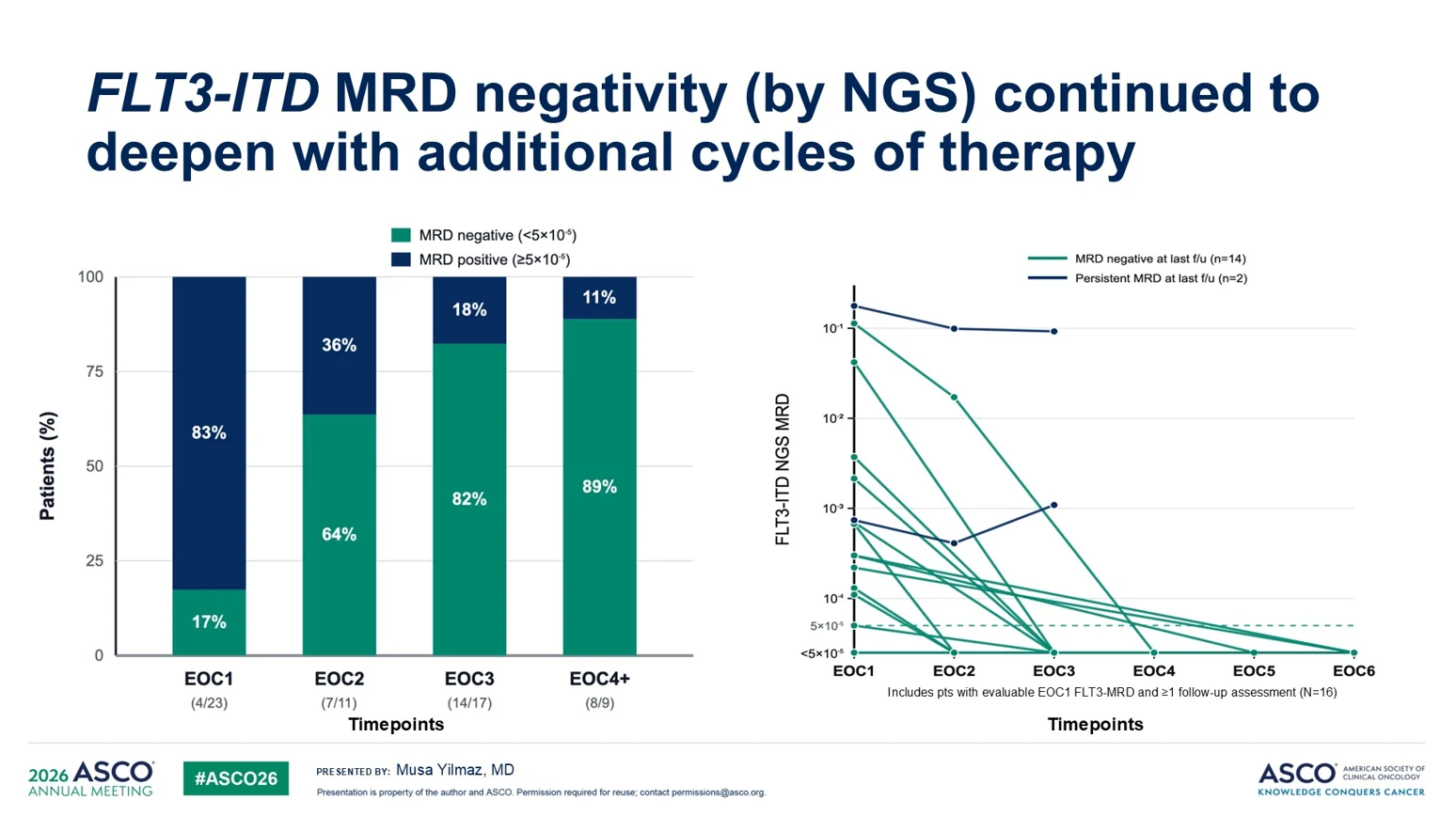
- MRD negativity deepened over time, reaching 71% by MFC and 85% by FLT3-targeted NGS
- 36% of patients proceeded to allo-HSCT
- Median RFS: 25 months
- Median OS: 36 months
Among 42 patients in the ND cohort, 38 achieved a response, 3 had no response, and 1 experienced induction death.
Relapsed/Refractory cohort:
- mCRc rate: 61%
- MRD negativity improved with continued therapy
- 37% of patients were bridged to allo-HSCT
- Median OS: 6.3 months

Responders had significantly longer OS than non-responders (8.1 vs 3.4 months; p<0.001), while prior HMA-venetoclax exposure was associated with inferior survival (4.6 vs 8.7 months; p=0.02).
To improve tolerability, protocol amendments shortened decitabine from 10 to 5 days and limited both venetoclax and quizartinib to 14 days. These changes accelerated hematologic recovery while maintaining clinical efficacy.
Bottom Line
Quizartinib, decitabine, and venetoclax achieved durable remissions and encouraging survival outcomes in FLT3-ITD AML, with manageable toxicity following schedule optimization. The regimen also served as an effective bridge to allo-HSCT for eligible patients.
Triplet Therapy May Deepen Remissions Beyond HMA-Venetoclax Alone
Compared with historical HMA-venetoclax data, both studies demonstrated substantially deeper responses. In IDH1-mutated AML, AZA-VEN-IVO achieved a CRc rate of 93%, compared with approximately 67% CR/CRi reported for IDH1-mutated patients treated with AZA-VEN in VIALE-A.
Similarly, DEC-VEN-QUIZ produced a CR+CRi rate of 89% in newly diagnosed FLT3-ITD AML, compared with approximately 67% reported historically for FLT3-mutated patients receiving HMA-venetoclax.
The discussion emphasized that response rates alone are insufficient. Increasingly, MRD negativity has emerged as an important surrogate for durable disease control. Data from VIALE-A demonstrated significantly improved survival among patients who achieved MRD negativity.
The triplet regimens generated particularly notable MRD outcomes, with MRD negativity rates reaching 91% in the IDH1 study and 71% in the FLT3 study.

Survival Signals Are Encouraging but Require Confirmation
The discussion also focused on the relationship between deeper remissions and long-term outcomes. In the IDH1 study, median OS was not reached after prolonged follow-up, with an estimated 3-year OS of 79%. In the FLT3 study, median OS reached 36 months in newly diagnosed patients, substantially longer than historical outcomes reported with HMA-venetoclax alone.
At the same time, neither study included a randomized control arm, and patient populations differed from those enrolled in VIALE-A and AGILE. As a result, the observed survival advantages should be viewed as hypothesis-generating rather than definitive evidence of superiority.
This is why ongoing randomized trials such as EVOLVE-1 will be critical for determining whether triplet therapy truly improves survival compared with current doublet standards.

Is More Really More?
Discussant Catherine Smith, MD, posed a central question, capturing the trade-off between the potential benefits of triplet therapy and the risk of increased toxicity.
“Is more really more?”
While deeper remissions and higher MRD negativity rates are desirable, adding targeted agents increases treatment complexity and can exacerbate myelosuppression. Notably, both studies required substantial schedule modifications and dose reductions over time.
The FLT3 study provides a particularly instructive example. Following protocol amendments that shortened decitabine exposure and limited both venetoclax and quizartinib to 14 days, hematologic recovery improved significantly. A successful implementation of triplet therapy may depend not only on the drugs themselves but also on careful schedule optimization.
An important takeaway is that dose modification should not necessarily be viewed as treatment failure. Rather, prolonged cytopenias may represent an expected consequence of highly active therapy, requiring individualized adjustment.
Frontline May Be the Optimal Setting for Targeted Triplets
Another notable observation is the apparent difference between newly diagnosed and relapsed disease.
In the quizartinib study, response rates declined from 91% in newly diagnosed patients to 61% in the R/R setting. Dr. Smith contrasts these findings with previously reported gilteritinib-venetoclax data, which achieved response rates around 75% in relapsed FLT3-mutated AML.
This raises an important question: are triplets most beneficial when used early, before clonal evolution and treatment resistance become established?
The discussion suggested that targeted agents may have their greatest impact when incorporated into frontline therapy, where they can maximize MRD eradication, prolong remission duration, and potentially prevent relapse altogether.
Looking Ahead
The results of both studies are encouraging and add to the growing body of evidence supporting molecularly tailored treatment strategies in AML. The next step will be determining whether the promising response, MRD, and survival outcomes observed in these early-phase studies can be confirmed in randomized trials and translated into meaningful long-term benefit for patients.

FDA Grants Approval for Oral Decitabine/Cedazuridine With Venetoclax in Newly Diagnosed AML
Written by Susanna Mikayelyan, MD
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}