


First results from the phase 2 ERASMM (EMN34, NCT06183489) study, evaluating elranatamab as an early therapeutic intervention in patients with high-risk smoldering myeloma, were presented by Cyrille Touzeau, MD, PhD at ASCO 2026.
The results provided insight into whether early intervention with elranatamab could achieve deep responses while maintaining acceptable safety in patients without symptomatic end-organ damage.
Rationale for Early Intervention
SMM represents an asymptomatic precursor stage between MGUS and active MM. Early intervention with lenalidomide or daratumumab have previously demonstrated delayed progression to active disease in patients with HR SMM.
Elranatamab, a BCMA×CD3 BsAb, has shown significant activity in heavily pretreated MM, with manageable toxicity profiles. The use of T-cell-redirecting therapy in HR-SMM is biologically compelling, as this setting is generally associated with a more intact immune microenvironment and less T-cell exhaustion compared with relapsed MM, potentially enabling stronger immune control.
Study Design
ERASMM is an international, open-label, multicenter phase 2 study conducted across 17 European Myeloma Network centers. Eligible patients were adults with HR SMM defined according to the Mayo 2018 “20-2-20” criteria, requiring the presence of at least two high-risk features.
Treatment consisted of fixed-duration subcutaneous elranatamab administered for up to 2 years. Priming doses included 12 mg on C1D1 and 32 mg on C1D4, followed by 76 mg on C1D8 and C1D15. Subsequent dosing was administered on C2-3 D1 and D15, followed by once-per-cycle dosing from C4-24 on a 28-day schedule.
The primary endpoint was CR rate after 6 cycles. Key secondary endpoints included safety, ORR, MRD, PFS, PFS2, time to SLiM/CRAB progression, and OS.

Patient Population
Between May 2024 and September 2025, 50 previously untreated HR SMM patients were enrolled. The median age was 65 years. Baseline disease characteristics included:
- 84% of patients had an M-protein level >20 g/L
- 72% had bone marrow plasma cell infiltration >20%
- 66% had a free light chain ratio >20.
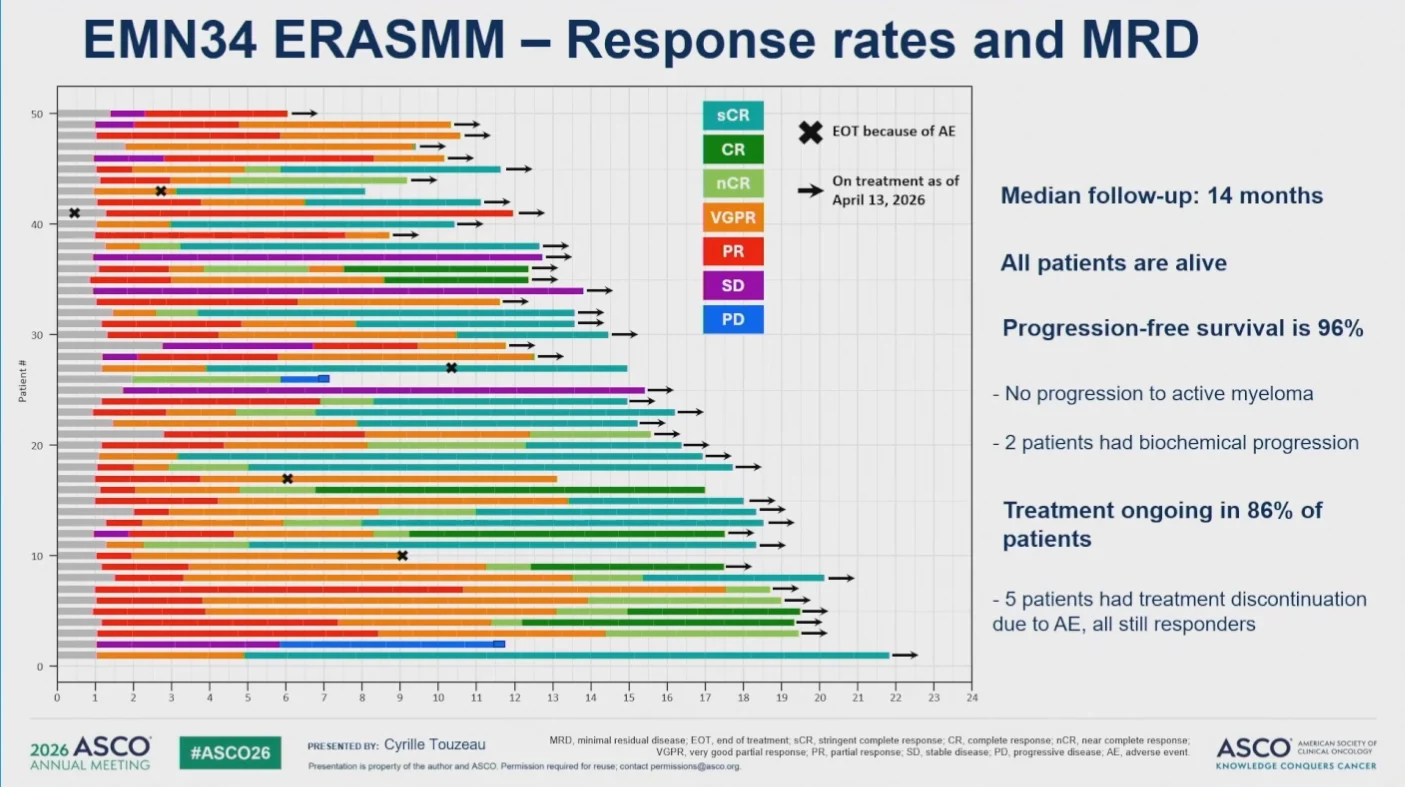
Efficacy Findings
At a median follow-up of 14 months, single-agent elranatamab achieved an ORR of 92%, including a CR rate of 72%. MRD negativity in 90% of evaluable patients with suspected CR. PFS was 96%, no patients progressed to active myeloma, and all patients were alive at the time of analysis.

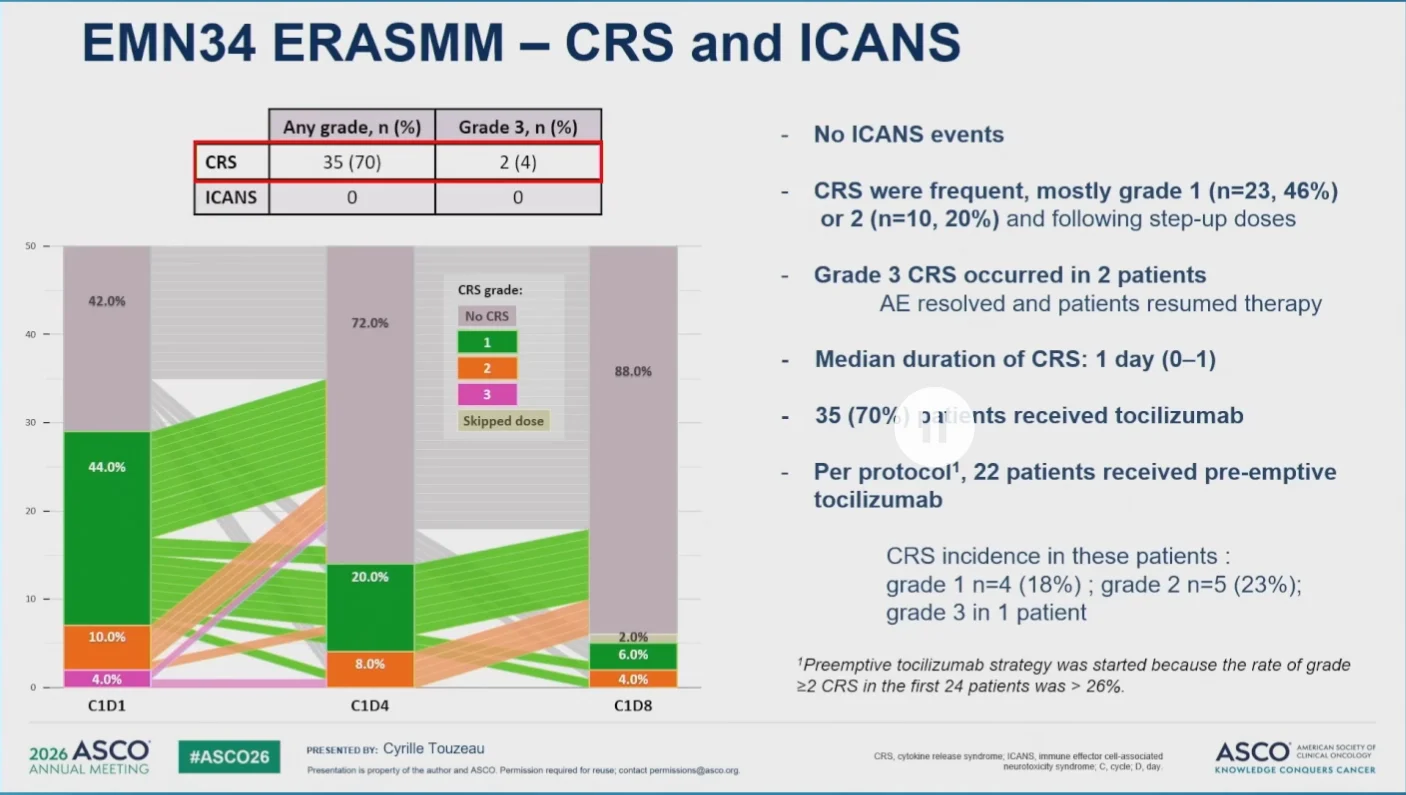
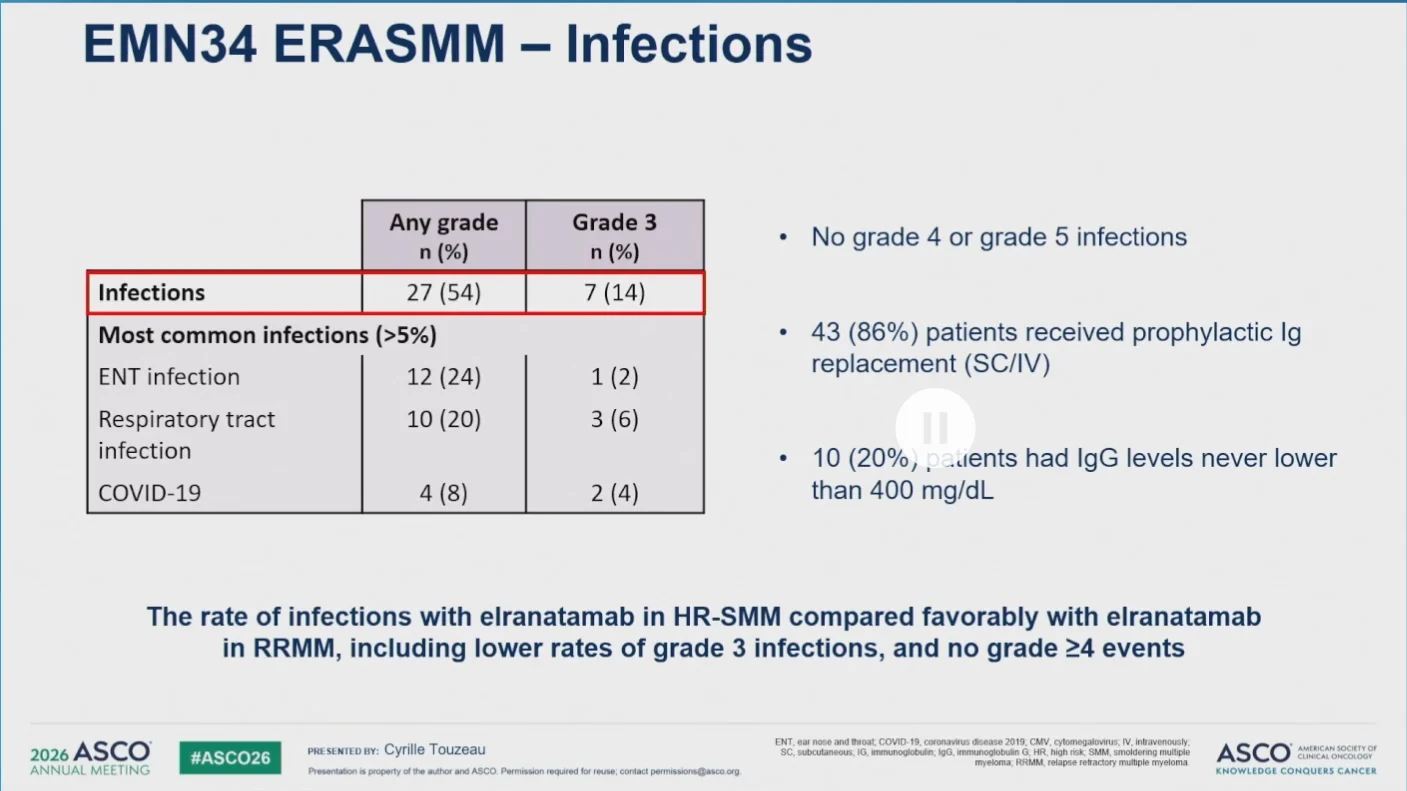
Safety Findings
CRS occurred in 70% of patients and was mostly grade 1/2, with only two grade 3 events reported. No ICANS events were observed.
Infections occurred in 54% of patients, including grade 3 infections in 14%, with no grade 4 or 5 infectious events reported. Other common non-hematologic adverse events included skin rash (38%), fatigue (32%), diarrhea (26%), and peripheral neuropathy (16%), most of which were grade 1/2.
Treatment discontinuation due to AEs occurred in 5 patients. Reported causes included Guillain-Barré syndrome, hypertransaminasemia, infections, and peripheral neuropathy.

Potential Impact
The early ERASMM findings demonstrated a strong efficacy signal for elranatamab in HR-SMM. No patients progressed to active myeloma in this early analysis, raising important questions about whether early intervention could alter the natural history of high-risk disease.
While longer follow-up is needed to better define durability, MRD outcomes, and long-term progression prevention, single-agent elranatamab demonstrated notable clinical activity with manageable toxicity, supporting further evaluation in HR-SMM.
Discussion Point
Regarding concerns that early anti-BCMA exposure could compromise the activity of subsequent BCMA-directed therapies once patients progress to active MM, the presenter noted that the fixed-duration design was an important aspect of the study, aiming to potentially reduce the risk of later BCMA antigen escape.
{kind=link}
{kind=link}
{kind=link}