


Frontline treatment strategies for newly diagnosed multiple myeloma (NDMM) continue to evolve with the incorporation of immunotherapy. Following the success of anti-CD38-based quadruplets, BCMA-directed therapies are increasingly being evaluated earlier in the course.
DREAMM-9 (NCT04091126) was a phase 1 dose- and schedule-evaluation study investigating the addition of belantamab mafodotin (belamaf), a BCMA-directed antibody-drug conjugate, to the standard bortezomib, lenalidomide and dexamethasone (VRd) backbone in transplant-ineligible (TI) NDMM. Results were presented by Saad Z. Usmani.
Clinical Background
Belamaf has demonstrated clinically meaningful activity across RRMM combination studies through a multimodal mechanism involving direct cytotoxicity and immune-mediated effects.
Yet, ocular toxicity, particularly keratopathy and visual acuity changes, remains the defining adverse event limiting broader and prolonged use. Optimizing dosing schedules to balance efficacy and tolerability is therefore of particular clinical importance, especially in older or frailer patients receiving extended frontline therapy.
In this context, DREAMM-9 provides important insight into whether modulation of belamaf dose intensity during induction and maintenance can preserve deep responses while improving tolerability.
Study Methods
As of June 2, 2025, 118 patients were enrolled in the intention-to-treat population. Patients received BVRd across 8 different belamaf dosing cohorts, categorized according to dosing frequency and intensity:
- SHORT schedules (Q3/4W): 1.9 mg/kg,1.4 mg/kg,1.0 mg/kg
- STRETCH schedules (Q6/8W): 1.9 mg/kg, 1.4 mg/kg
- Step-down schedules (Q9/12W): 1.9 to 1.4 mg/kg, 1.4 to 1.0 mg/kg
- Extended schedule (Q12W): 1.0 mg/kg
The primary endpoint was safety, with particular attention to ophthalmic adverse events assessed through ophthalmic examination findings (OEFs) according to the Keratopathy and Visual Acuity scale. Responses, MRD negativity in complete response or better (CR+), and patient-reported outcomes (PROs) were assessed.
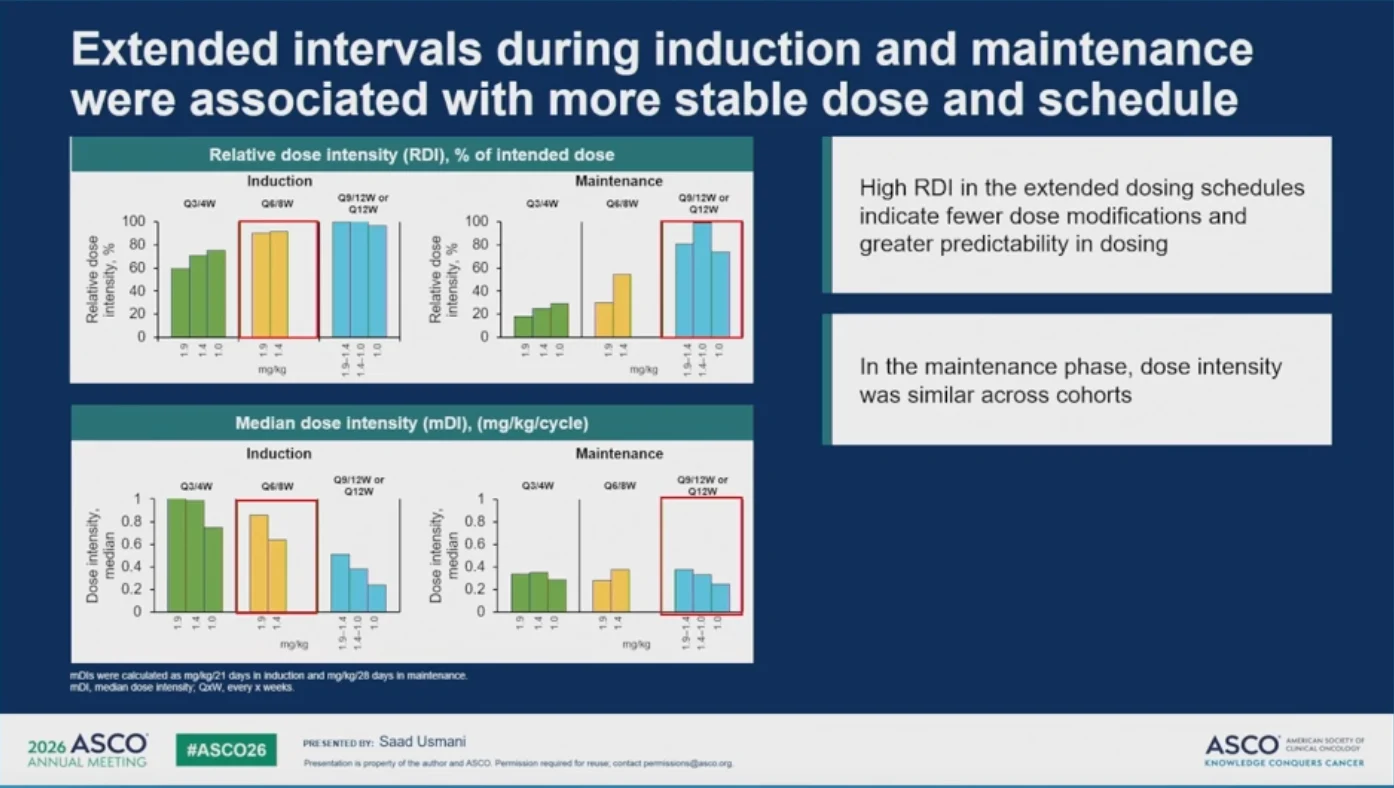
Median dose intensities (mDIs) were calculated separately for induction (mg/kg/21 days) and maintenance (mg/kg/28 days) phases to better understand the relationship between exposure, efficacy and toxicity.
Results
The study demonstrated consistently high anti-myeloma activity across all dosing cohorts. ORRs were ≥83%. Outcomes varied according to belamaf induction dose intensity.
Patients receiving higher induction mDI regimens, primarily the pooled SHORT and STRETCH cohorts, achieved the deepest responses:
- Q3/4W (SHORT cohorts) achieved CR or better and MRD negativity rates of 68% and 55%, respectively.
- Q6/8W (STRETCH cohorts) achieved CR or better and MRD negativity rates of 88% and 54%, respectively.
In contrast, Q9/12W cohorts achieved CR or better and MRD negativity rates of 61% and 41%, respectively, while Q12W cohorts achieved rates of 57% and 46%, respectively.

Safety Data
Safety analyses showed a clear relationship between induction dose intensity and ocular toxicity. Grade ≥2 ophthalmic examination findings occurred in:
- ≈ 90% of patients in pooled SHORT/STRETCH cohorts
- ≈ 69% of patients in pooled Q9/12W and Q12W cohorts
The first grade ≥3 ophthalmic findings resolved before the end of treatment in 86-100% of patients across cohorts. Five of the 8 cohorts had no belamaf discontinuations due to grade ≥3 OEFs, which were observed only in SHORT cohorts (n=1 each).
Long-interval schedules were not associated with meaningful deterioration in vision-related function across most timepoints, supporting a more favorable tolerability profile compared with SHORT schedules. In the maintenance phase, median dose intensity was similar across cohorts, likely reflecting dose modifications during treatment.

Key Takeaways
- BVRd demonstrated high ORRs across all dosing schedules.
- Higher induction dose intensity produced superior CR+ and MRD negativity rates.
- Higher dose intensity was associated with increased ocular toxicity, though most grade ≥2 events resolved before treatment completion.
- Longer dosing intervals improved tolerability.
Conclusion
DREAMM-9 demonstrated activity of belantamab mafodotin across all cohorts while highlighting the impact of induction dose intensity on both depth of response and ocular toxicity. The findings support a dosing strategy in which higher induction dose intensity is followed by longer-interval maintenance dosing to improve tolerability and maintain responses in TI NDMM.
{kind=link}
{kind=link}