


At the 2026 ASCO Annual Meeting, Naveen Pemmaraju, MD, presented results from a Phase II investigator-initiated study (NCT04216524) evaluating the combination of tagraxofusp, Hyper-CVAD, and venetoclax in both newly diagnosed and relapsed/refractory blastic plasmacytoid dendritic cell neoplasm (BPDCN).
Clinical Context and Rationale
BPDCN is an ultra-rare, aggressive hematologic malignancy characterized by multicompartment involvement and historically poor outcomes, with a median OS of approximately 8-12 months.
Tagraxofusp (TAG), a CD123-directed therapy, became the first approved targeted agent for BPDCN after demonstrating rapid and durable responses, although relapse and CNS involvement remain major therapeutic barriers. Ongoing efforts are therefore focused on TAG-based combination strategies aimed at improving response durability.
Venetoclax, a BCL2 inhibitor with demonstrated activity in BPDCN, may enhance apoptotic sensitivity and improve therapeutic efficacy. In parallel, Hyper-CVAD-based regimens have shown substantial activity in lymphoid malignancies and may help reduce CNS relapse risk in BPDCN.
Based on these observations, the combination of the CD123-targeted agent tagraxofusp with venetoclax and Hyper-CVAD-based chemotherapy was hypothesized to improve outcomes while also bridging patients to allogeneic SCT.

FDA Approved Decnupaz (pivekimab sunirine-pvzy), the First ADC for Adults With BPDCN
Patient Population
This phase II, single-arm study enrolled 21 adults (≥18 years) with newly diagnosed (n=16) or R/R (n=5) BPDCN, ECOG performance status 0-2, and adequate organ function. Frontline patients were permitted to receive up to one prior cycle of BPDCN-directed therapy before enrollment. The median age was 61 years, and most patients were male.
Skin involvement was the predominant disease manifestation (86%), followed by bone marrow involvement (57%), while CNS and lymph node involvement were less frequent. The most common co-occurring mutations included TET2, ASXL1, and DNMT3A. Two pts had prior/concomitant MDS.
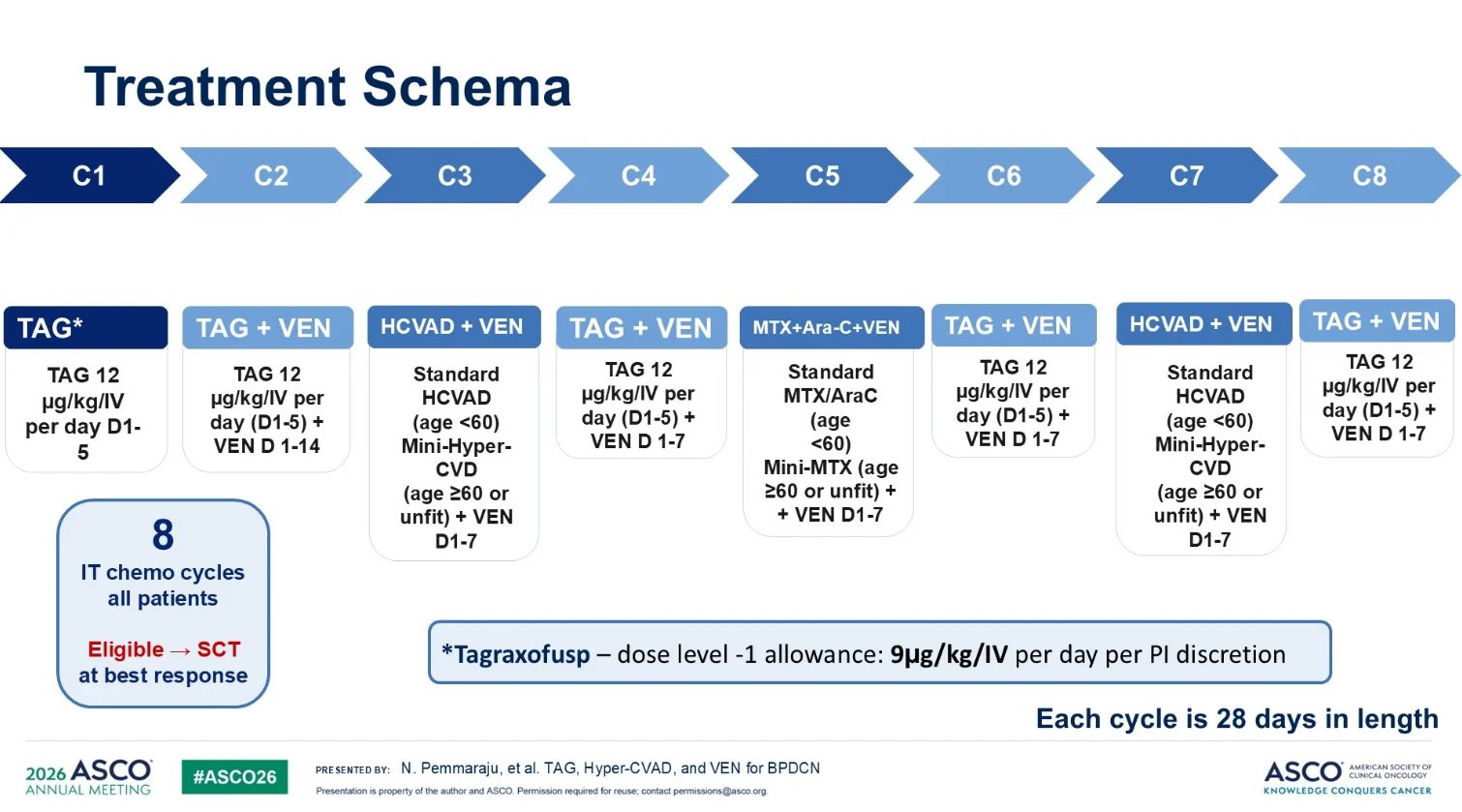
Treatment Schema
Patients received a sequential TAG-, venetoclax, and Hyper-CVAD-based regimen over up to 8 cycles. TAG monotherapy was administered during cycle 1, followed by alternating TAG+VEN combinations and VEN-based Hyper-CVAD/mini-hyper-CVD or methotrexate/cytarabine-containing cycles. All cycles were 28 days in duration, followed by maintenance with POMP, VEN, and TAG. Patients also received CNS prophylaxis with ≥8 intrathecal treatments.
Safety and Tolerability
The most common treatment-emergent adverse events were edema, elevated liver function tests, pain, nausea/dyspepsia, and fatigue, with most events being grade 1-2. Grade ≥3 toxicities were relatively infrequent, though elevated LFTs represented the most common higher-grade AE.
Capillary leak syndrome, a known toxicity of tagraxofusp, occurred in 19% of patients, including 10% with grade 3 events, with all episodes occurring during cycle 1 and resolving with supportive management, including intravenous diuresis and albumin administration. No grade 4-5 CLS events were reported.
Dose modifications of tagraxofusp were commonly implemented, largely driven by age, frailty, comorbidities, or treatment-related toxicities, particularly elevated LFTs. Successful mitigation strategies included shortening treatment duration and reducing the tagraxofusp dose.

Clinical Responses and Outcomes
Across the overall cohort of 21 patients, ORR was 90% (19/21), including CR in 67% (14/21) and CRi in 10% (2/21). Responses were typically observed early, with best response achieved after a median of 2 cycles. More than half of patients (57%,12/21) subsequently proceeded to SCT.
Treatment-Naïve BPDCN
At a median follow-up of 30.2 months, ORR reached 94% (15/16), including CR in 82% and CRi in 13%. Responses occurred rapidly, with best response achieved after a median of 1 cycle. No 30- or 60-day mortality was reported. Additionally, 63% of frontline patients proceeded to SCT(45% historical control rate with tagraxofusp monotherapy).

Relapsed/Refractory BPDCN
At a median follow-up of 34.5 months, ORR was 80% (4/5), including CR in 40%. Median OS was 8.9 months, while median EFS was 7.4 months. Two of five patients proceeded to SCT, supporting the activity of this TAG-, venetoclax-, and Hyper-CVAD-containing approach in a heavily challenging disease setting.

Landmark SCT Analysis
A landmark survival analysis in frontline BPDCN used a transplant landmark time of 2.9 months to assess outcomes by SCT status. Among 16 frontline patients, 10 proceeded to allogeneic SCT, with a median age of 60 years at transplant. Survival outcomes favored the transplanted cohort, with median OS not reached after SCT versus 2.6 months in non-transplanted patients. The 1-year OS after SCT was 64%.
Survival and Disease Course
Five frontline patients remained in long-term CR beyond 2 years, indicating the potential for durable remissions in a subset of patients. However, relapses were still observed, including after SCT, and several deaths in CR occurred, primarily due to sepsis.
In the R/R cohort, responses were generally less durable, with multiple relapses, post-transplant progression in some patients, and early sepsis-related deaths.

Bottom Line
This regimen demonstrated its most favorable activity in the frontline setting, with high response rates, no high-grade CLS or early mortality, frequent SCT consolidation, durable remissions in a subset of patients, and no CNS relapses observed. At the same time, relapses and infectious complications remained important challenges, particularly in the R/R setting, emphasizing the need for continued therapeutic optimization.
Toward Broader BPDCN Evidence
In this context, the BPDCN International Registry, launched in 2022 (NCT05430971) by the Immune Oncology Research Institute in Armenia, represents an initiative aimed at expanding the global evidence base for this ultra-rare malignancy and generating larger datasets to validate emerging findings and inform future therapeutic approaches. Continued international collaboration and real-world data contribution will be important for improving the understanding and management of BPDCN.
{kind=link}