


During an oral presentation at EHA 2026, Timothy Hughes reported long-term findings from the phase 3 ASC4FIRST trial (NCT04971226). After approximately 3 years of follow-up, asciminib continued to demonstrate higher molecular response rates and a favorable safety profile compared with both imatinib and second-generation TKIs in patients with newly diagnosed Philadelphia chromosome-positive chronic myeloid leukemia in chronic phase (CML-CP).
Why This Analysis Matters
Several TKIs are currently approved for newly diagnosed CML-CP. As patients often remain on therapy for many years, long-term follow-up studies are important for assessing the durability of molecular responses, treatment persistence, and safety across frontline options.
Asciminib is a first-in-class Specifically Targeting the ABL Myristoyl Pocket (STAMP) inhibitor with a mechanism distinct from ATP-competitive TKIs. In the phase 3 ASC4FIRST trial, asciminib previously demonstrated superior efficacy and improved tolerability compared with investigator-selected TKIs at both the primary 48-week analysis and the key secondary 96-week analysis.

Methods
ASC4FIRST is a multicenter, open-label study. Participants were randomized 1:1 to receive asciminib 80 mg once daily or an investigator-selected TKI administered according to approved labeling.
Randomization was stratified by ELTS risk category and by the TKI selected before randomization, either imatinib or a second-generation (2G) TKI. The present analysis was performed at week 144 with a data cutoff of September 29, 2025.
The study evaluated molecular response rates, survival outcomes, and safety. Event-free survival events included treatment failure according to ELN 2020 criteria, confirmed loss of MMR, discontinuation due to adverse events, disease progression, or death.
Major Molecular Response
In the imatinib stratum, MMR was achieved by 79.2% of patients receiving asciminib compared with 47.1% of those receiving investigator-selected imatinib, corresponding to a treatment difference of 32.6% (95% CI, nominal P<.001).
In the second-generation TKI stratum, MMR rates were 75.0% with asciminib and 59.8% with investigator-selected 2G TKIs, resulting in a treatment difference of 15.2%.
The presentation noted that these comparisons were not α-controlled and that the study was not designed to formally confirm statistical significance for this endpoint. Nevertheless, the observed differences favored asciminib across both treatment strata, also with higher MR4, and MR4.5 rates than comparator TKIs.

Long-Term Outcomes
The probability of EFS at week 144 was 83% with asciminib vs 63% with imatinib and 87% vs 75% for asciminib and 2G TKIs.
Estimated PFS at three years remained high across all treatment groups, reaching 97% vs 93% in the imatinib comparison and 99% vs 97% in the 2G TKI comparison. Overall survival was similarly high, ranging from 96% to 99%.
No new BCR::ABL1 mutations emerged with asciminib after the week 96 analysis, whereas one new mutation was reported in the imatinib group and one in the second-generation TKI group.
Safety and Tolerability
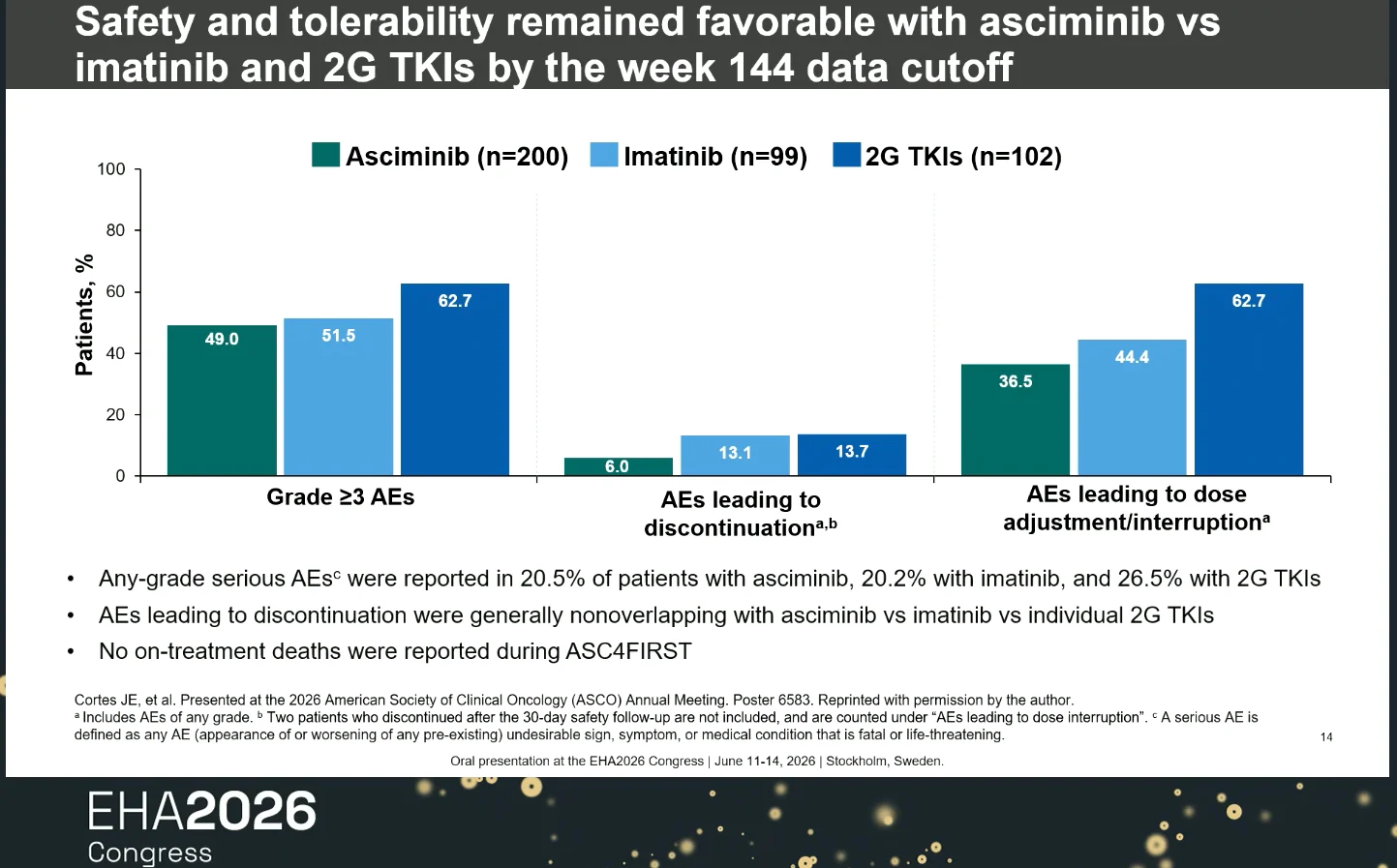
Safety and tolerability remained favorable with asciminib at the data cutoff. Compared with both imatinib and second-generation TKIs, asciminib was associated with lower rates of grade ≥3 adverse events, treatment discontinuation due to adverse events, and dose adjustments or treatment interruptions.
Serious adverse event rates were generally comparable across treatment groups. Among patients in the imatinib stratum, several hematologic toxicities, including thrombocytopenia, neutropenia, leukopenia, anemia, and lymphopenia, were reported less frequently with asciminib. No on-treatment deaths were reported during ASC4FIRST.

Clinical Context
Results from the ASC4FIRST week 144 analysis are consistent with those reported in the primary and key secondary analyses. Extended follow-up did not identify new treatment-emergent BCR::ABL1 mutations in the asciminib arm. These findings support the favorable benefit-risk profile of asciminib compared with currently available standard-of-care TKIs in newly diagnosed Ph-positive CML-CP. The study remains ongoing, with analyses planned to assess treatment-free remission eligibility and success.
You can watch more on OncoDaily TV.
{kind=link}