


Susheel Kumar Yeshala, Consultant Medical Oncologist at American Oncology Institute, shared a post on LinkedIn:
“Had the opportunity to participate in a great panel discussion on metastatic triple-negative breast cancer (mTNBC) at the IAIO forum.
The dialogue was rich, evidence-based, and focused on evolving standards of care.
Here are some of the key takeaways that emerged — sharing them for colleagues who could not attend:
Key Takeaways in mTNBC
- Precision Testing Matters
PD-L1 CPS, germline BRCA, and repeat metastatic biopsy are essential. HER2-low status is dynamic and can open doors to ADCs. - First-Line Treatment Is Biomarker-Driven
Pembrolizumab + chemotherapy remains standard for PD-L1 CPS ≥10 (KEYNOTE-355).
Chemotherapy ± platinum for PD-L1–negative disease.
PARP inhibitors → only for germline BRCA mutations. - ADCs Are Changing Outcomes
Sacituzumab govitecan (ASCENT) significantly improves OS in pretreated mTNBC.
T-DXd is practice-shifting for HER2-low metastatic breast cancer (mBC), with ongoing trials exploring its use in earlier lines of treatment. - CNS Involvement Remains a Major Challenge
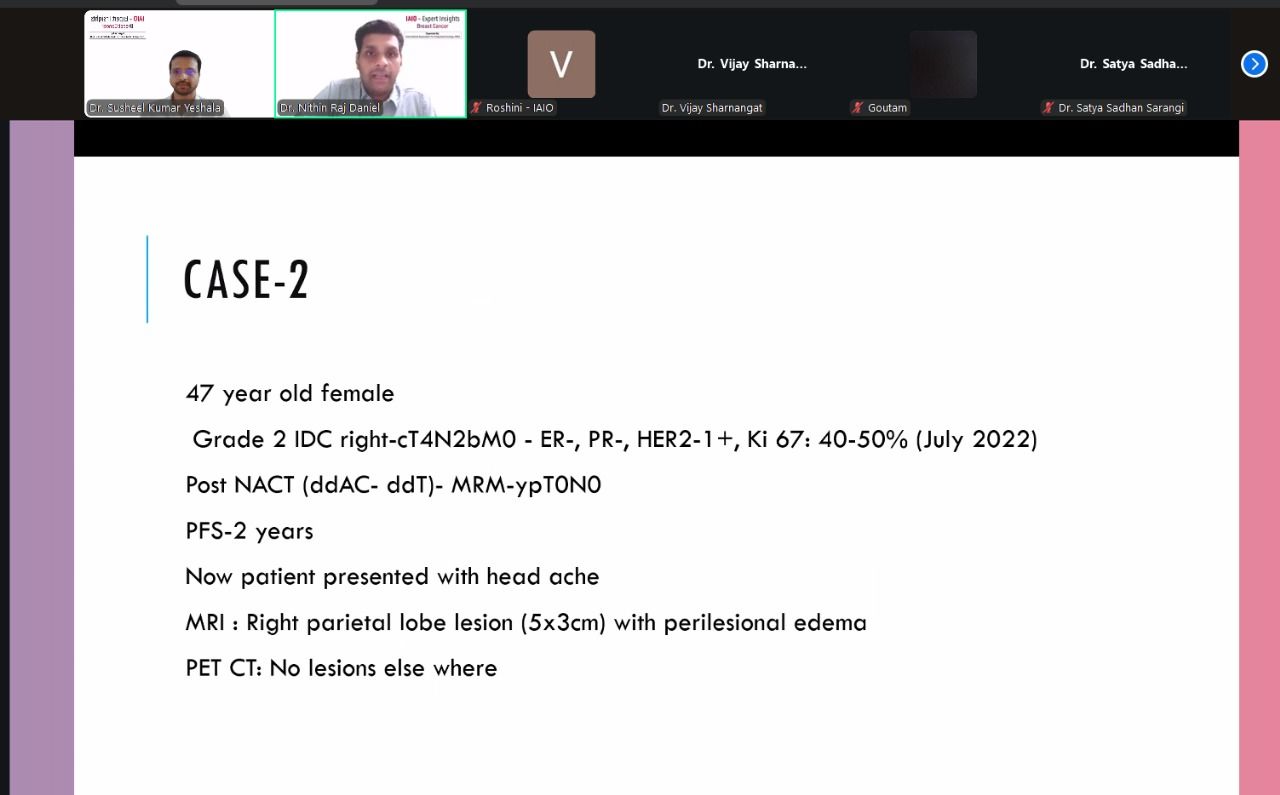
Up to 1/3 of mTNBC patients develop brain metastases. We urgently need CNS-penetrant systemic therapies. - Repeat Biopsy Is Increasingly Important
Receptor conversions (ER/PR/HER2), including HER2-low shifts, are common and influence the sequencing of therapy.
Unmet Needs
- CNS-active systemic agents
- Better biomarkers beyond PD-L1
- Predictors for ADC benefit and sequencing
- Strategies to overcome IO and ADC resistance
- Targetable pathways for the BRCA-WT majority
- Less toxic, durable regimens
Future research must focus on these areas to help us move toward true precision oncology and better long-term outcomes in mTNBC.
I am grateful to IAIO for the opportunity and look forward to continued collaboration and learning.”

More posts featuring Susheel Kumar Yeshala.
{kind=link}