


The Phase III RASolute 302 trial data presented at ASCO 2026 has sparked widespread discussion across digital oncology platforms. Evaluating the multi-selective RAS(ON) inhibitor daraxonrasib in previously treated metastatic pancreatic cancer, the trial earned a rare standing ovation for nearly doubling median overall survival to 13.2 months. Digital discourse is heavily focused on whether these unprecedented results officially shatter the “undruggable” status of the RAS oncogene, with clinicians online actively debating how quickly this breakthrough will reshape the global standard of care.
Below is a selection of key highlights and perspectives shared by global oncology leaders.
Piotr J. Wysocki
“It took 15 years to again achieve a huge progress in the treatment of pancreatic cancer – the groundbreaking RASolute 302 trial in RAS-mutated PDAC”
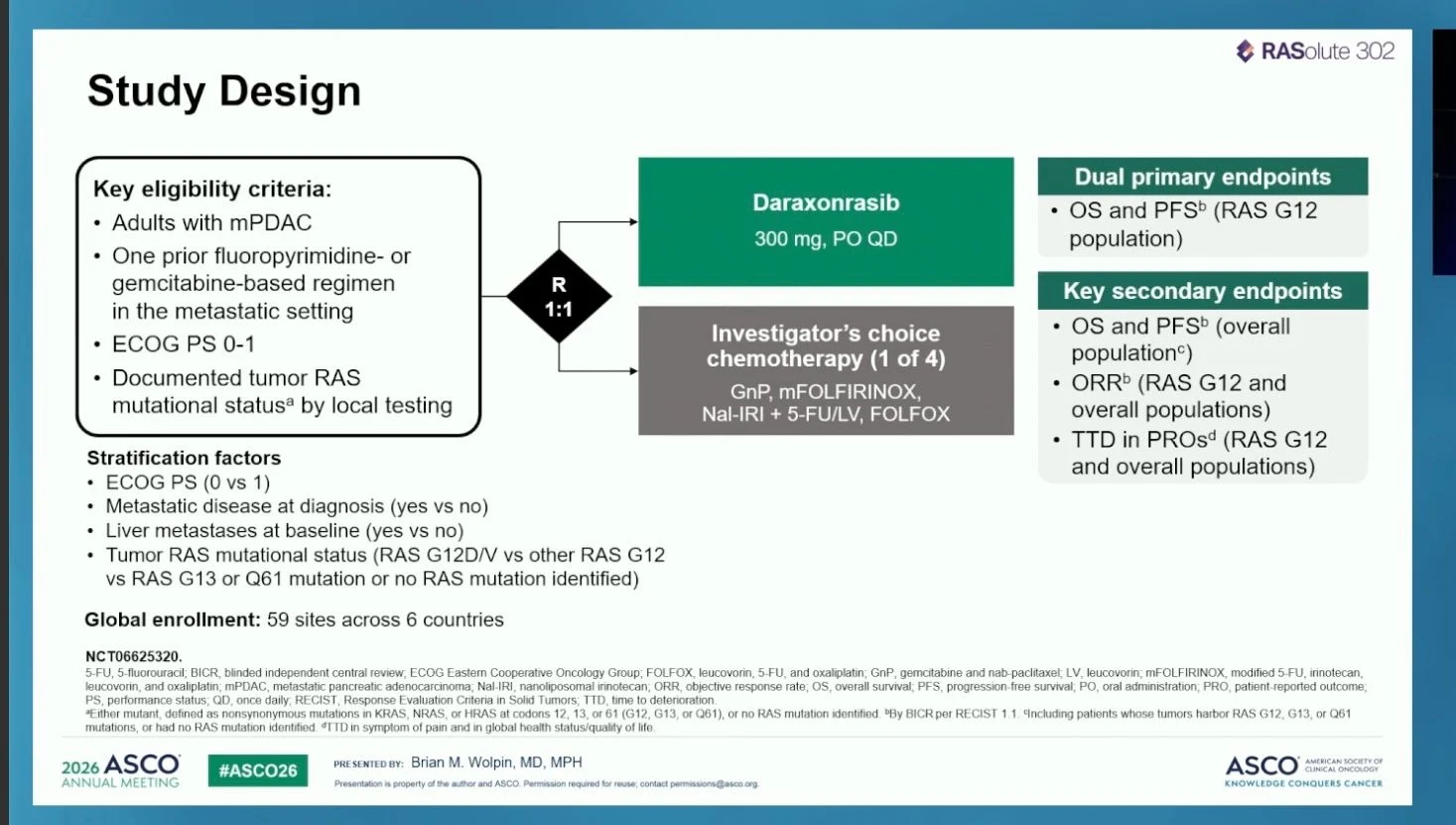
O’Reilly EM et al. published the primary results of the phase 3 RASolute 302 trial, evaluating daraxonrasib – an oral RAS(ON) multiselective, tri-complex inhibitor of the active GTP-bound state of both mutant and wild-type RAS – versus chemotherapy of investigator’s choice in patients with previously treated metastatic pancreatic ductal adenocarcinoma (mPDAC).
A total of 500 patients were randomly assigned 1:1 to receive daraxonrasib (300 mg orally once daily) or chemotherapy (gemcitabine plus nab-paclitaxel, modified FOLFIRINOX, FOLFOX, or liposomal irinotecan plus fluorouracil and leucovorin). The dual primary endpoints were overall survival (OS) and progression-free survival (PFS) in the RAS G12 mutation subpopulation (91.8% of enrolled patients). Crossover between arms was not permitted.
Results in the RAS G12 population:
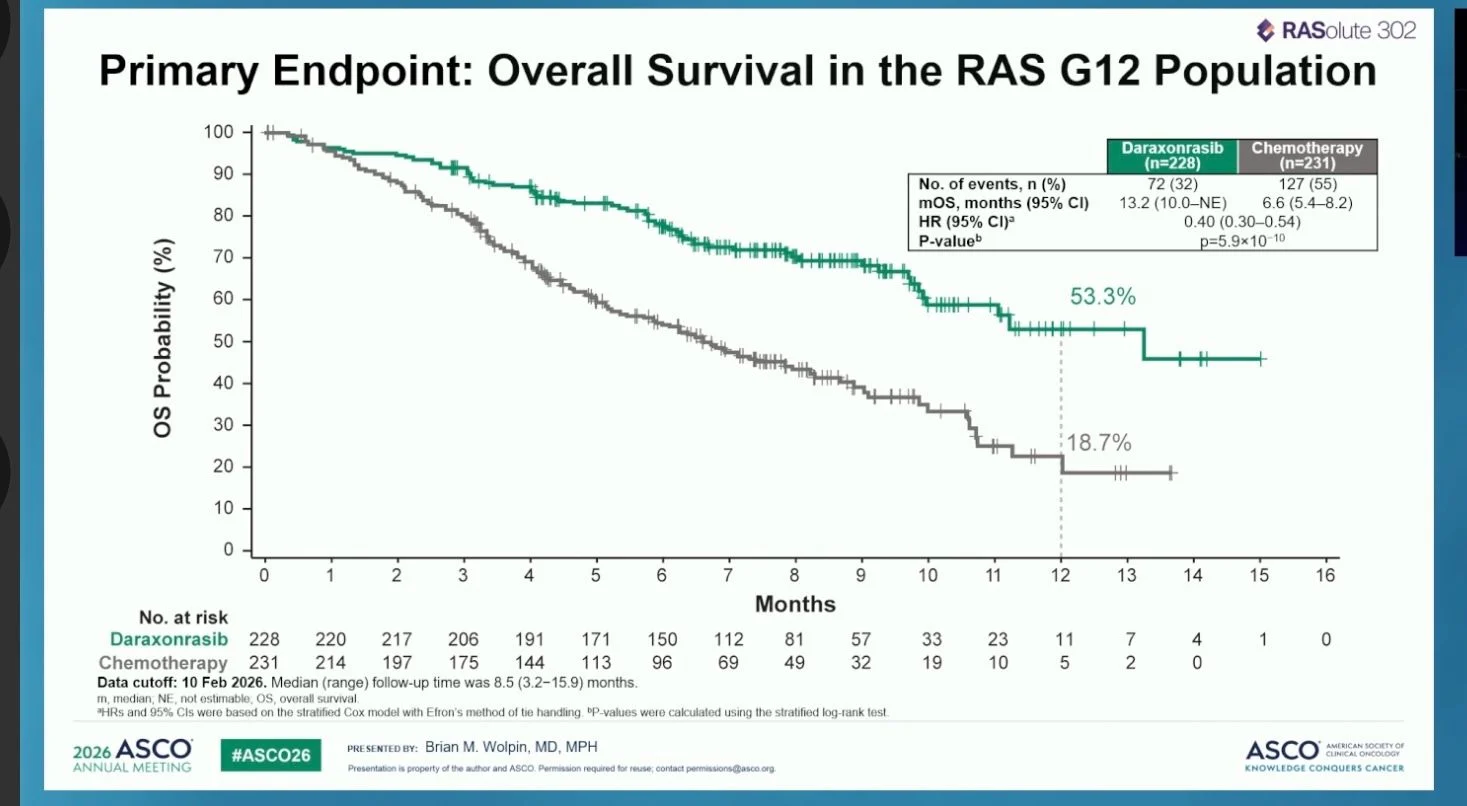
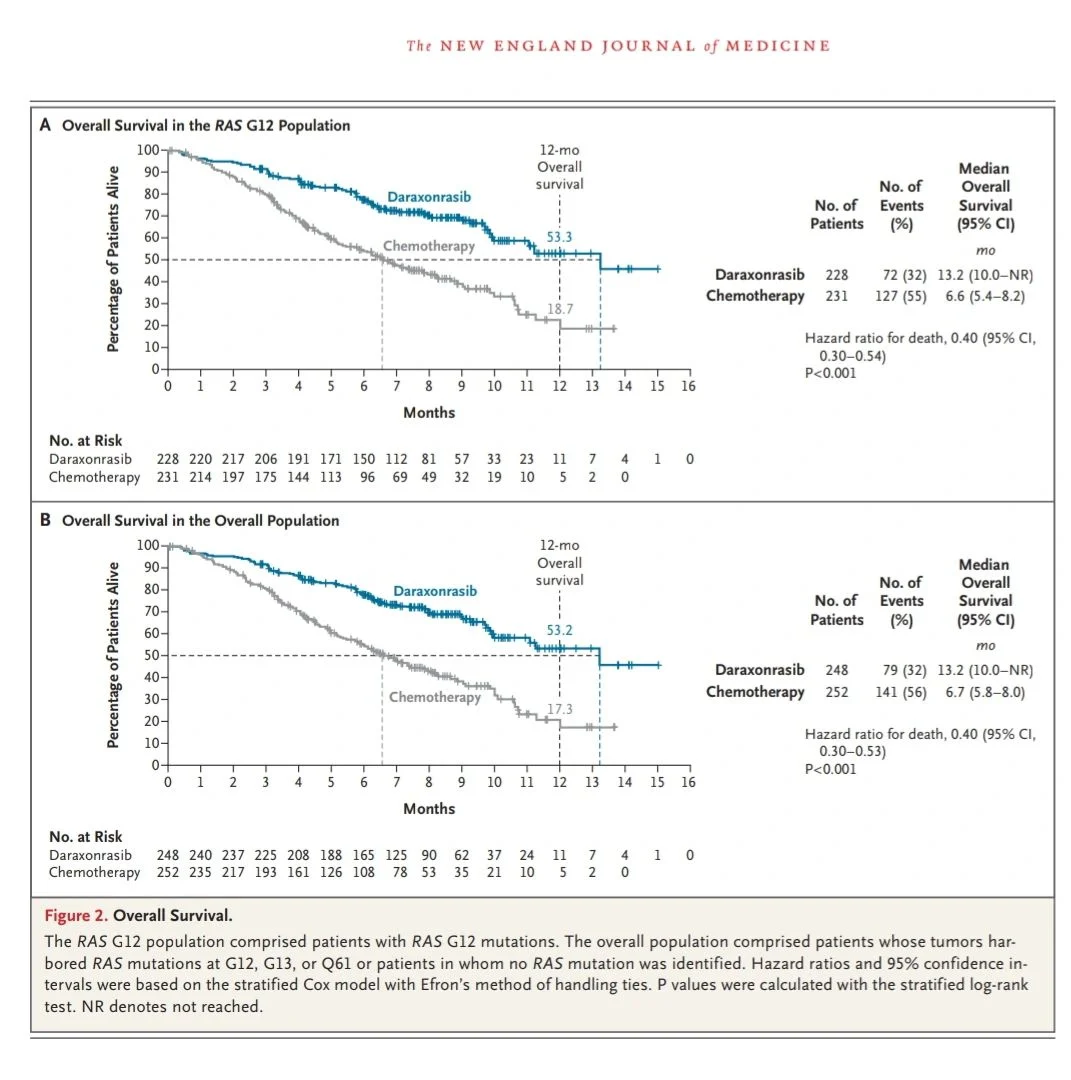
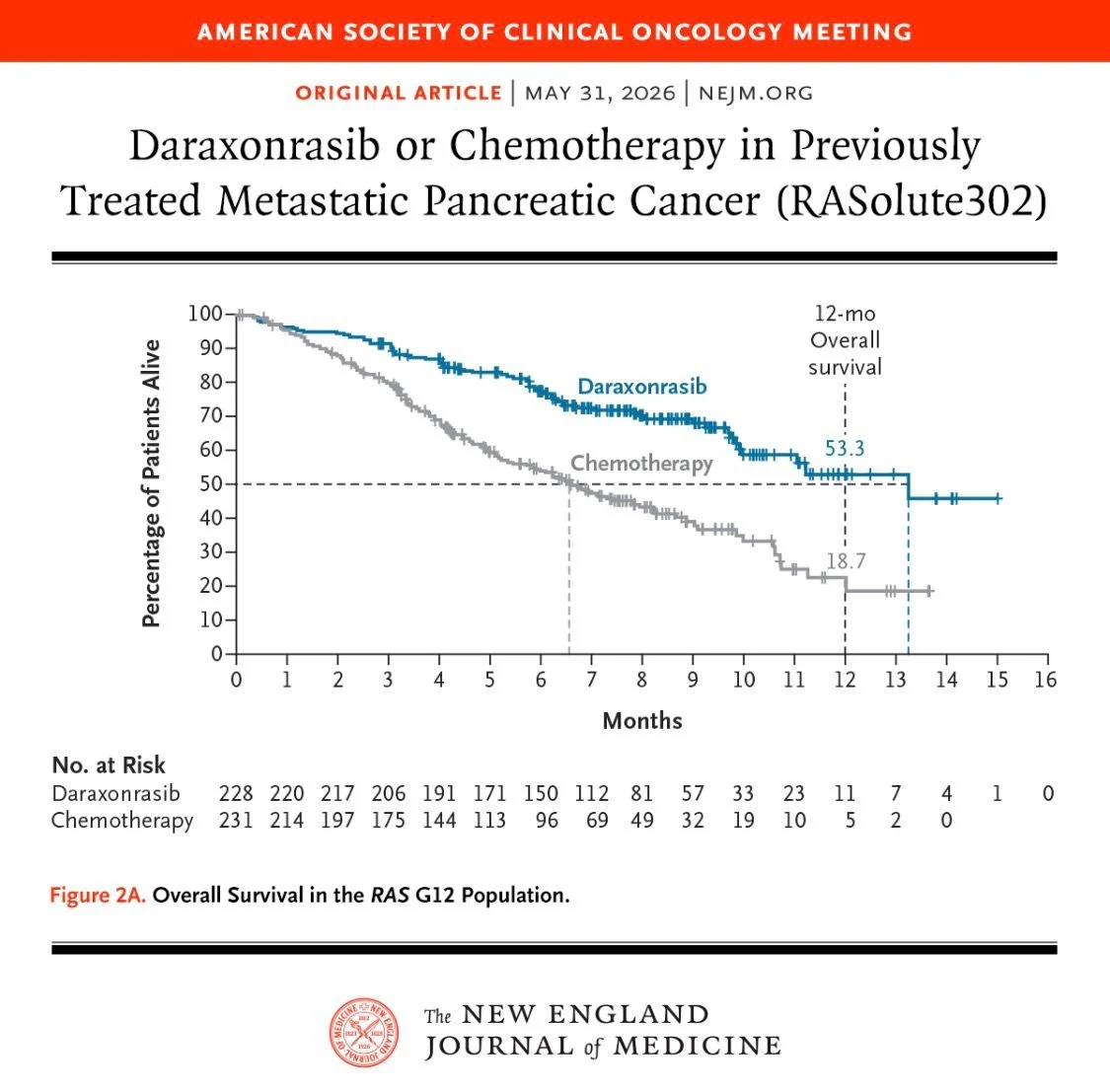
- Median OS – 13.2 months (daraxonrasib) vs. 6.6 months (chemotherapy) – HR=0.40; 95% CI, 0.30 to 0.54; P<0.001
- Median PFS – 7.3 months (daraxonrasib) vs. 3.5 months (chemotherapy) – HR=0.45; 95% CI, 0.34 to 0.59; P<0.001
- Objective response rate – 33.2% (daraxonrasib) vs. 11.8% (chemotherapy)
- 12-month OS rate – 53.3% (daraxonrasib) vs. 18.7% (chemotherapy)
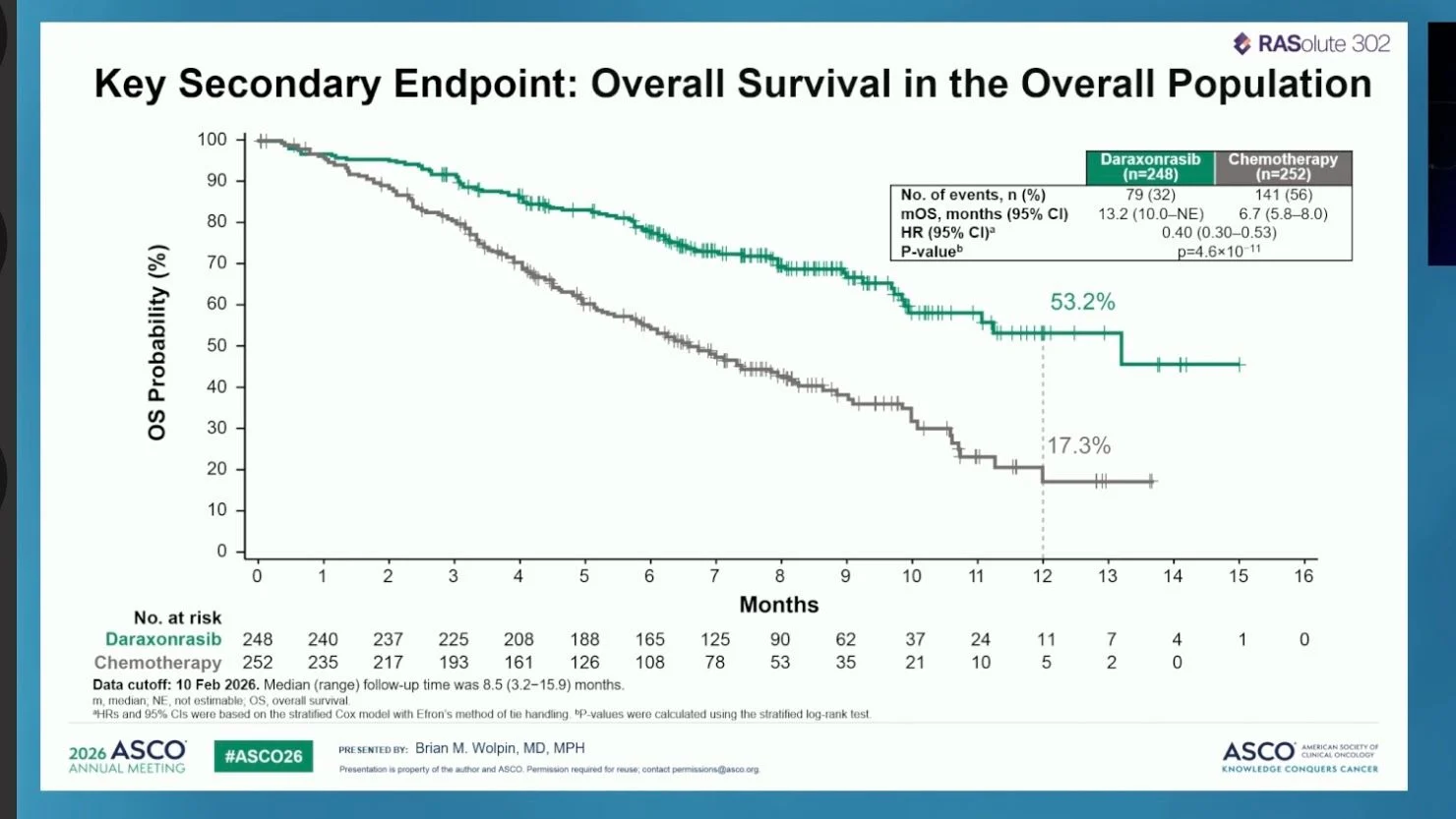
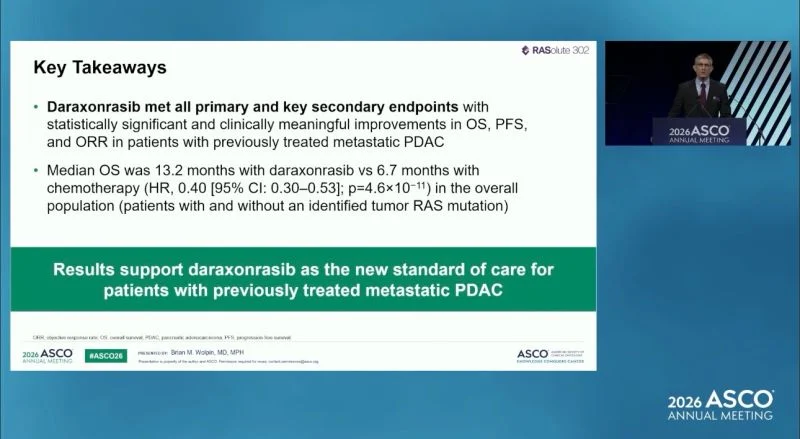
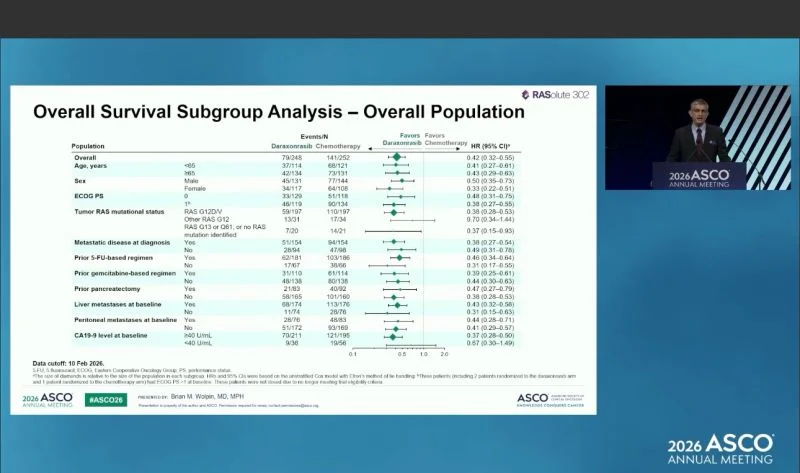
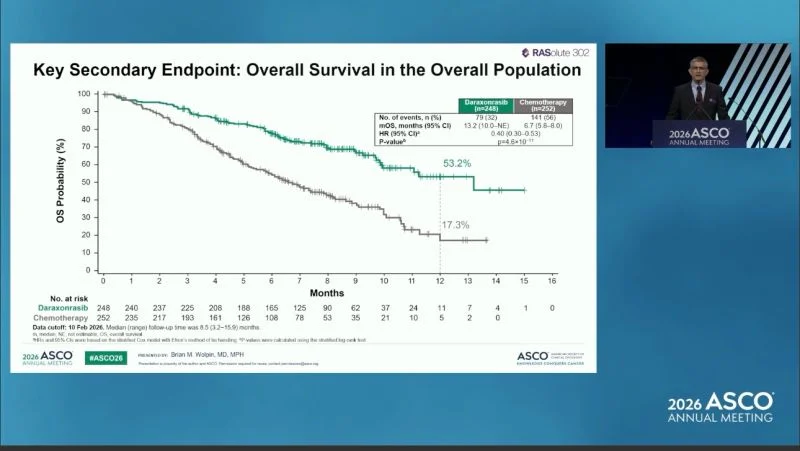
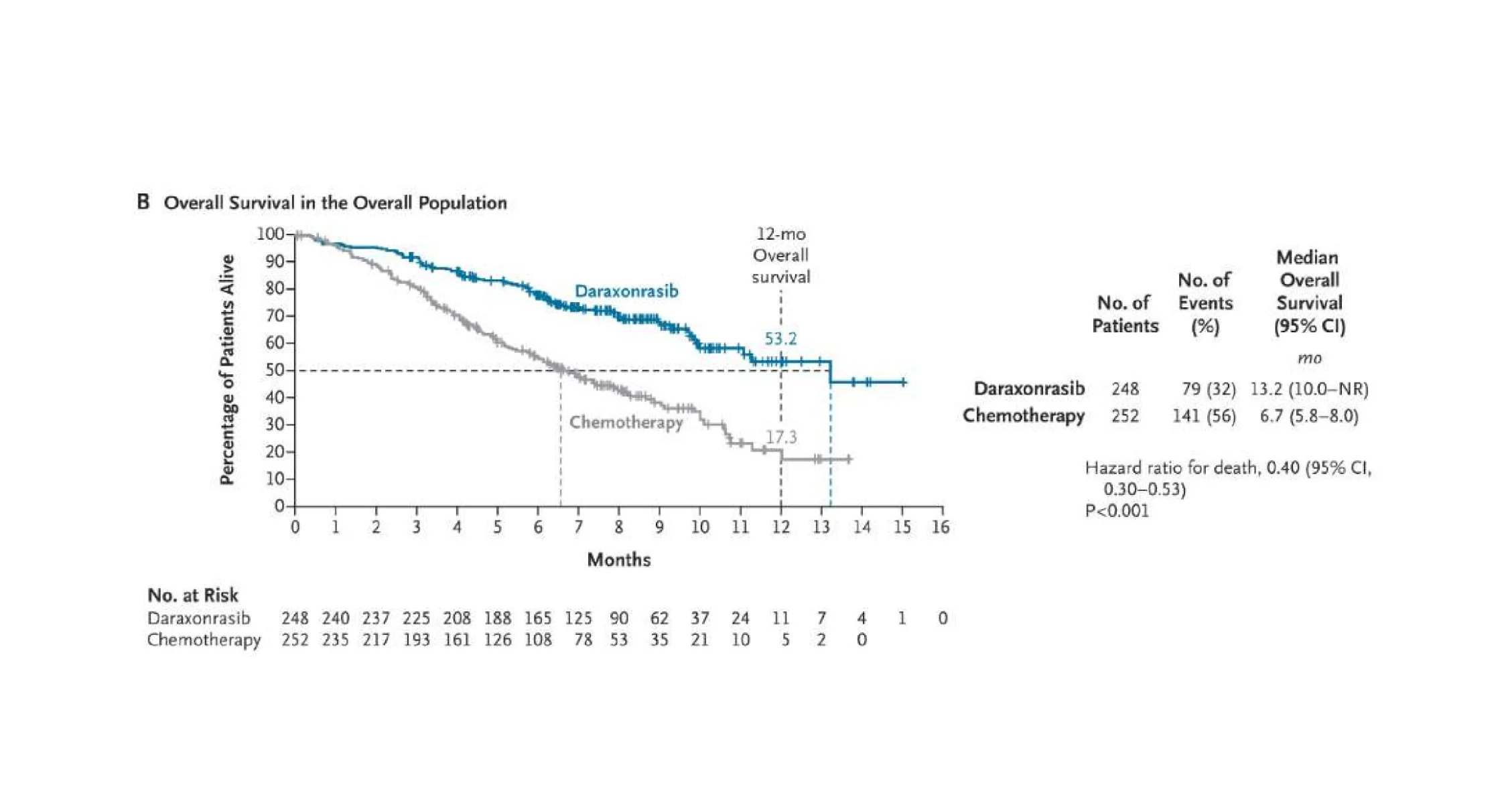
Results in the overall population were virtually identical (HR for OS=0.40; HR for PFS=0.49; P<0.001 for both).
Patient-reported outcomes also favored daraxonrasib, with significantly longer time to deterioration in pain (9.0 vs. 3.7 months; HR=0.51; P<0.001) and global health status–quality of life (5.6 vs. 2.4 months; HR=0.60; P<0.001).
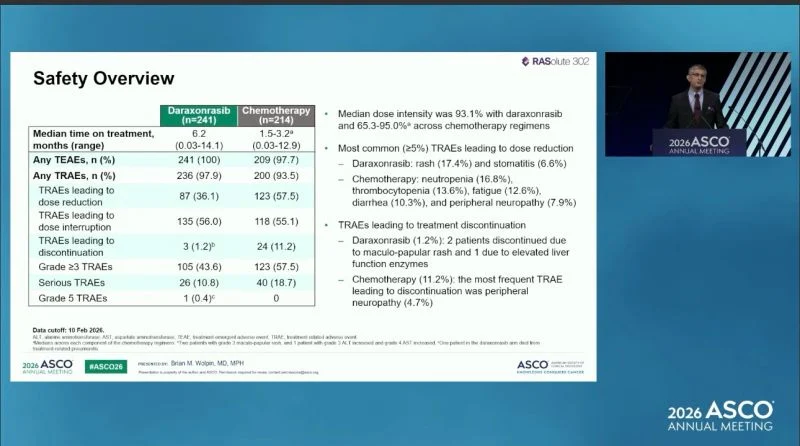
Safety Profile:
Grade ≥3 adverse events – 61.8% (daraxonrasib) vs. 69.6% (chemotherapy)
Treatment-related discontinuation – 1.2% (daraxonrasib) vs. 11.2% (chemotherapy)
Most common daraxonrasib-related events: rash (85.5%), diarrhea (58.1%), stomatitis (53.1%) – predominantly low-grade
Chemotherapy-related events of note: neutropenia (38.3%), anemia (39.7%), peripheral neuropathy (25.2%)
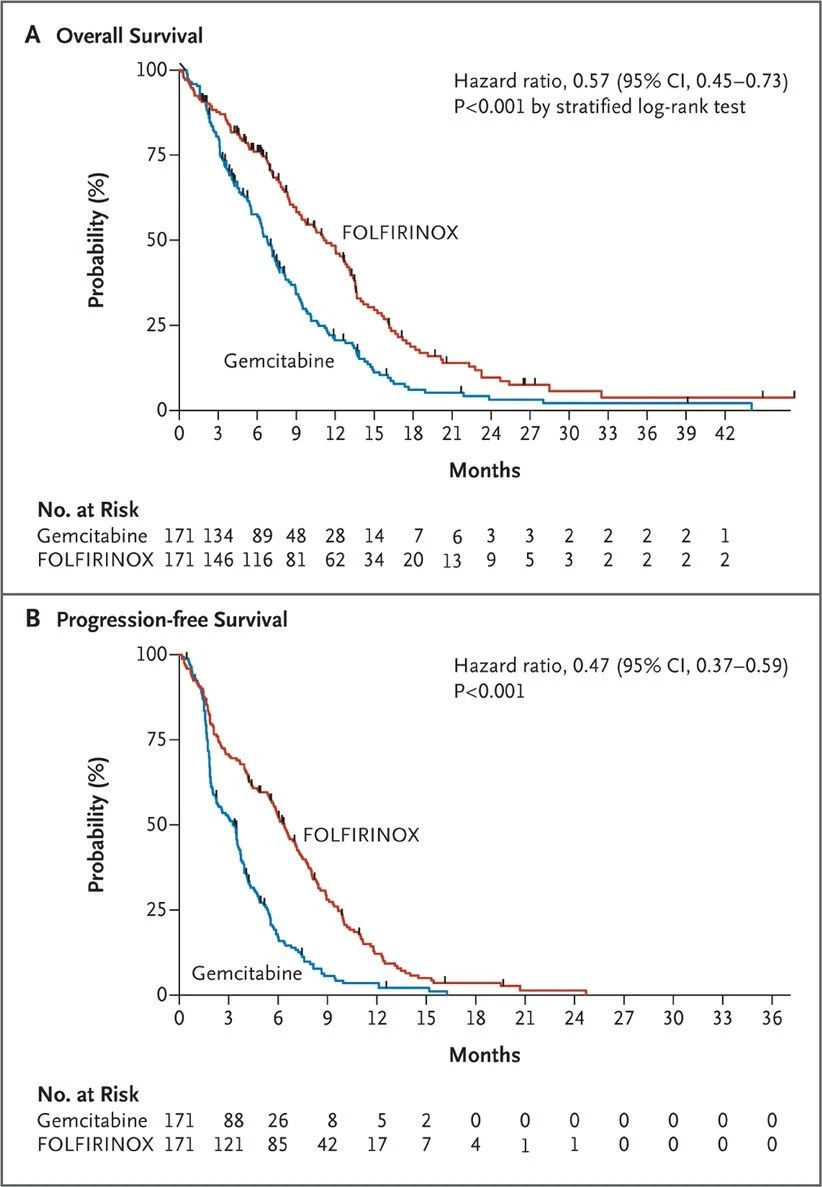
Fifteen years ago, FOLFIRINOX shook the ground in PDAC treatment, allowing a huge improvement in survival compared to gemcitabine (43% reduction in the risk of death). Over the years, we have experienced almost no clinically significant progress. Now we have a new, active targeted treatment dedicated to approximately 90% of PDAC patients – those harboring RAS mutations, while the remaining 10% of RAS wild-type cases are known to carry a better prognosis. Let’s hope that the approval process will go smoothly and that in less than 12 months the drug will be available for our patients.”
Lorenza Rimassa
“Standing ovation for RASolute302 of daraxonrasib in second-line PDAC at ASCO26 plenary session.
Finally a practice changing trial for patients with advanced PDAC. Now we need daraxonrasib in clinical practice soon!”

Rachna Shroff
“A truly monumental day for pancreatic cancer patients and clinicians!”
Thank you NBC News for spotlighting these game changing results from #ASCO26! Kudos to the entire RASOLUTE-302 team – tears of joy were shed today!”
Pashtoon Kasi
“ASCO26
Honored and excited to have contributed to the study at City of Hope. More options for our patients in an unprecedented way!
What was also very heartening was the rapid improvement in cancer related symptoms and rapid fall of markers (19-9/ctDNA).
History in the making. Important landmark and milestone accomplished. This news is beyond an option for patients with pancreas cancer in the 2nd line setting.”

Nicholas DeVito
“A desperately needed win for patients with pancreatic cancer, a disease which has seen drug failure after drug failure in trials, now with a monotherapy that doubles overall survival vs chemo.”
Now we need to make sure we get daraxonrasib to those who need it as soon as possible. RevMed’s EAP does just that, but requires a lot of lifting on the part of oncology clinics to get things up and running. Every center needs someone to lead this effort, and given the patient need, it is not efficient to complete one by one.
Enter Emily Bolch and the newly minted Duke Pancreatic Cancer Center who have moved towards making institutional access to daraxonrasib a reality – at a rapid pace. I am proud to call her a colleague and to be a part of the efforts to prioritize access for our patients Duke Cancer Institute.”
Sarah Cannon Research Institute
“A powerful moment at ASCO26 for pancreatic cancer research. SCRI contributed to the research.
As Meredith Sellers Pelster, Associate Director, Gastrointestinal Cancer Research for SCRI, shared:
“The standing ovation says it all – we finally have an advancement for patients with pancreatic cancer. Daraxonrasib, a multi-selective RAS inhibitor, doubles overall survival for previously treated metastatic pancreatic cancer patients compared to standard chemotherapy, giving tremendous hope to people with this disease.”
For a disease that has seen limited progress over decades, these findings mark an important step forward – offering both extended survival and renewed hope for patients and families.”
Devika Das
“Practice changing! What a memorable plenary and journey for RAS!
Can’t wait for the lcsm data/trials now! This is why our patients with all cancers deserve precision medicine and access to clinical trials!”

Julius Chapiro
“Amazing moment and the applause goes to the trial investigators, the patients but let’s not forget Revolution Medicines and their scientists, business managers and the clinical trial office who made this possible as well.”
It took the power of free market enterprise, unshackled and unmitigated capitalism, entrepreneurial spirit, and the power and will of the American economy and innovation spirit to achieve such results.
This is huge!”
Nabil Ismaili
“Exciting results from ASCO26 – Daraxonrasib (pan-RAS inhibitor) meaningfully improved outcomes vs chemotherapy in previously treated metastatic pancreatic ductal adenocarcinoma (mPDAC):
- Overall survival (RAS G12 population): 13.2 vs 6.6 months (HR 0.40, P<0.001)
- Progression-free survival: 7.3 vs 3.5 months (HR 0.45)
- Objective response rate: 31.6% vs 11.2%
- Quality of life: Significantly longer time to deterioration in pain and global health status
- Safety: Fewer grade ≥3 AEs (61.8% vs 69.6%), much lower treatment discontinuation due to AEs (1.2% vs 11.2%)
Conclusion: Daraxonrasib doubles survival, improves QOL, and has a better tolerability profile, establishing it as the new standard of care for previously treated mPDAC with RAS G12 mutations (>90% of patients).”

Yüksel Ürün
“This is not simply a new pancreatic cancer drug.”
Daraxonrasib met all primary and key secondary endpoints in previously treated mPDAC, with median OS 13.2 vs 6.7 months vs chemo.
A hard target is becoming a real therapeutic path.”

Santiago Fontes
“ASCO Plenary Session; RAS is no longer UN-DRUGGABLE
For decades, RAS was considered the archetypal “undruggable” target, representing one of the greatest challenges in oncology.
Today, that paradigm has shifted
The presentation of the RASolute trial at the ASCO Annual Meeting 2026 highlights the remarkable progress being made in targeting RAS-driven cancers and further reinforces the transition from therapeutic nihilism to precision medicine; specially in pancreatic cancer!!
While resistance mechanisms and patient selection remain critical challenges, the momentum in RAS-directed therapies is undeniable.
“RAS is no longer undruggable – it is increasingly actionable.”

Bishal Gyawali
“Daraxonrasib data are solid and the standing ovation is well deserved but let’s not celebrate the P-values, please. It’s meaningless to tell you how good a drug it is.”
“You can get even smaller P values with much lousier drugs.”

Yago Garitaonaindia
“A lot of lung. But pancreas won the heart of the audience?”
ASCO26 Plenary day
The uncontested king: RASolute 302
(daraxonrasib, a RAS(ON) inhibitor, vs chemo in pretreated mPDAC)
The one everyone was waiting for this ASCO26.
- mOS 13.2 vs 6.6 mo | HR 0.40
- mPFS 7.3 vs 3.5 mo | HR 0.45
- Discontinuation 1.2% vs 11.2%
mOS is still improvable, and beyond OS the quality-of-life dimension is what matters most here, and that discontinuation gap points in the right direction. Either way, the first real signal in RAS-driven PDAC, with cross-tumor implications looming.

Imad Karam
“In patients with RAS G12–mutant metastatic pancreatic cancer, daraxonrasib doubled median overall survival (13.2 vs 6.6 months) and progression-free survival (7.3 vs 3.5 months) compared with chemotherapy, establishing a potential new second-line standard of care.”

Wafik S. El-Deiry
“A breakthrough advance to help patients with pancreatic cancer. The target is KRAS that for decades has been undruggable. Scientific research made this possible.
For pancreatic cancer given the prevalence of KRAS mutations, this is an extremely impressive result and looks better than the last result 15 years ago showing that FOLFIRINOX improves survival vs Gem/Abraxane. POLO was impressive but only 4-7% have germline BRCA mutations. MSI is only 1-2% and there is no trial done in just pancreatic with ICI therapy. NTRK, Ret, MET or ALK are also very rare in pancreatic cancer.”
“But I would say we have to do better with combinations and in addressing resistance in order to help patients long-term.”

Akshat Jain
“Godzilla of cancer news!”
The fight of metastatic pancreatic cancer patients has for decades been one sided, with odds against them.
With this announcement at American Society of Clinical Oncology (ASCO) history has been made and hope restored.
Disease: Pancreatic Ductal Adeno Carcinoma (most prevalent panceratic maligancy) – a death sentence with limited hope and life expectancy despite conventional chemotherapy.
Drug: Why this Pan-RAS inhibitor Works in PDAC?
- >90% of PDAC has KRAS mutations (predominantly G12D, G12V, G12R) – daraxonrasib targets all of them.
- Overcomes resistance mechanisms:
Secondary KRAS mutations
Wild-type RAS allele amplification
Compensatory NRAS/HRAS activation via RTKs - Exploits oncogene addiction: RAS-driven tumors are highly dependent on RAS signaling, making them vulnerable to direct RAS inhibition
- Tumor Microenvironment (TME) Remodeling
- RAS(ON) inhibitors also reverse immunosuppression in PDAC

Hossam Abdulkhalek
“Meaningful Progress in mPDAC: My balanced Reflections on RASolute‑302
The phase 3 RASolute‑302 study has delivered one of the most significant advances we have seen in the second‑line management of metastatic pancreatic adenocarcinoma. In a disease where progress is often incremental, the demonstration that daraxonrasib can do more than double median overall survival compared with standard chemotherapy represents a meaningful step forward for patients and clinicians alike. The trial reported a median OS of 13.2 months vs 6.6–6.7 months, and a median PFS of 7.2–7.3 months vs 3.5–3.6 months, with consistent benefit across both the RAS G12 cohort and the overall population. Importantly, the safety profile was favourable, with substantially fewer treatment discontinuations due to toxicity. These findings position daraxonrasib as a compelling new option in the 2L setting.
At the same time, it is essential to approach the data with appropriate scientific scrutiny:
- The median follow‑up of 8.5 months limits our understanding of long‑term durability.
- The open‑label design, while mitigated by BICR, still introduces interpretive considerations.
- The observed benefit in RAS‑wild‑type tumours raises important biological questions that merit further mechanistic exploration.
- Broader issues of real‑world applicability, access, and cost‑effectiveness will ultimately shape the impact of this therapy across diverse healthcare systems.
Overall, RASolute‑302 represents a highly encouraging development in a challenging disease area. The results warrant both recognition and continued critical evaluation as we consider how best to integrate daraxonrasib into clinical practice.”

Nicholas Hornstein
“This one is special.
This is the hottest paper of 2026 and potentially in the history of pancreatic cancer.
RASolute 302: Daraxonrasib vs investigator’s choice chemotherapy in previously treated metastatic pancreatic cancer
Abstract LBA5 (soon!)
Presentation: May 31, 2026, 3:21-3:33 PM CDT
For decades, pancreatic cancer has been where good ideas go to die.
We have optimized chemotherapy. We have sequenced chemotherapy. We have celebrated modest gains.
But the central driver of PDAC has always been sitting there in plain sight:
RAS.
More than 90% of pancreatic cancers have oncogenic RAS mutations, and until recently, we had essentially nothing direct to do about it.
Daraxonrasib is an oral RAS(ON) multiselective inhibitor targeting the active GTP-bound state of mutant and wild-type RAS.
And in RASolute 302, it delivered.
Quick hits:
Phase 3 international randomized trial 500 patients with previously treated mPDAC Daraxonrasib vs investigator’s choice chemotherapy
- RAS G12 population
91.8% of patients had RAS G12 mutations - OS in RAS G12 population
13.2 vs 6.6 months
HR 0.40
P<0.001 - OS in overall population
13.2 vs 6.7 months
HR 0.40
P<0.001 - PFS in RAS G12 population
7.3 vs 3.5 months
HR 0.45
P<0.001 - PFS in overall population
7.2 vs 3.6 months
HR 0.49
P<0.001 - 12-month OS
Overall population: 53.2% vs 17.3% - Toxicity matters, but this was not just more efficacy for more toxicity
Grade ≥3 AEs: 61.8% vs 69.6%
TRAEs leading to discontinuation: 1.2% vs 11.2%
This is the kind of survival curve we almost never get to see in pancreatic cancer.
This validates RAS(ON) inhibition in the most RAS-addicted major cancer. It takes a target we have talked about for decades and turns it into a clinically meaningful survival benefit in a randomized phase 3 trial.
The next questions come fast: 1L combinations, maintenance, perioperative disease, sequencing, resistance, toxicity management, and whether this becomes a new backbone.
RAS is here, and it couldn’t have come sooner.”
Mark Lewis
Cheers, chills, and a standing ovation when RASolute 302 showed unprecedented survival on daraxonrasib for patients with progressive pancreatic cancer.
“Seldom do you sense you’re witnessing a historic moment in cancer care but this feels like ras targeting has arrived.”
Benjamin L. Ebert
A major breakthrough was just presented at American Society of Clinical Oncology (ASCO) for the treatment of pancreatic cancer. The Phase 3 clinical trial showed that a new drug, daraxonrasib, more than doubles survival of patients with previously treated metastatic pancreatic cancer, compared to chemotherapy treatment. Not only do these findings have the potential to redefine the standard of care for pancreatic cancer, but they also offer renewed hope for continued advances for patients facing this devastating disease.
The thousands of usually staid oncologists in the audience rose for an emotional standing ovation. New treatments with this magnitude of benefit remain exceedingly rare, and unprecedented for pancreatic cancer, one of the most lethal and difficult to treat cancers.
The results were presented by Brian Wolpin, Dana-Farber Cancer Institute’s Robert T. and Judy B. Hale Chair in Pancreatic Cancer and Director of our Gastrointestinal Cancer Center, who led this clinical trial and presented it in the plenary session of the ASCO meeting. Brian has devoted his career to treating patients with pancreatic cancer and to developing new therapies. The unprecedented findings presented today will benefit patients with pancreatic cancer around the world. This advance shows, once again, how rigorous science and innovative drug development can lead to transformative progress for previously intractable diseases.

Other articles about ASCO on OncoDaily.
Written by Mariam Harutyunyan
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}