


Olubukola Ayodele, Breast Cancer Lead at University Hospitals of Leicester NHS Trust, shared a post on LinkedIn:
““The truth is rarely pure and never simple.” Oscar Wilde’s words captured the mood at this morning’s invasive lobular cancer (ILC) update at SABCS25.
What stood out clearly is how much more we still need to learn about ILC.
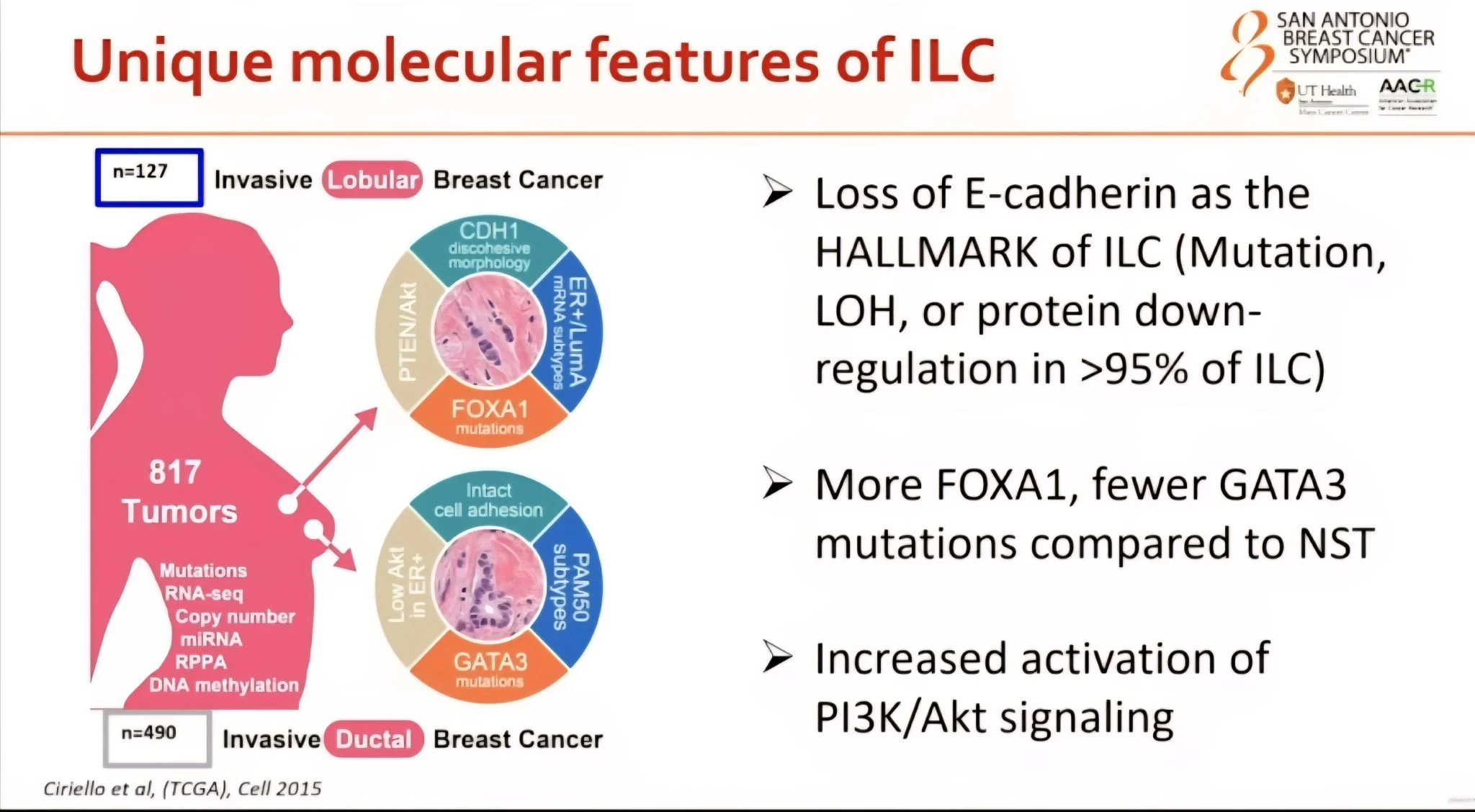
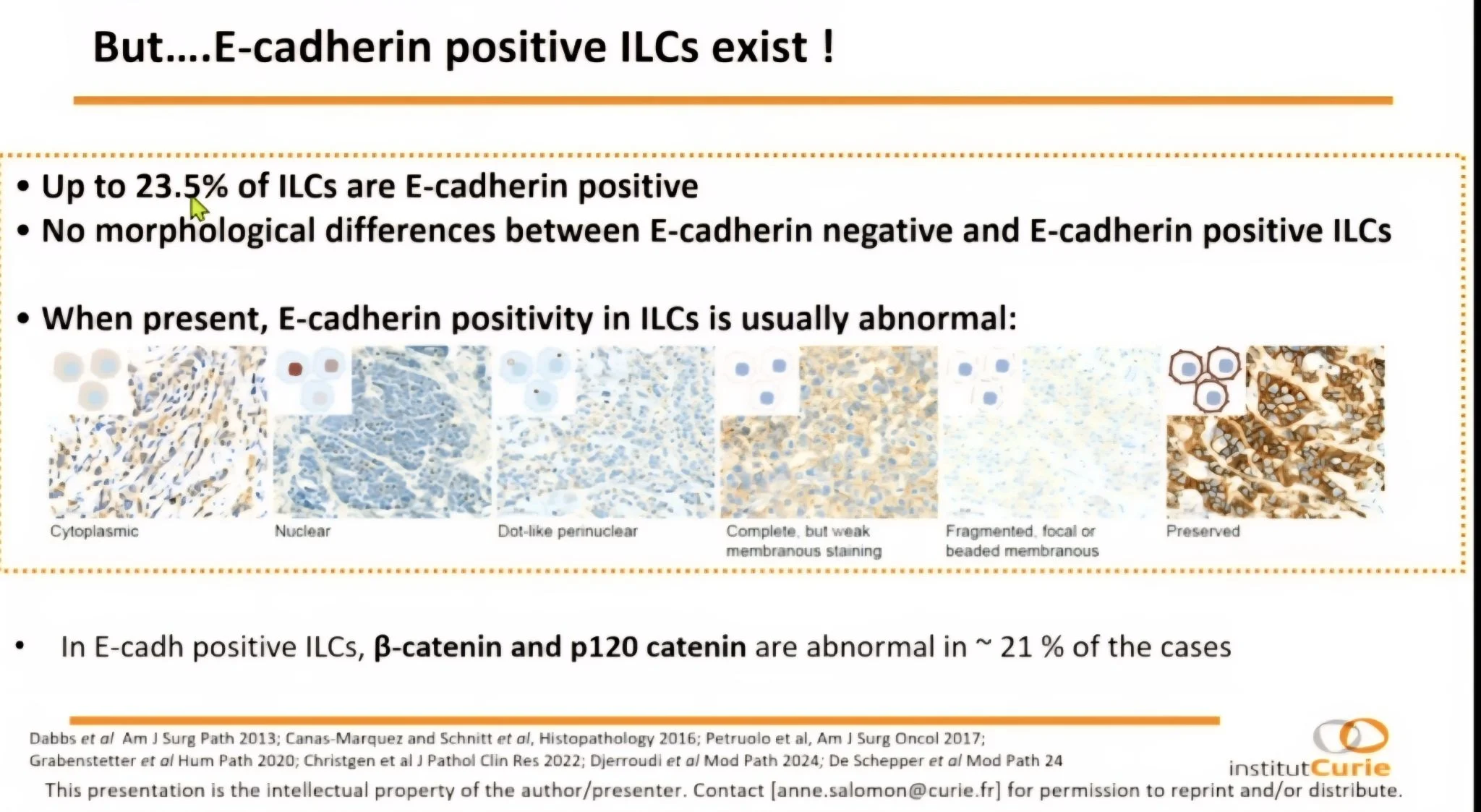
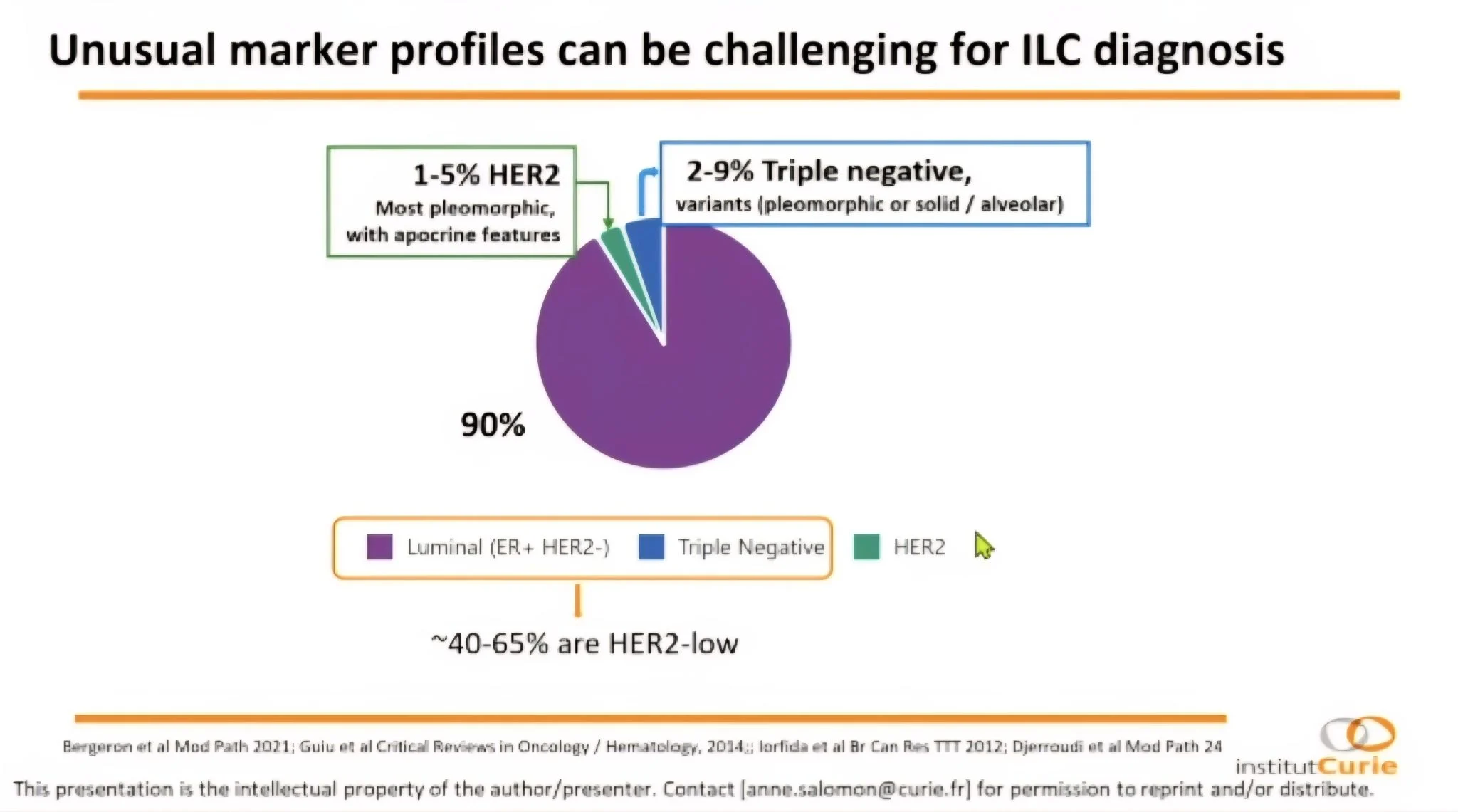
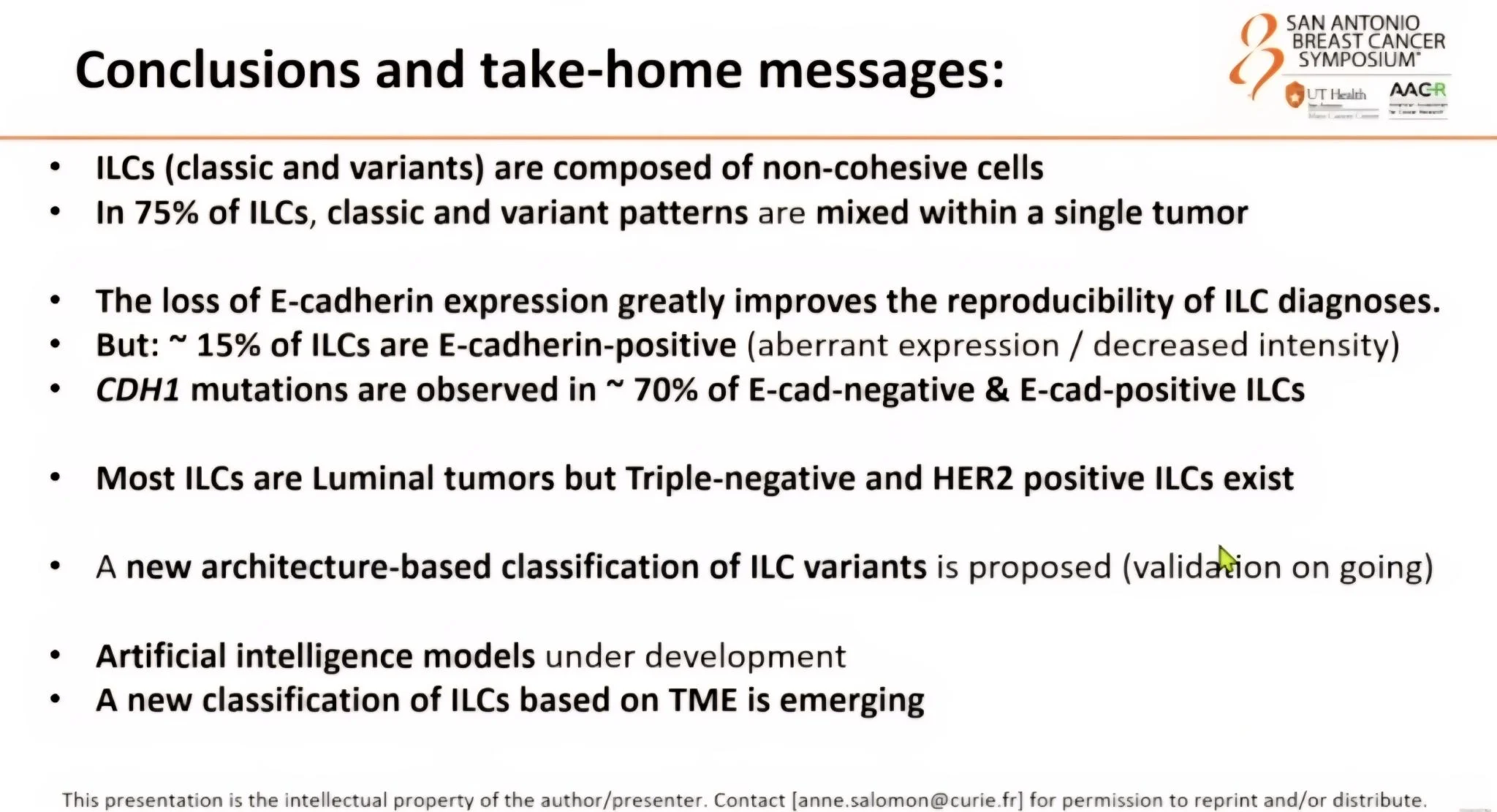
Anne Vincent-Salomon highlighted the ongoing challenges with diagnostic criteria and classification. We often rely on loss of E-cadherin to identify ILC, yet this is present in only about 85% of cases. Around 23.5% may still be E-cadherin positive. Many tumours also show mixed patterns rather than the classical form. While most ILCs are luminal, a small proportion are HER2 positive (1 to 5%) or triple negative (2 to 9%).
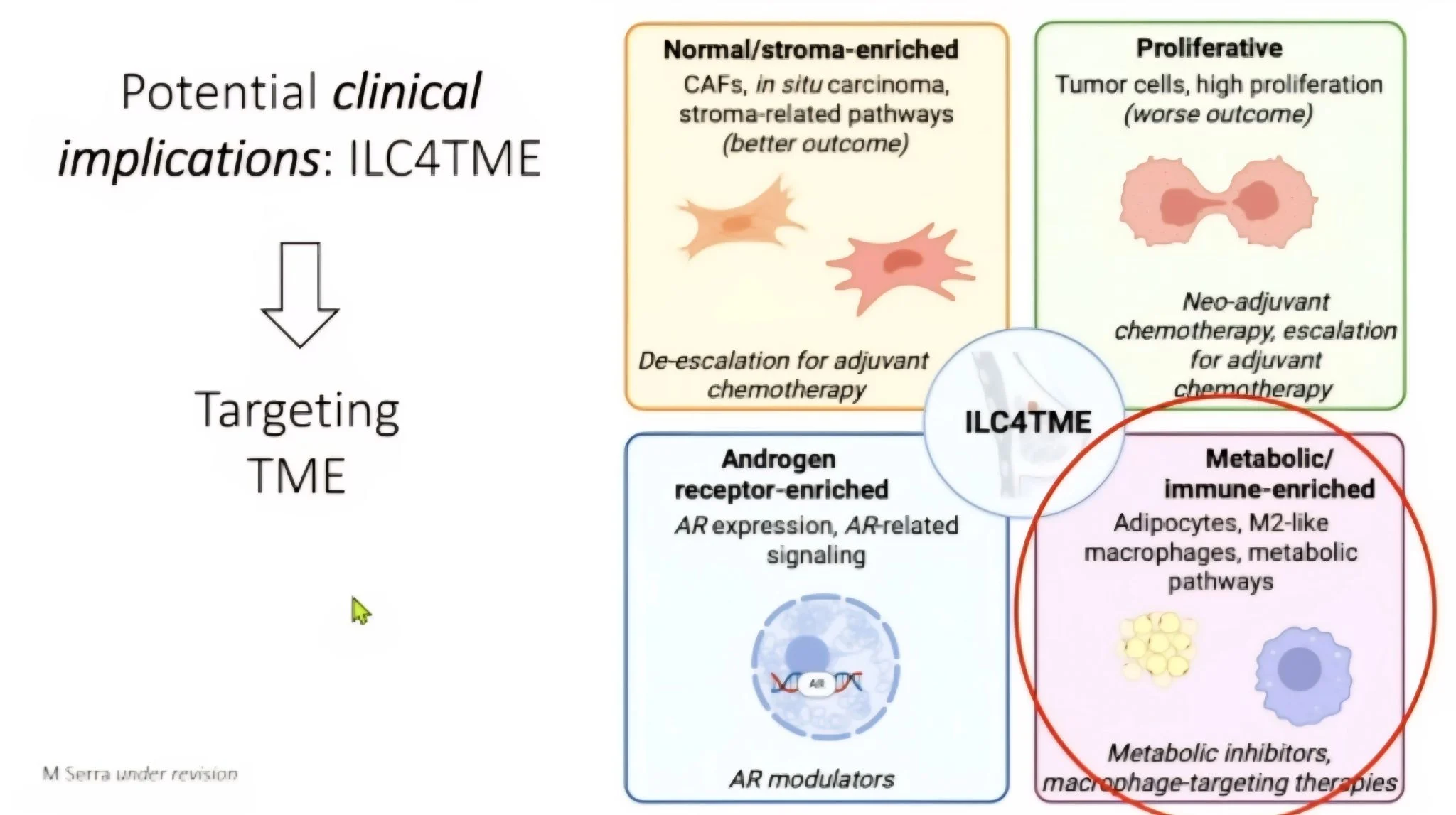
Christos Sotiriou shared four emerging molecular subtypes that could shape future treatment decisions:
1. Normal stroma enriched, associated with better outcomes and possible scope for adjuvant chemotherapy de-escalation.
2. Proliferative, linked to poorer outcomes and likely need for neoadjuvant or adjuvant chemotherapy.
3. Androgen receptor enriched, opening the door for AR-targeted therapies.
4. Metabolic immune enriched, often seen in younger patients and potentially responsive to macrophage-targeted treatments.
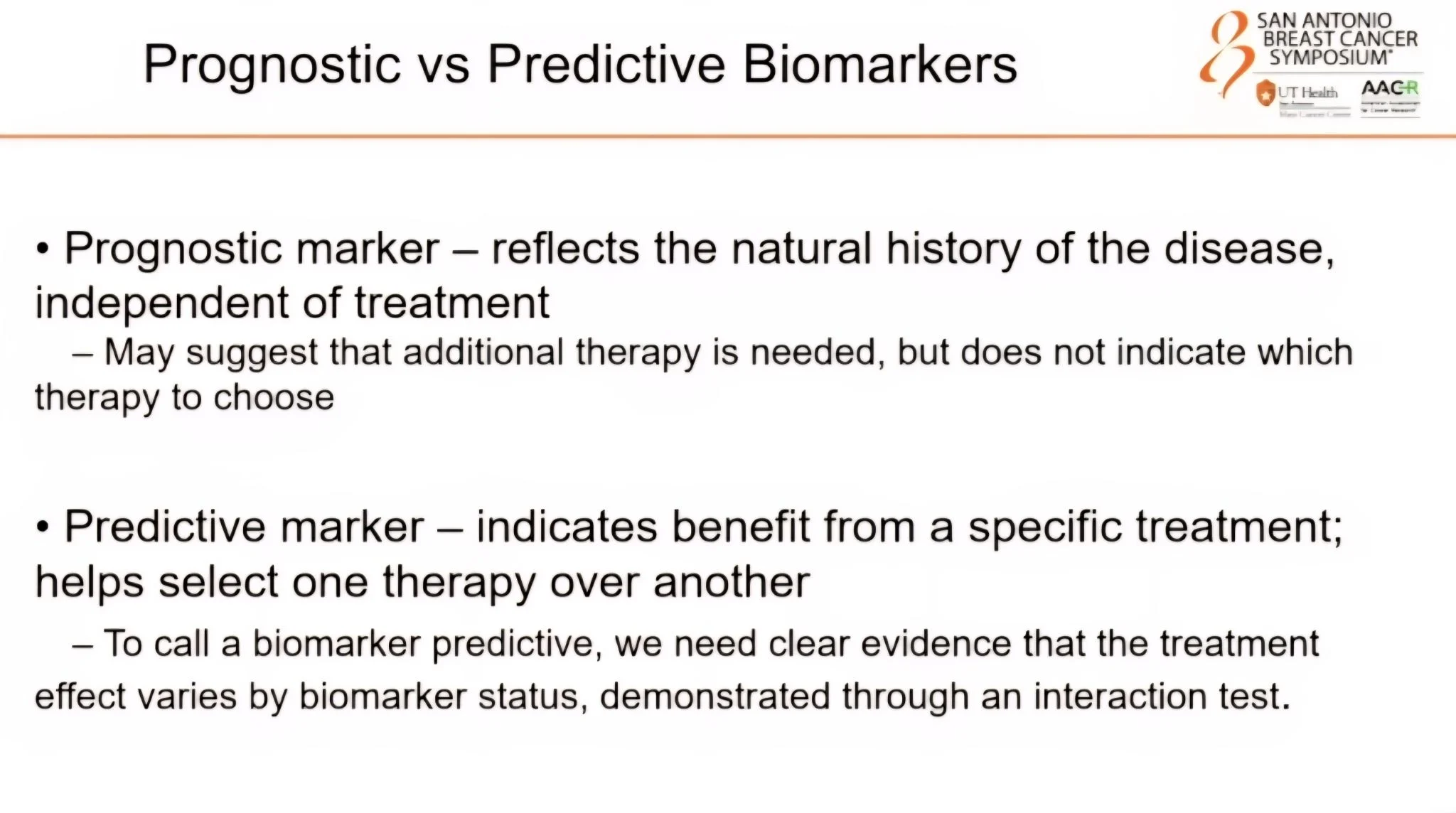
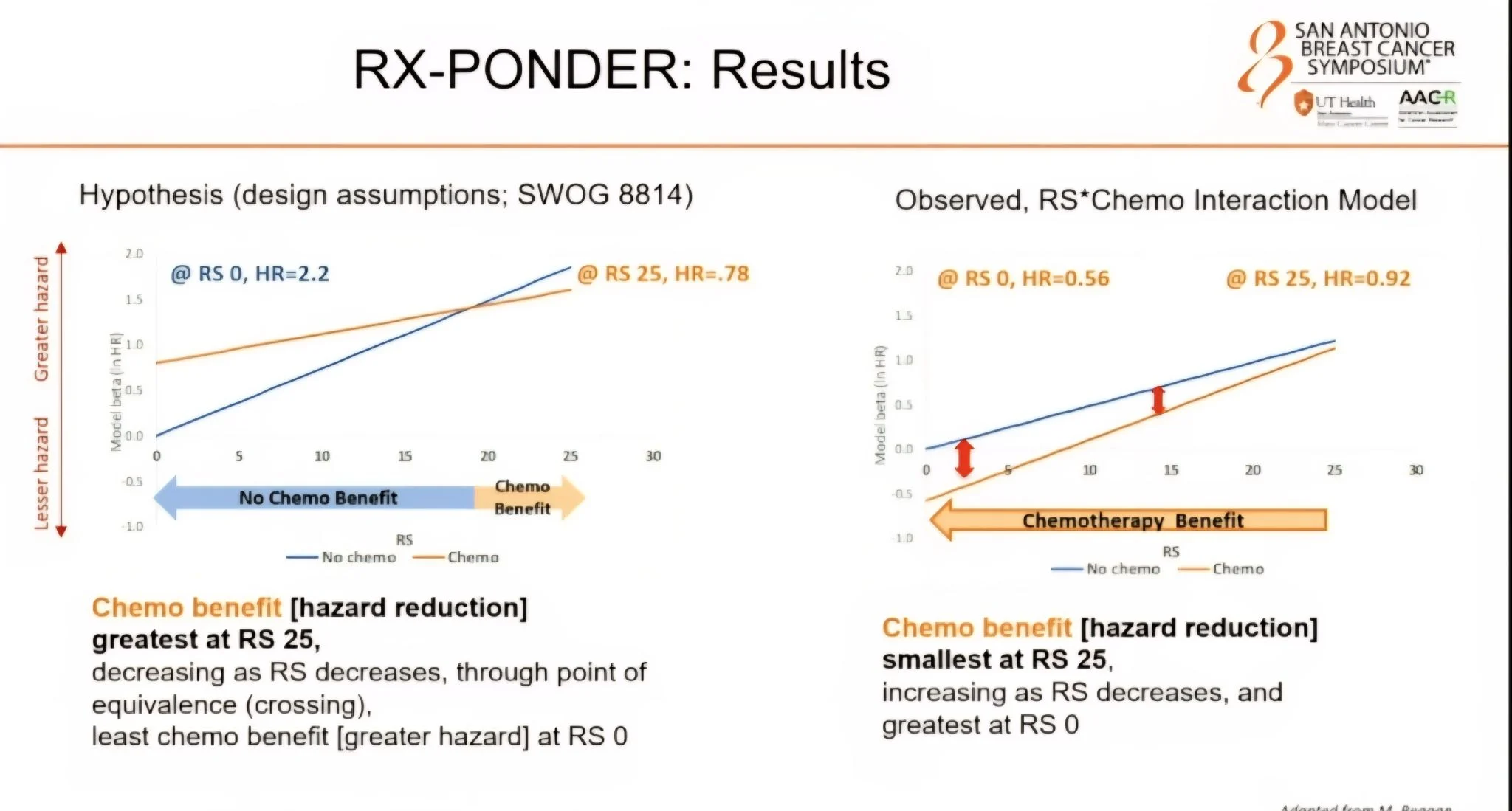
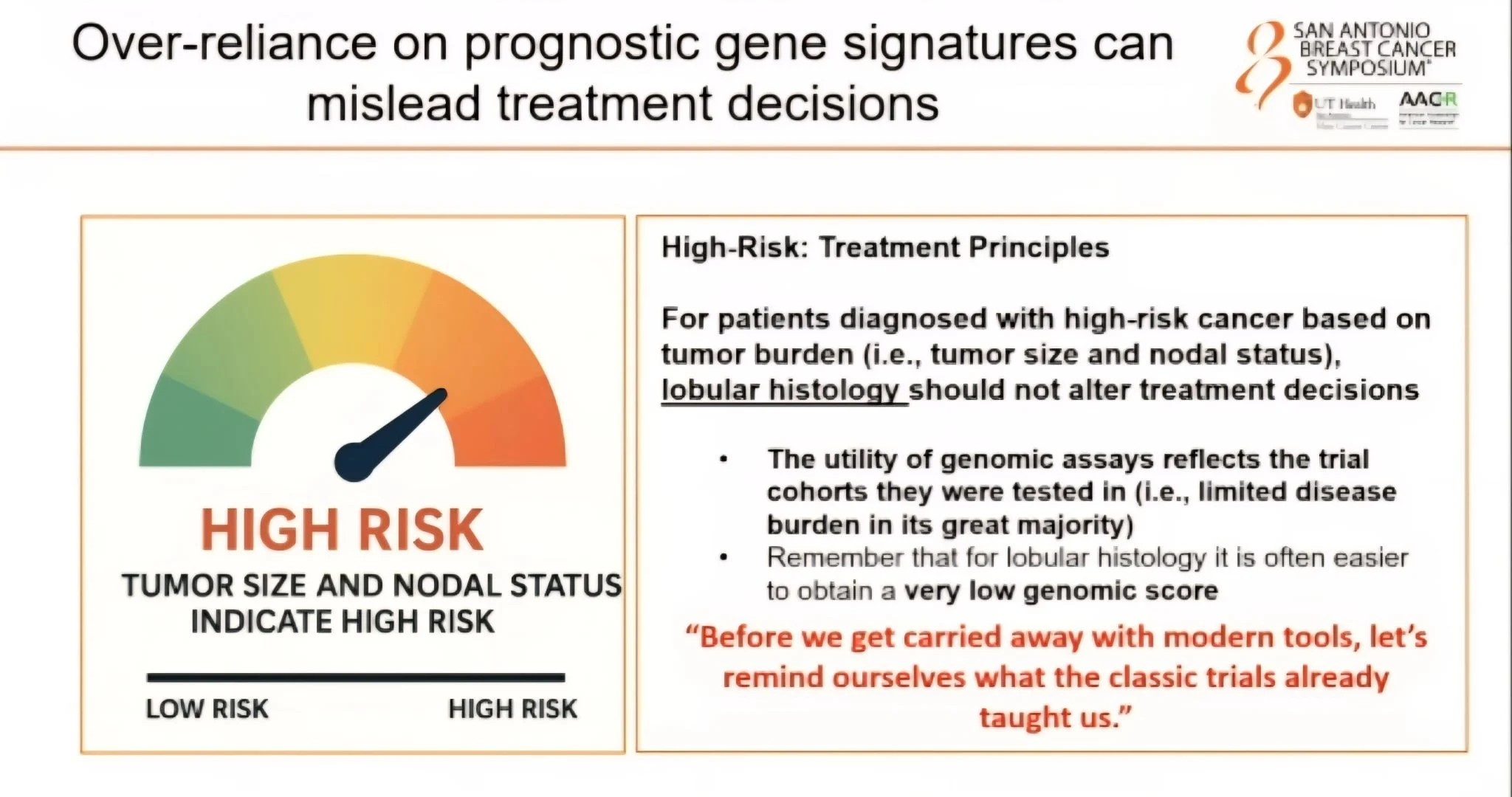
Otto Metzger urged caution when interpreting genomic risk scores in ILC. These tumours are often low grade with low mitotic activity, which can lead to deceptively low recurrence scores. As seen in RxPonder, this creates discordance. The long-held belief that ILC does not benefit from adjuvant chemotherapy needs a closer look. Lobular histology alone should not be used as a reason to omit chemotherapy. The choice of endocrine therapy is also important, as ILC can show resistance to Tamoxifen.
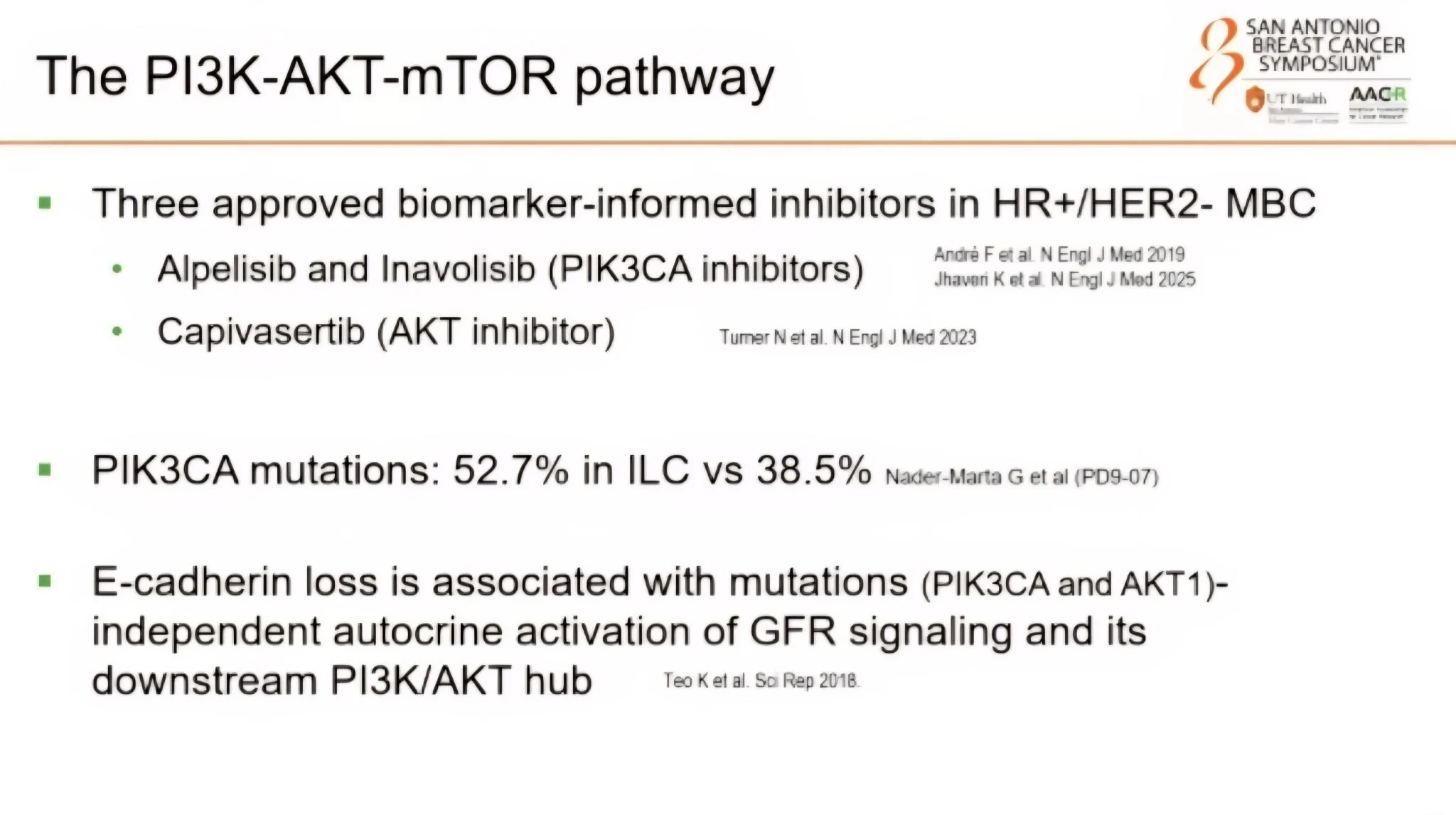
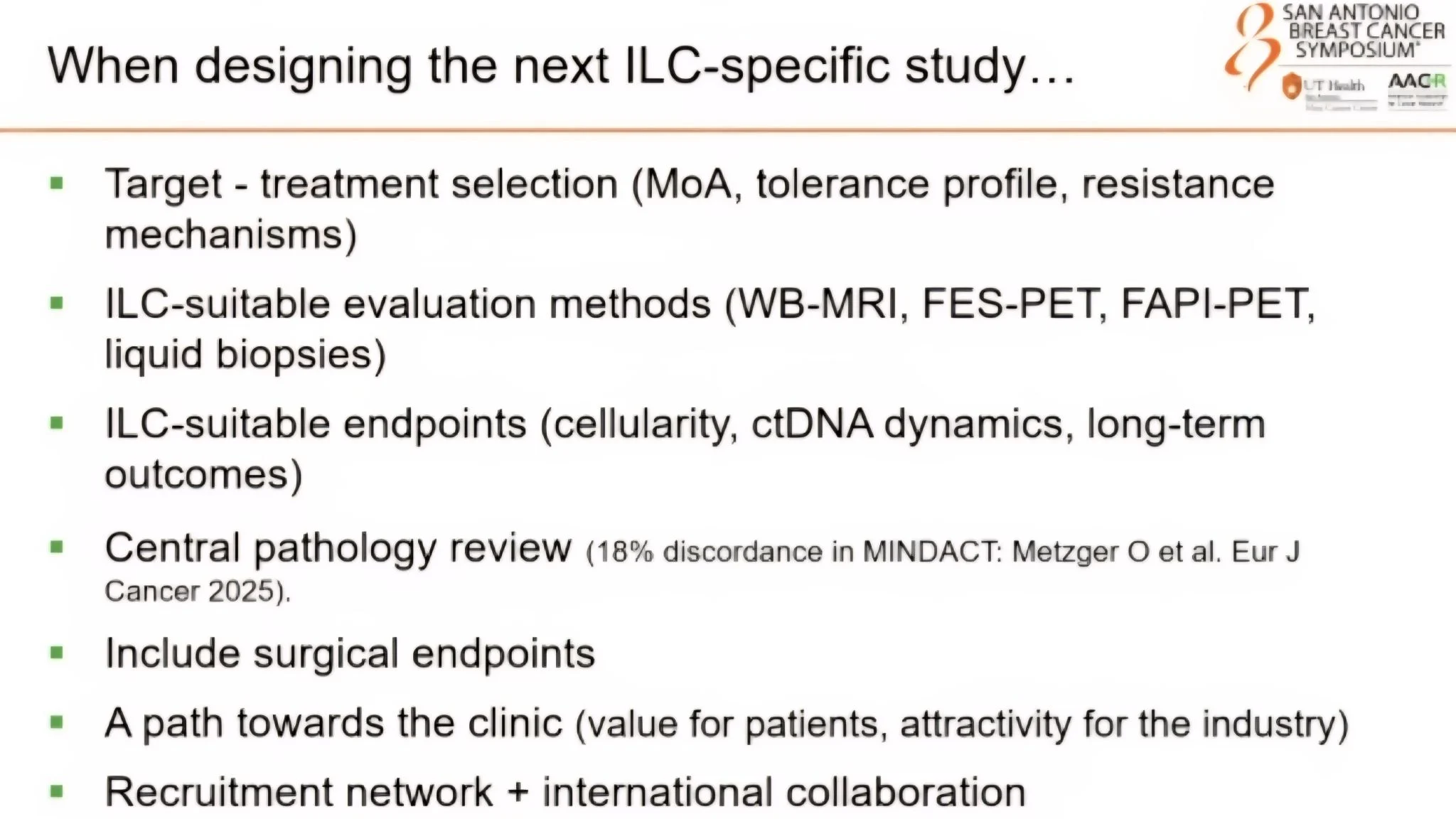
Philippe Aftimos MD noted that loss of E-cadherin is linked with higher rates of PIK3CA and AKT mutations. This is valuable information as we design future ILC-specific trials. He also emphasised the need for better evaluation methods for ILC, such as whole-body MRI for RECIST, central pathology review and more suitable endpoints like ctDNA dynamics and long-term outcomes, given the dormancy often seen in ILC.
The message was unmistakable. Breast cancer is not a single disease. We cannot keep applying a one-size-fits-all approach.
A special mention to the Lobular Breast Cancer Alliance Inc. for ensuring a patient advocate was part of the discussion. Their voice is essential as we work towards better, more personalised care. Thank you Flora Migyanka for being so vulnerable.”

More posts featuring Olubukola Ayodele on OncoDaily.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}