


Liang Cheng, Director of Anatomic Pathology and Director of Molecular Pathology at Lifespan Academic Medical Center, Vice Chair for Translational Research at the Warren Alpert Medical School of Brown University, and President at the International Society of Urological Pathology, shared a post on LinkedIn about a paper he co-authored with colleagues published in Histopathology:
“Is it time for a change after 28 years of stagnation in bladder cancer grading?
In this timely review, ‘Grading of bladder cancer: updates, controversies and practical solutions’, Professor Michelle Downes and colleagues (published this month in Histopathology; PMID: 41384703) comprehensively examine the historical evolution of bladder cancer grading, emerging concepts, and persistent controversies. The authors critically appraise existing grading systems and present compelling evidence supporting alternative, more biologically and clinically relevant approaches to bladder cancer grading.
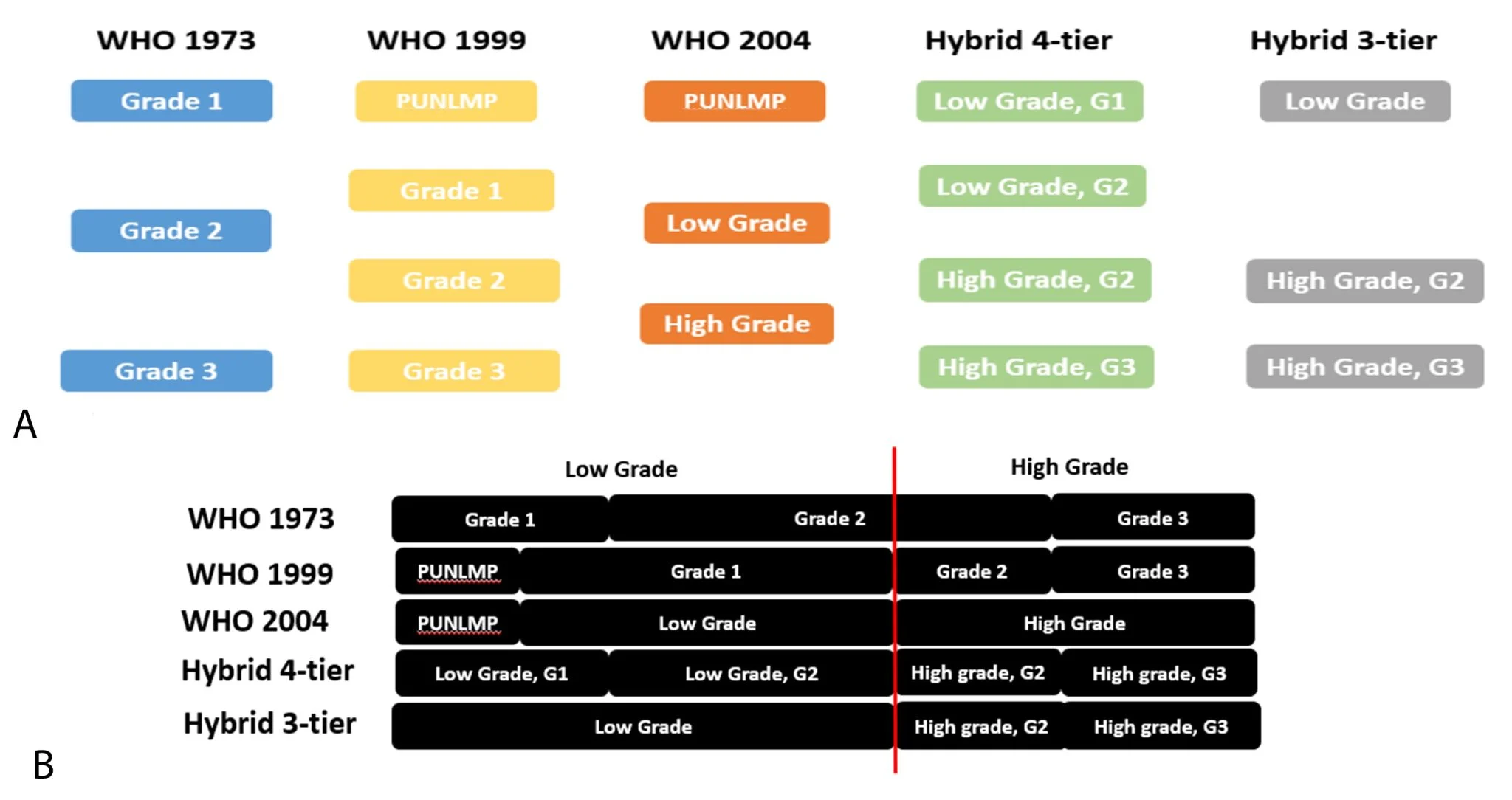
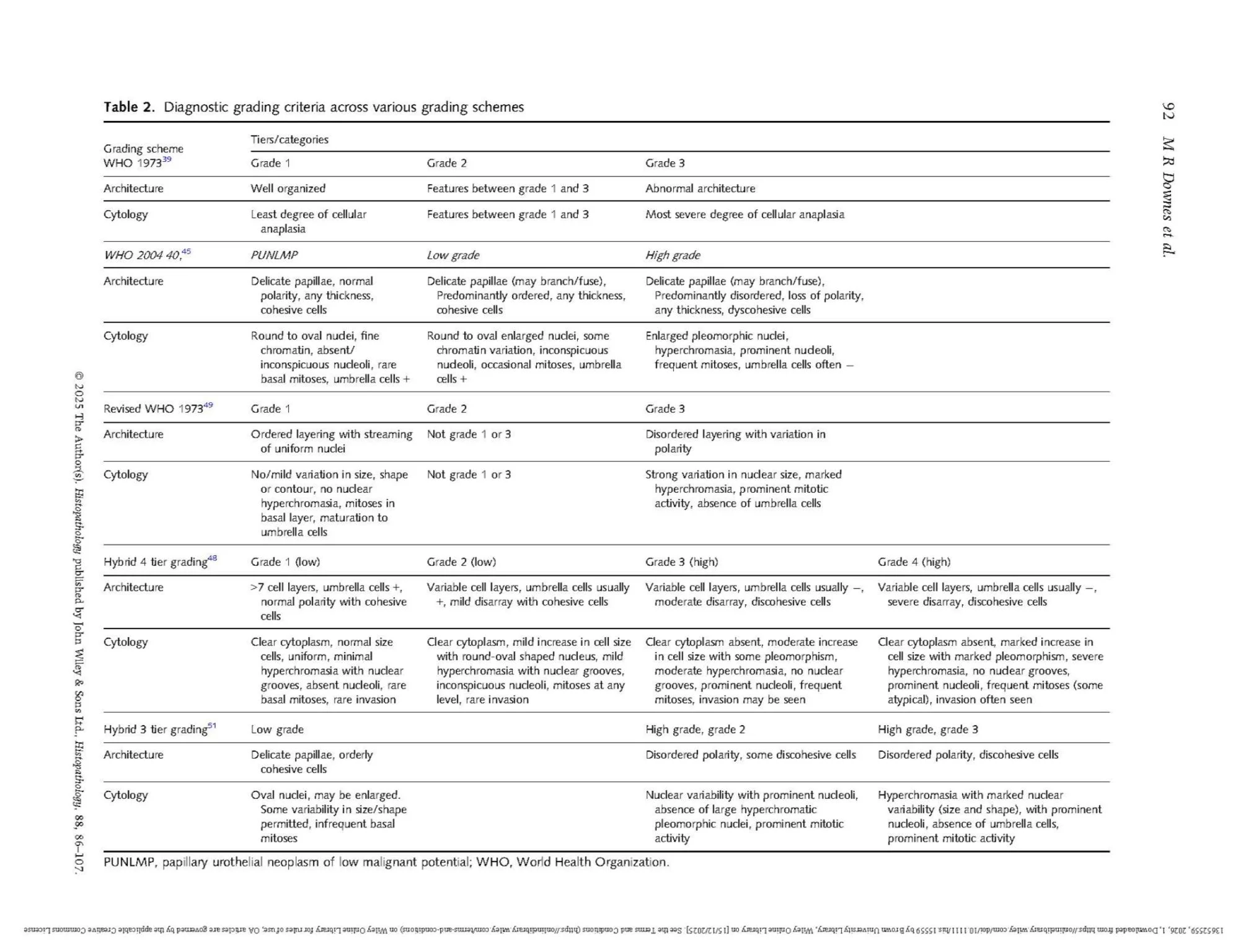
The 1998 International Society of Urological Pathology (ISUP) consensus classification introduced new diagnostic categories for papillary urothelial tumours, notably PUNLMP- which is a topic for another day…Under the WHO 1973 system, still widely used in European countries, many tumours were classified as grade 2 (G2), a heterogeneous group with variable clinical outcomes, limiting prognostic discrimination. While WHO 2004/2022 simplified grading into low- and high-grade categories, it did not fully resolve this issue. All high-grade tumours are grouped together, potentially leading to under- or overtreatment.
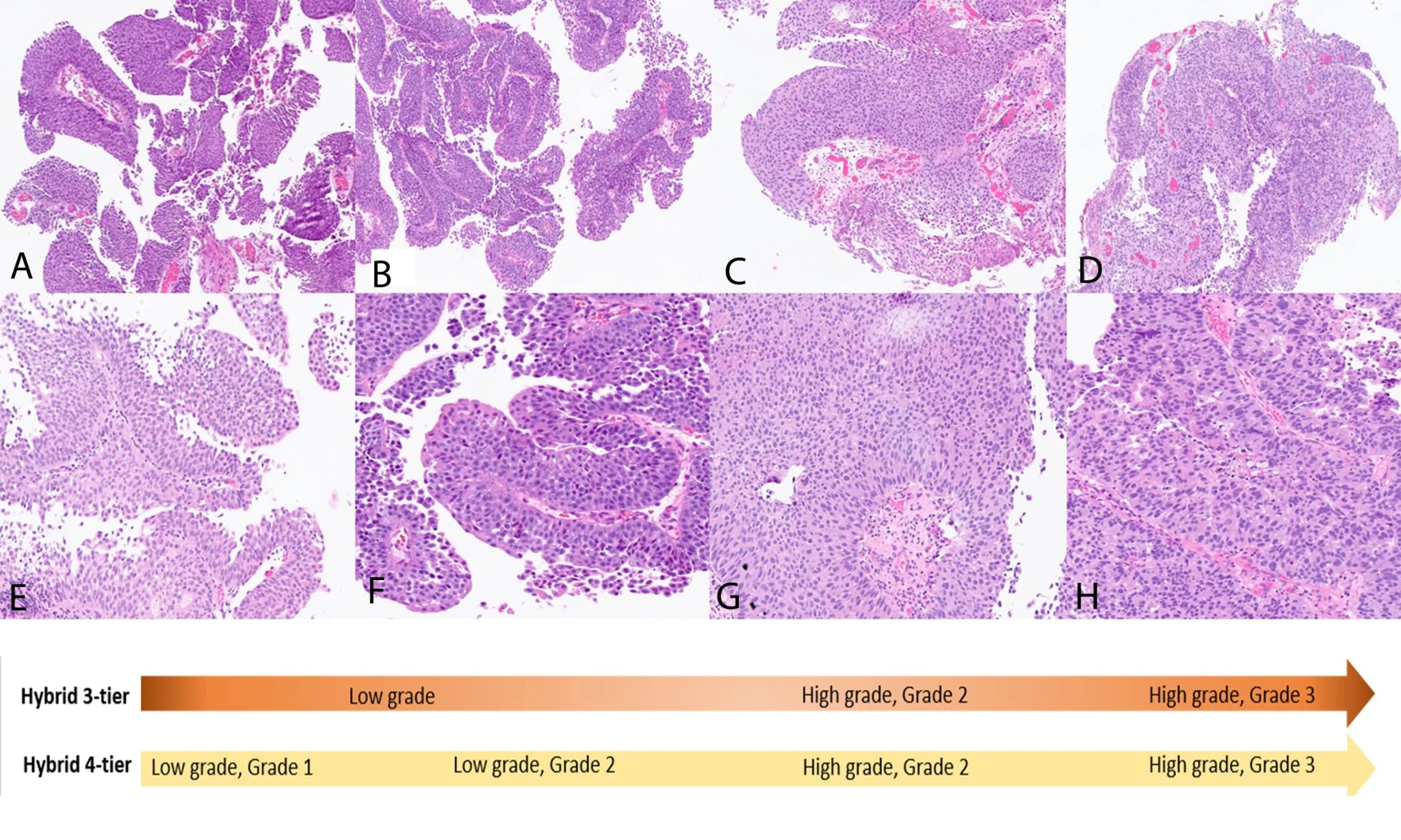
Emerging molecular and clinical outcome data indicate biologically meaningful differences within high-grade tumours. High-grade G3 cancers show distinct molecular profiles and worse clinical behaviour compared with high-grade G2 tumours, which share greater similarities with low-grade disease. These differences are reflected in higher rates and faster time to progression in G3 tumours, in both non-invasive and invasive settings.
There is broad alignment between pathologists and clinicians on the need for improved risk stratification to better guide surveillance and treatment decisions. Debate continues regarding the optimal number of grading tiers. Some advocate a hybrid 4-tier system, subdividing low-grade tumours (with grade 1 encompassing PUNLMP) and splitting high-grade tumours into grades 2 and 3, allowing finer placement along the biological continuum. Others favour a hybrid 3-tier system, which preserves the simplicity of WHO 2004 for low-grade disease while restoring the prognostic discrimination of WHO 1973 by subdividing high-grade tumours.
Survey data from clinicians and voting outcomes from the ISUP Basel Consensus meeting, supported by recent clinical studies, indicate a preference for hybrid 3-tier grading. This approach demonstrates good reproducibility, improved inter-observer agreement, and meaningful clinical stratification, making it a pragmatic and clinically relevant alternative to current grading schemes.
The ISUP Hybrid grading system – particularly the 3-tier model – may therefore represent a logical next step after nearly three decades of relative stagnation in bladder cancer grading.”
Title: Grading of bladder cancer: updates, controversies, and practical solutions
Authors: Michelle R Downes, Theodorus H van der Kwast, Antonio Lopez-Beltran, Liang Cheng
You can read the Full Article in Histopathology.

More posts featuring Liang Cheng.
{kind=link}
{kind=link}
{kind=link}
{kind=link}