


François-Clément Bidard, Head of Center for Clinical Investigation CIC-2501 at Inserm, shared a post on LinkedIn:
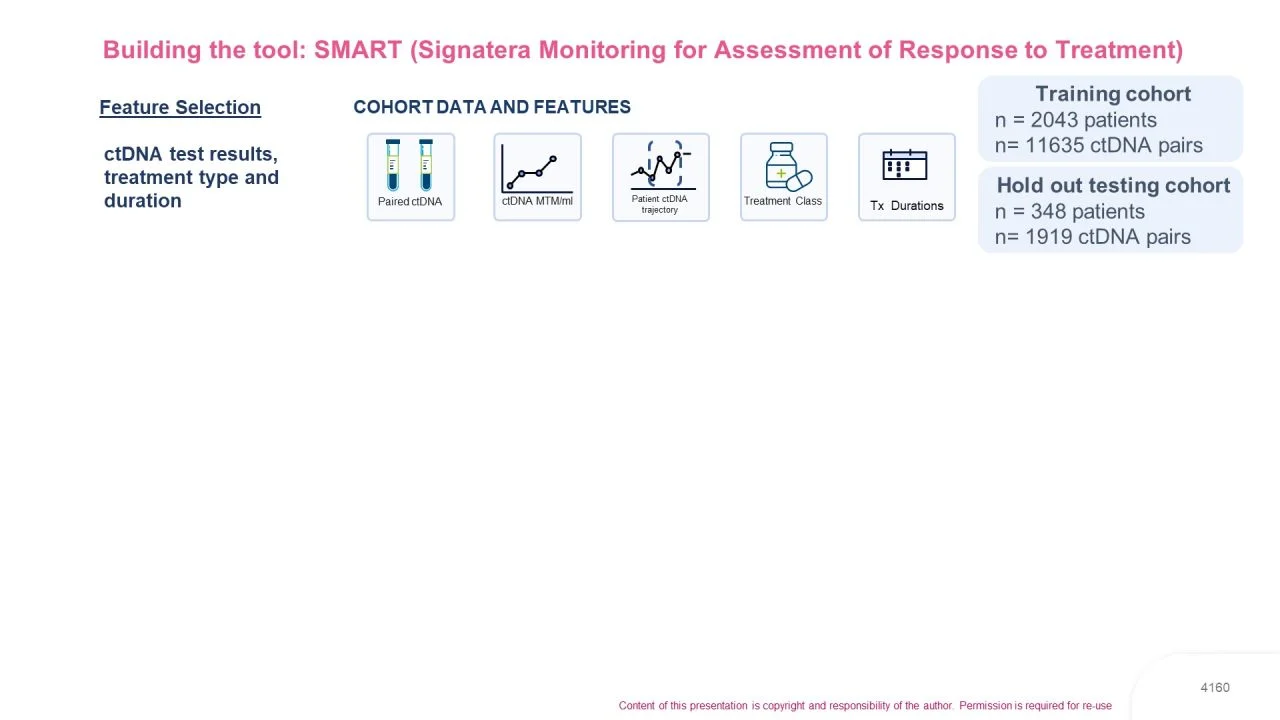
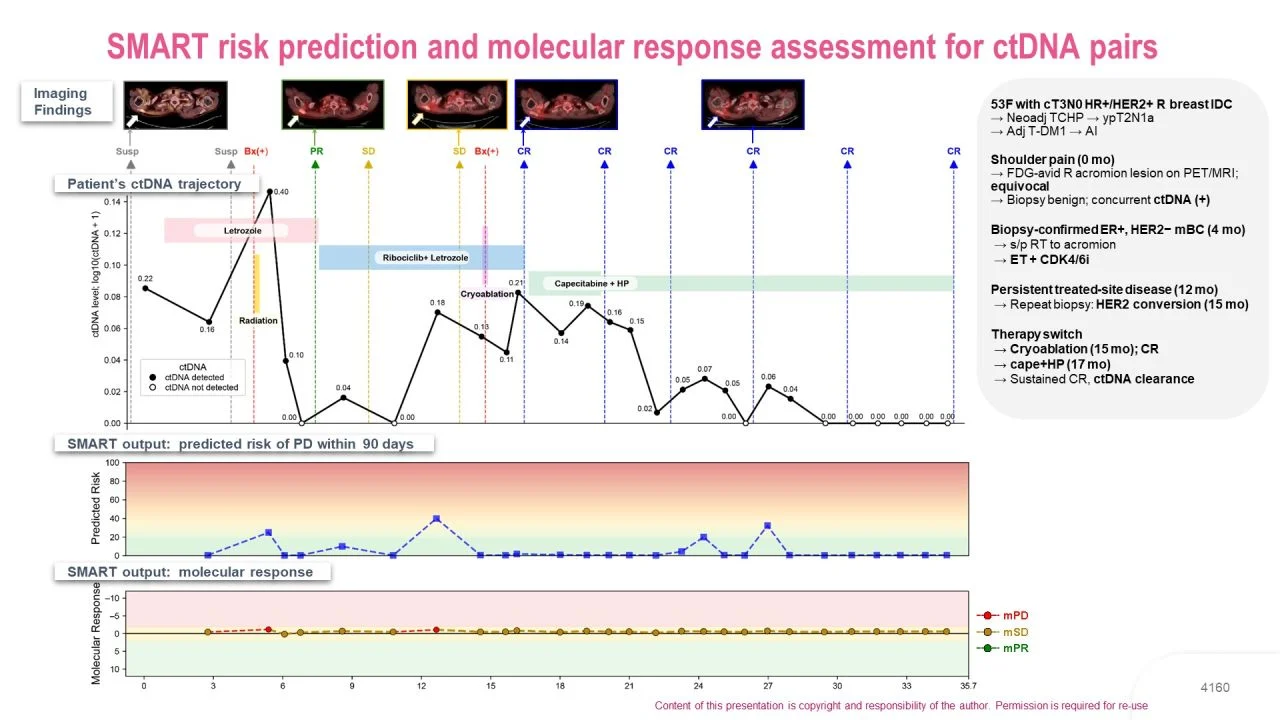
“Slides from a key ctDNA study presented by Pedram Razavi at ESMO Breast 2026 (and me as senior author; proferred paper session). The work is based on data from patients with mBC whose disease was monitored throughout therapy using the Natera WES assay.
Key takeaways (in short):
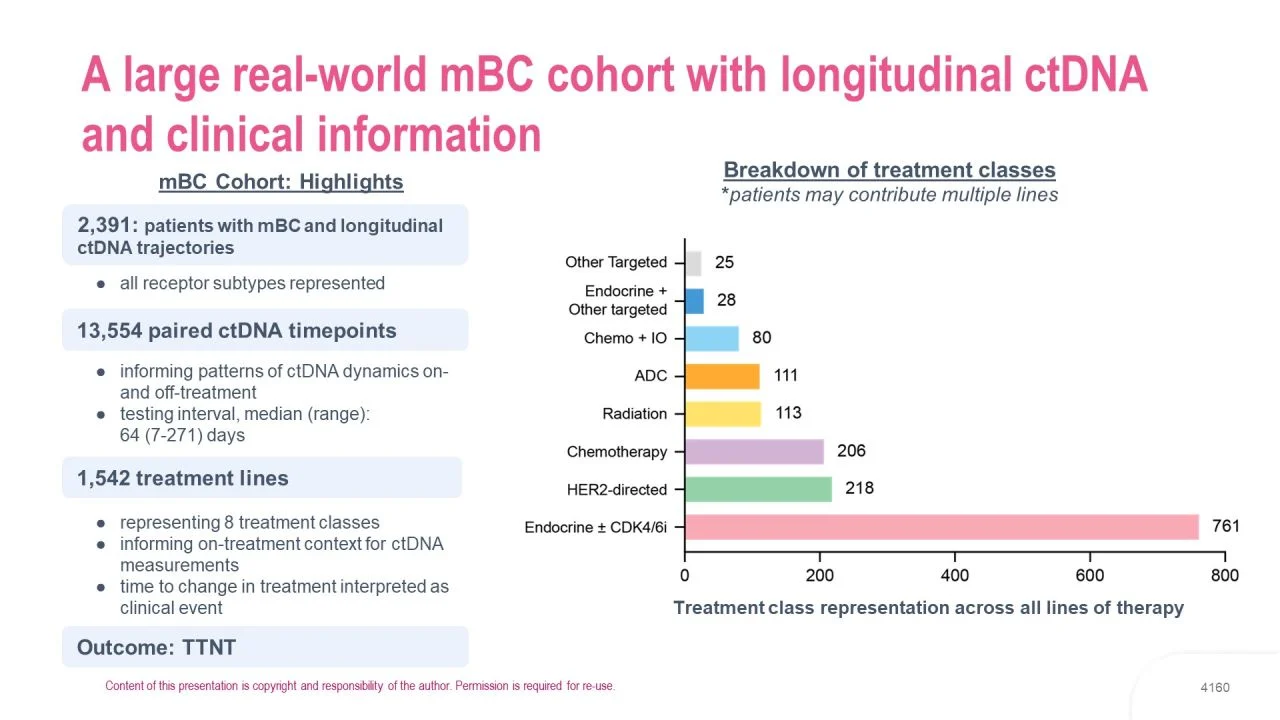
- ctDNA is making its way to clinical practice… and this is unstoppable: this large dataset comes from US patients whose disease is already monitored by ctDNA. Note the test used here monitors tumor fraction in blood, so this is a much broader approach than tracking ESR1m under AI-based therapy.
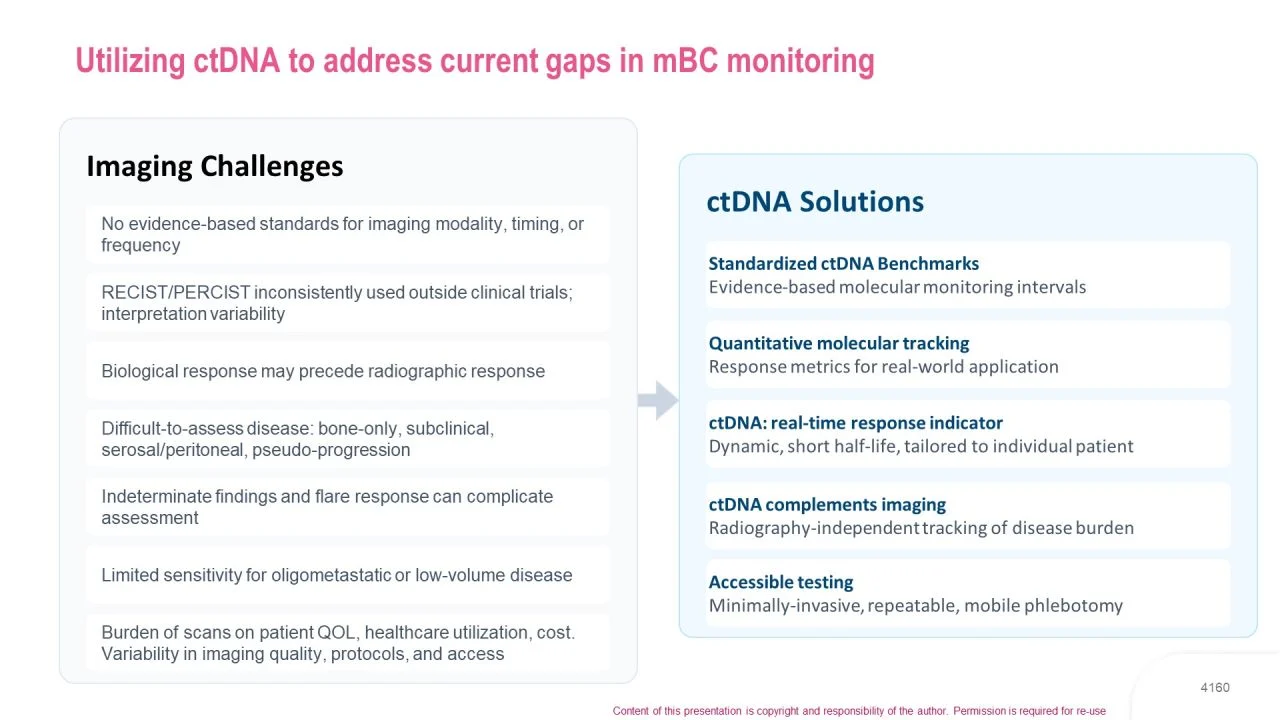
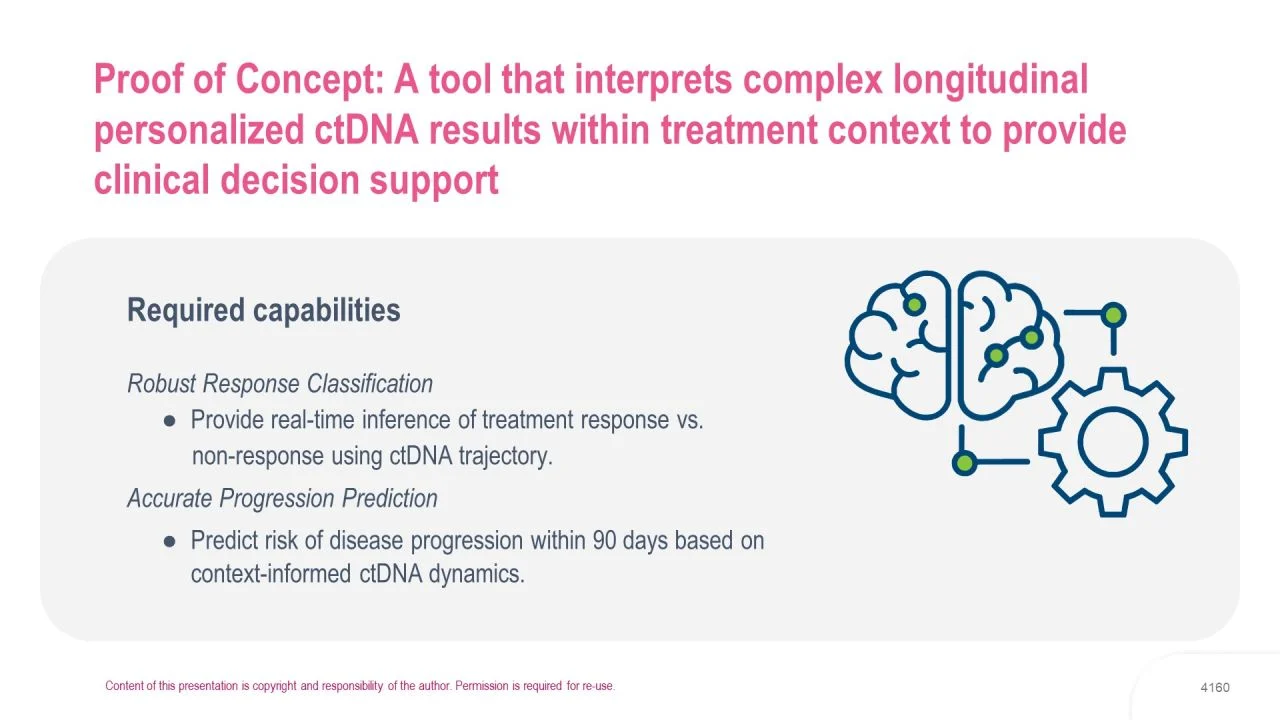
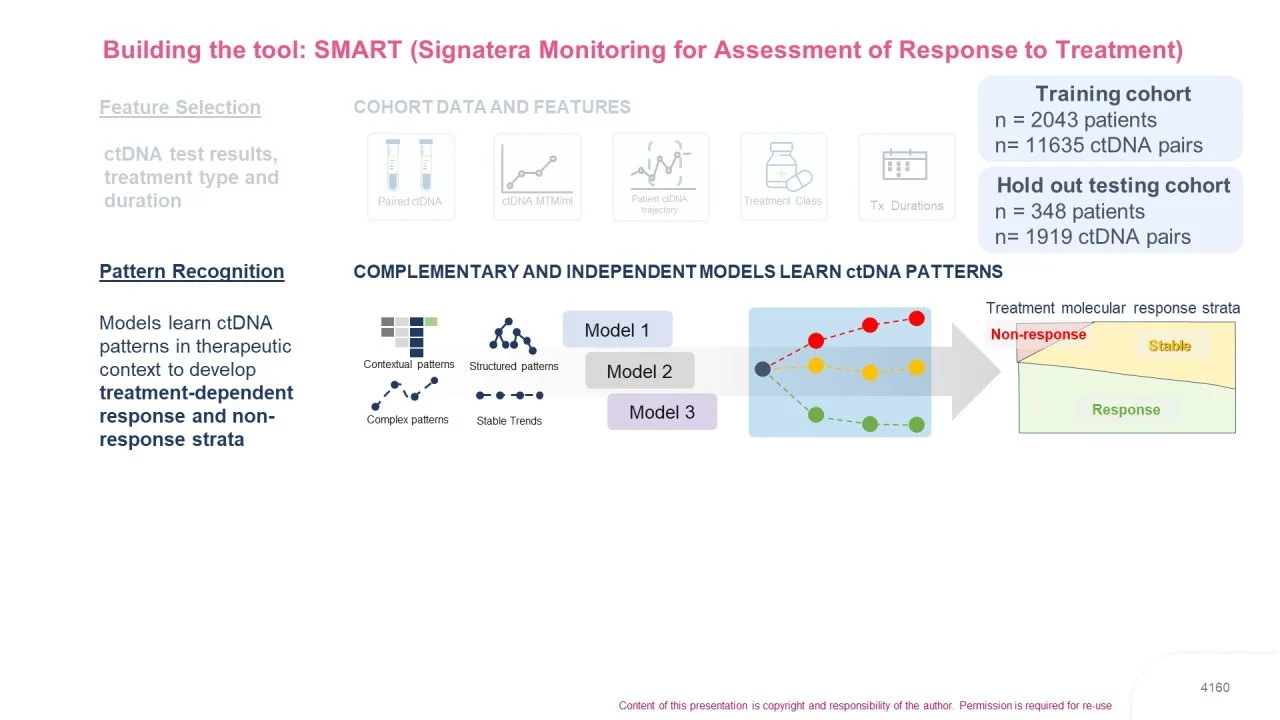
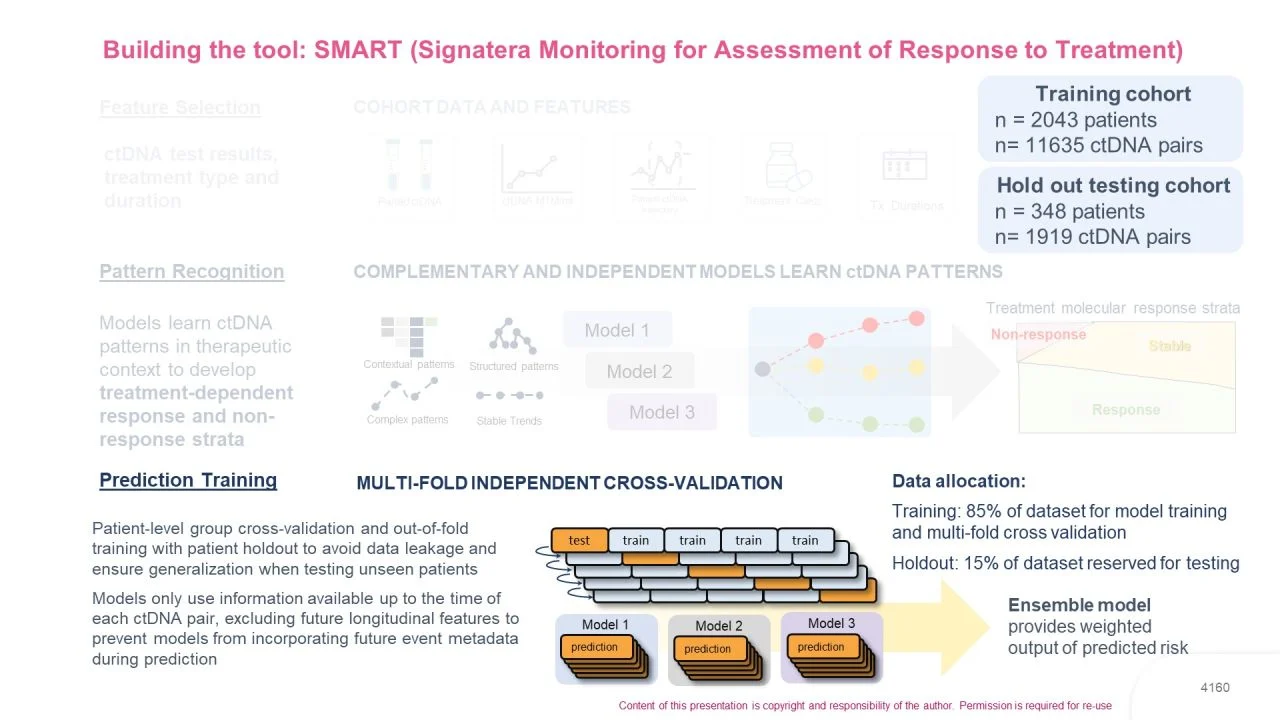
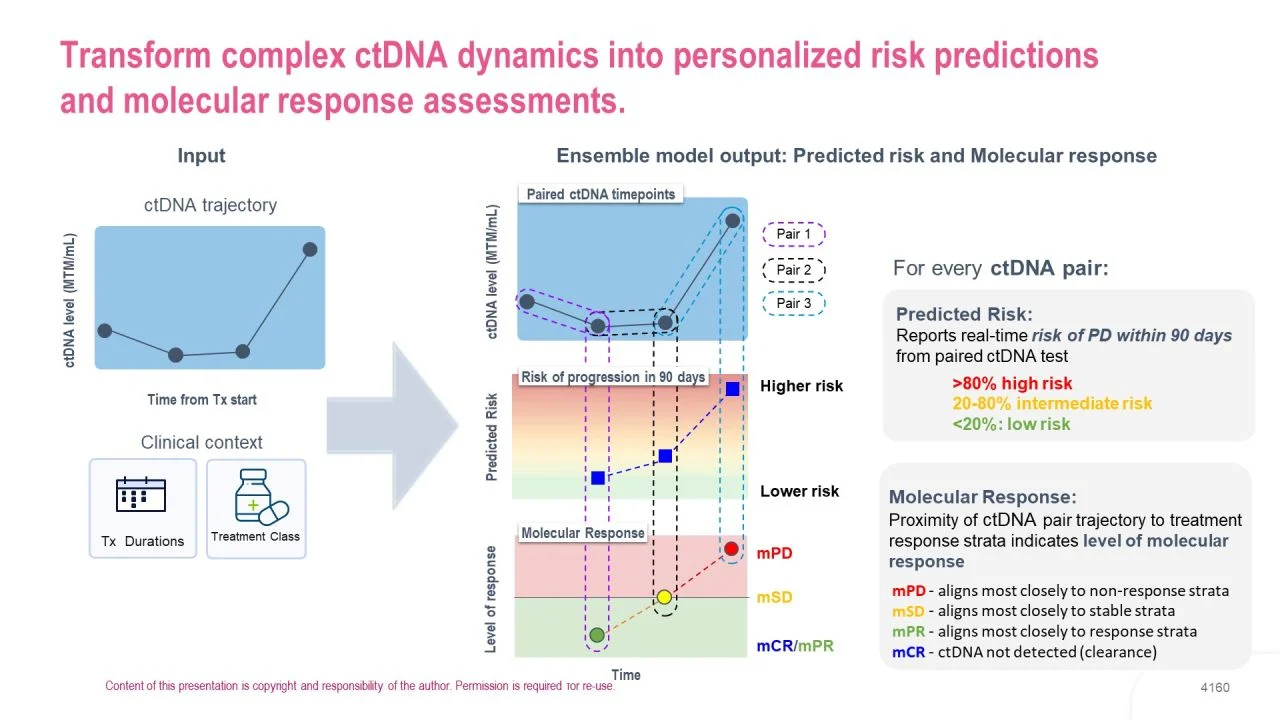
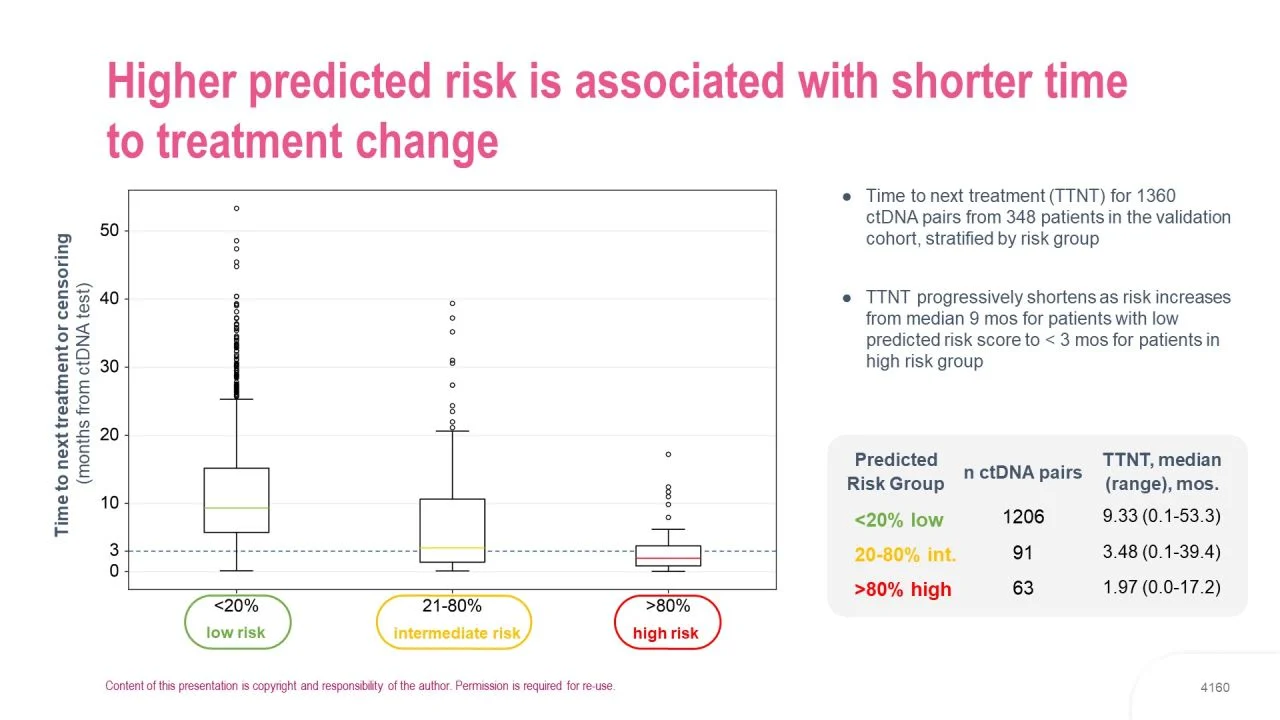
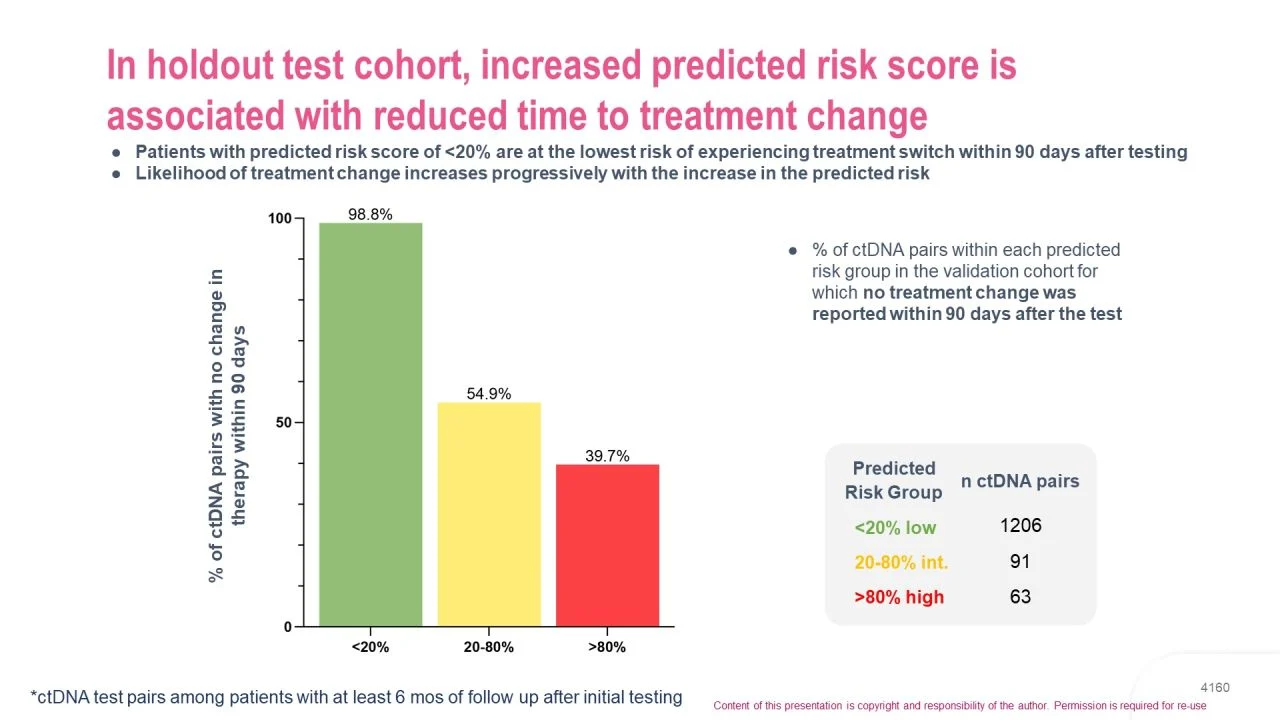
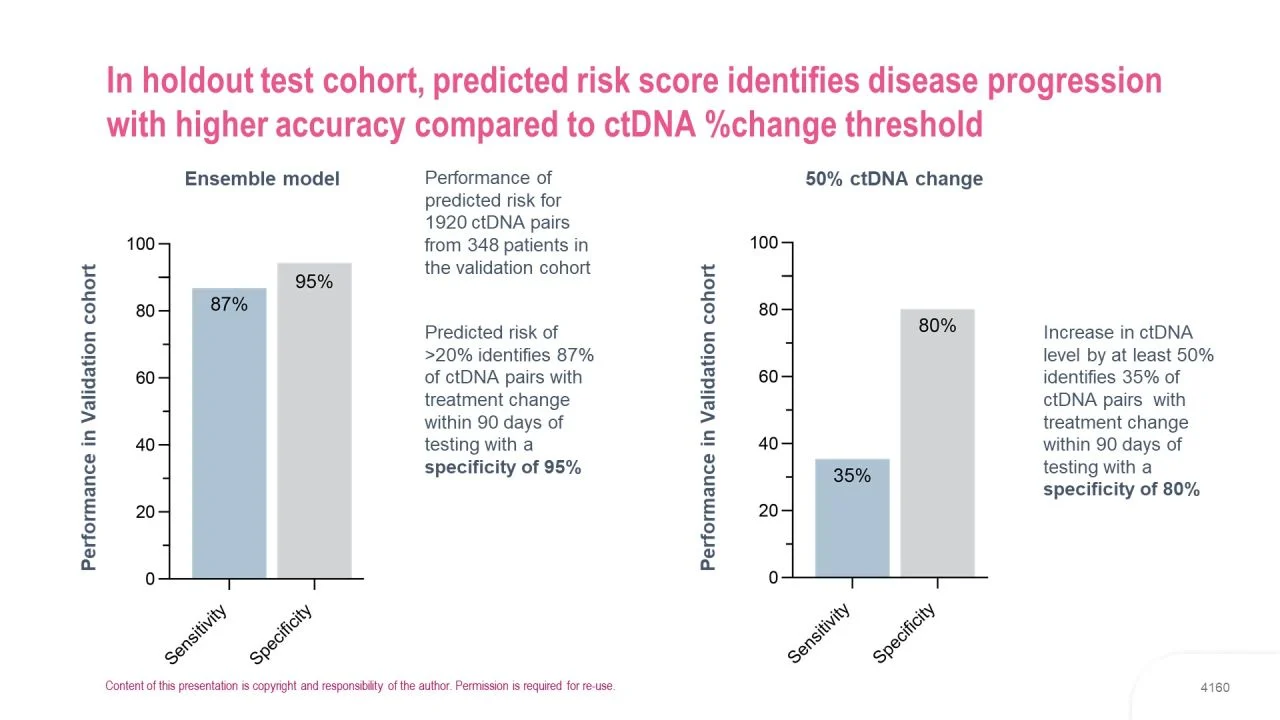
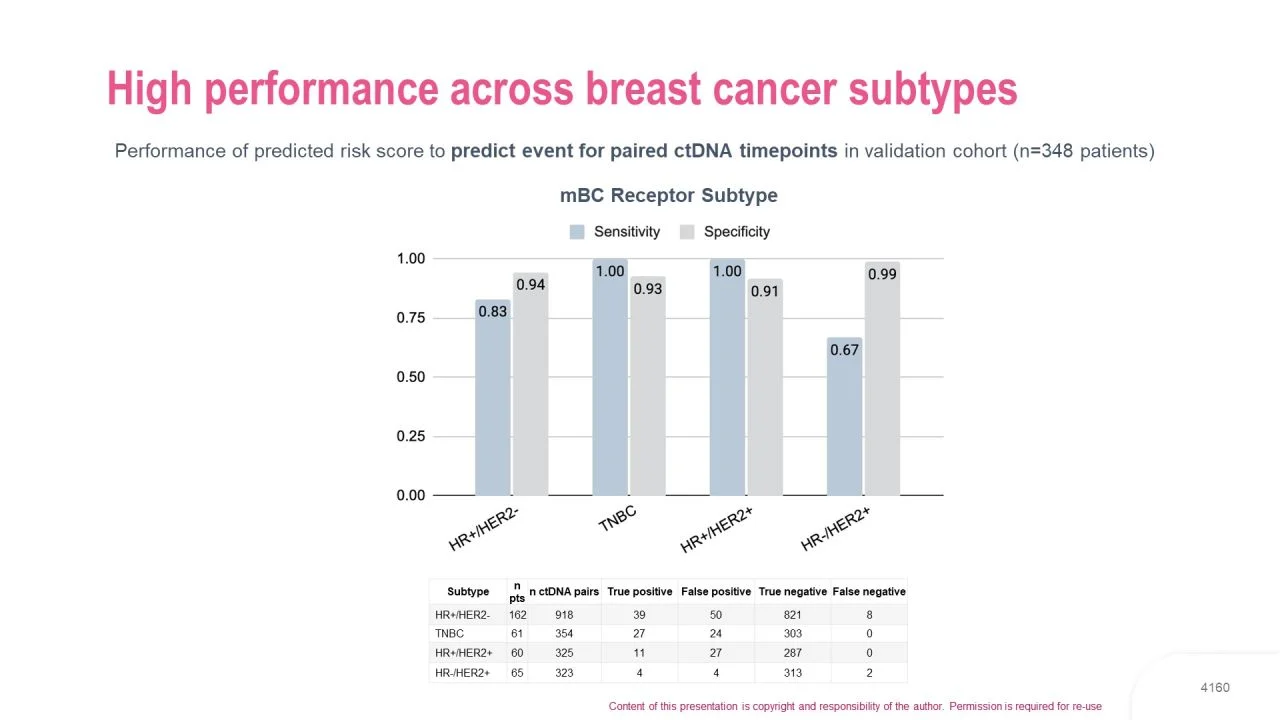
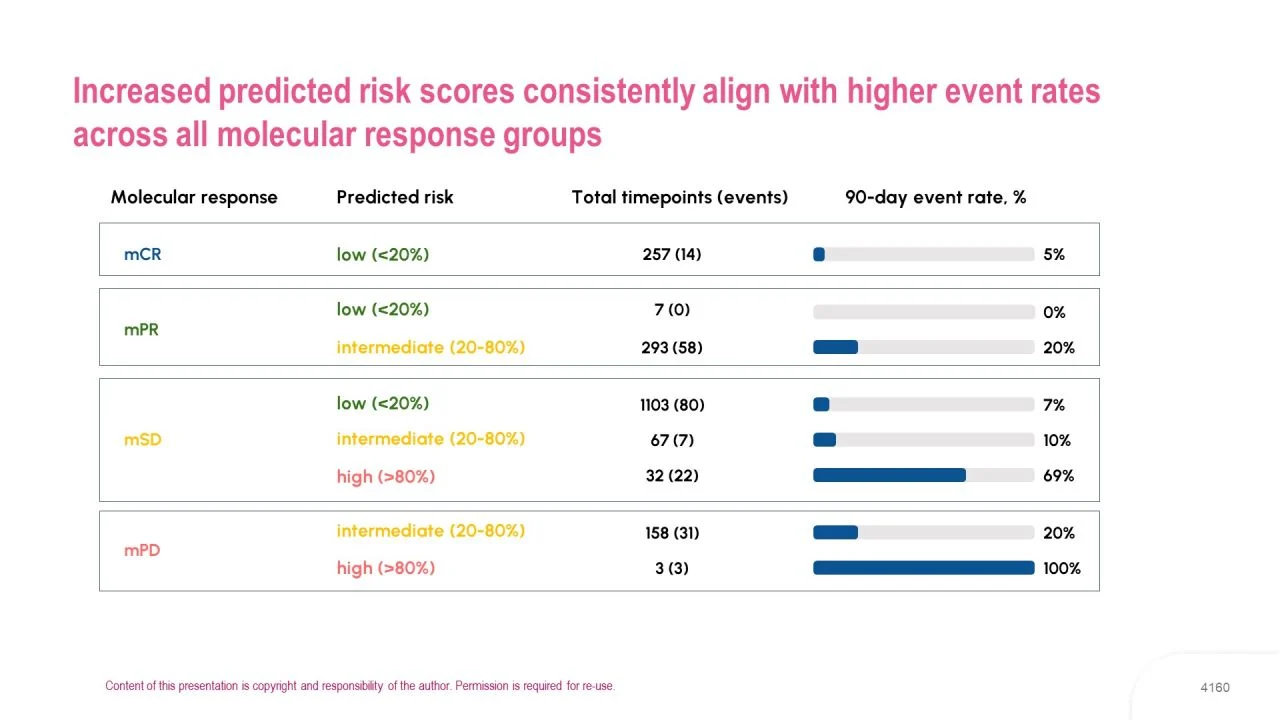
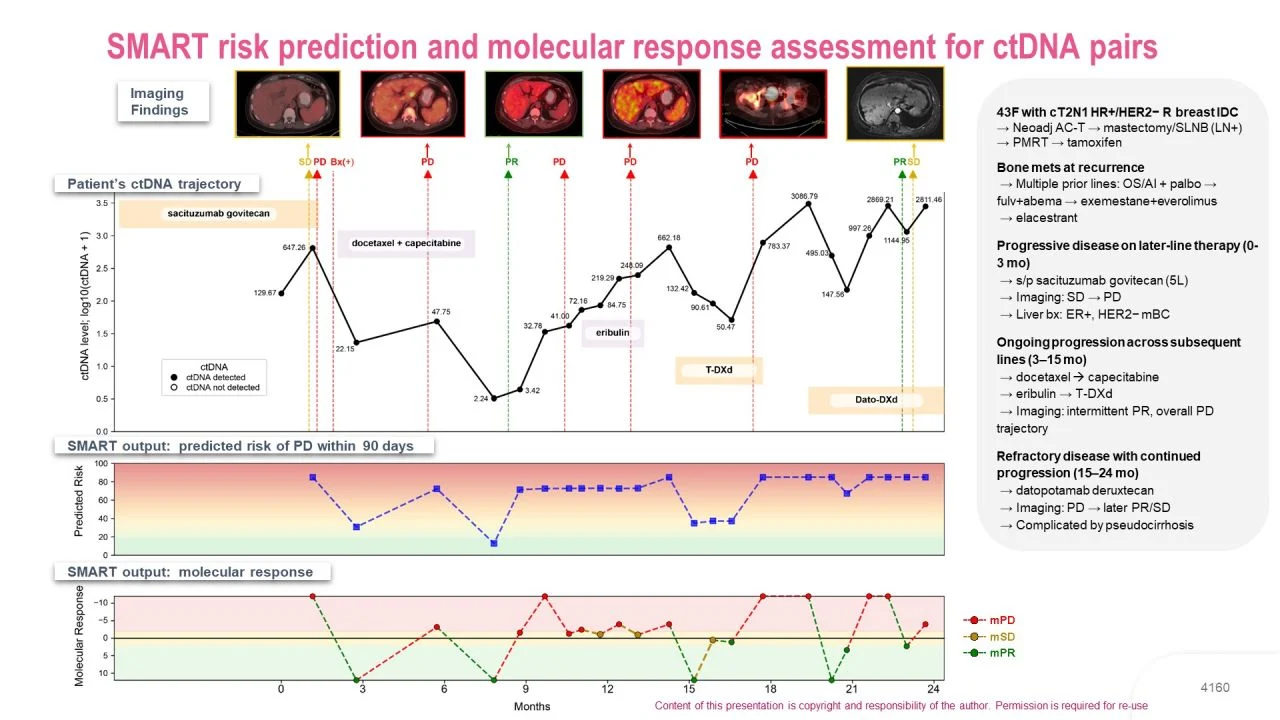
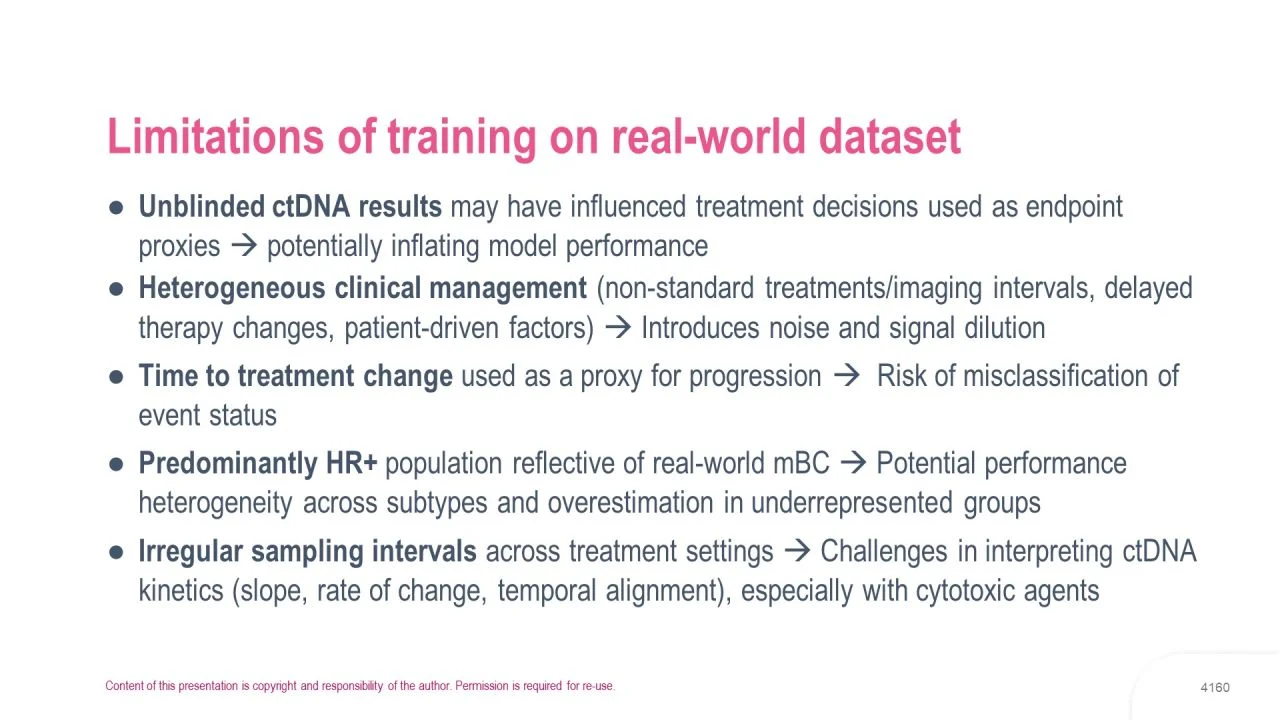
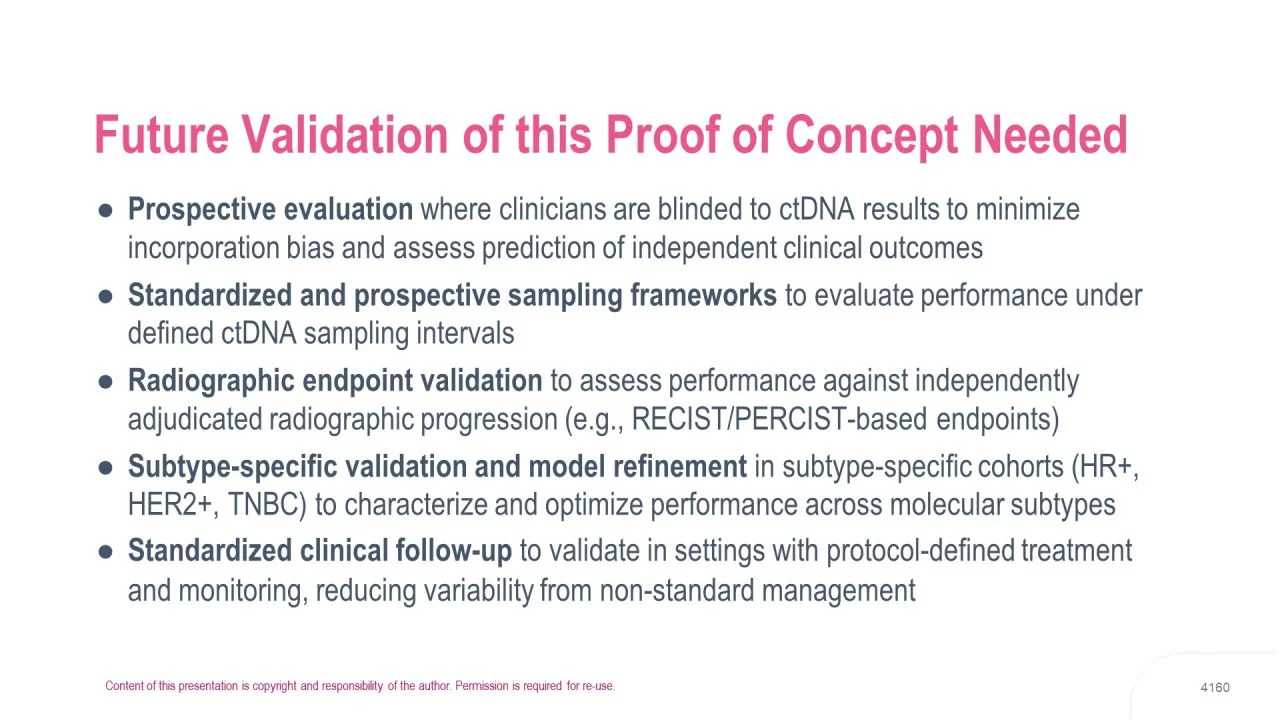
- The multiparametric model based on serial ctDNA monitoring during therapy predicts disease progression very accurately. Further validation is still needed but this approach brings us back to the clinical utility demonstrated in S6: why should we wait for patients to *feel* clinical progression now that we have tools that can detect molecular progression (mPD) ? As highlighted in the introduction slides, imaging based monitoring also has many limitations – our current standard is not so golden.
General concept:
As physicians, we have been trained to wait for symptoms to appear in patients with mBC and only then to catch up. We have learned how to manage/minimize various pains, epiduritis, bowel obstruction, dyspnea, lymphangitis, visceral crisis, symptomatic brain mets, bone marrow involvement, hypercalcemia… and many other complications that may occur at tumor progression.
But what if careful ctDNA monitoring could help us change therapy ‘just before‘ these events occur? That would be a remarkable change in our everyday practice…
(I removed a few slides, not about results, to keep the presentation as short as possible.)”
See the Slides Below in Gallery

Other articles featuring François-Clément Bidard on OncoDaily.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}