


David Sher, Vice Chair of Clinical Operations and Quality, Medical Director of Radiation Oncology, Chief of Head and Neck Radiation Oncology Service at UTSW Medical Center, shared a post on X:
“Come for the critically important data on protons for oropharyngeal cancer, stay for the beautifully written paper.
TORPEdO is out, and it is fascinating and instructive.
I will warn you upfront that this is a long thread, but there is a lot here to discuss!
The study was a phase III RCT comparing IMPT with IMRT (weighted 2:1) for patients with oropharyngeal cancer requiring chemoradiotherapy, with two co-primary endpoints at 12 months following treatment: UW-QOL Composite Score (patient-reported) and either g-tube use or grade 3 weight loss (> 20% baseline) (physician-reported).
Given the challenges in mandating g-tube placement, I think both a one-year endpoint and including the weight loss result are quite reasonable and practical. Each split the alpha, so p=0.025 was considered significant.
The study had 86% power to show an 8 point superiority in the UW-QOL score (considered clinically significant) and a tube dependence/weight loss difference of 25% IMRT versus 7% IMPT. This latter difference seems quite ambitious, even if IMPT is better, but total patient numbers were limited.
The study was stratified by several criteria, including site, T stage, bilateral neck nodes, p16 status, and smoking status. I understand how each are relevant for the endpoint, but that’s 2^5 = 32 boxes for only 200 patients…!
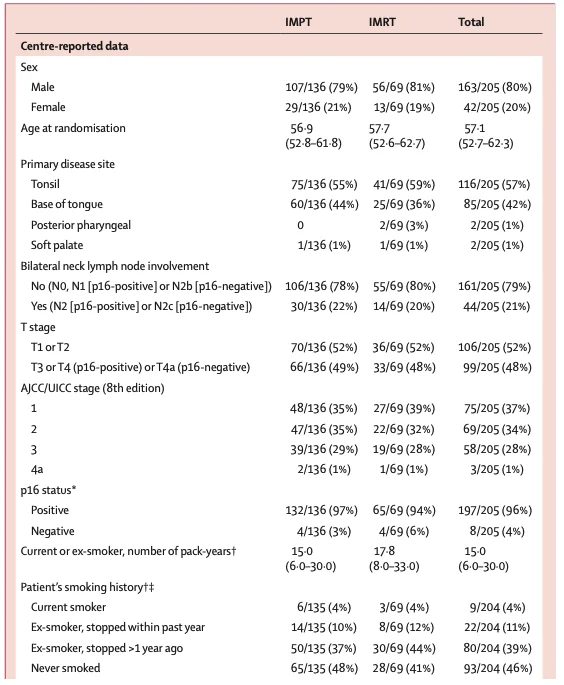
Ultimately, 205 patients were randomized, 136 to IMPT and 69 to IMRT. Key patient characteristics are below.
The treatment approach was protocolized without variation across centers. There were two dose levels (70 and 56 Gy) in 33 fractions (technically 69.96 and 56.1), so that is 5% hotter per fraction than a 35 fraction scheme.
The volumes getting 70 Gy were standardized and would be considered pretty standard, but I still think they were too large. The primary was expanded by 5 mm and the nodes by 10 mm (!), plus 3-5 mm for PTV70. That’s a very large expansion for nodal disease and means the volume getting 70 Gy in the neck was huge. The elective primary volume and neck received 56 Gy.
Importantly, IMPT patients were treated at either the Christie or UCL, whereas the IMRT patients were treated at the local referring center. Despite this distinct difference in treating physician and center, it is important to emphasize the robust QA components that went into ensuring homogeneity between the arms.
In addition to pre-trial credentialing, all contours were reviewed prospectively, and the first plans (IMPT and IMRT) were reviewed for each center. The amount of work there is mindboggling, but also very important for quality control.
In addition, all patients underwent CT resimulation at week 3, with protocol-mandating replanning if the target coverage was inadequate, or if the cumulative dose to a critical organ was more than 2% over tolerance, or the parotid and SMG doses were increased by 3 Gy.
Of note, 61% of all IMPT plans required replanning, versus only 30% in IMRT. That speaks to the work needed to preserve IMPT plan quality over time. I am a huge proponent of adaptive radiotherapy, and even a 30% IMRT replan probability speaks to how frequently plan quality degrades. Can’t wait to see secondary analyses of these interim scans.
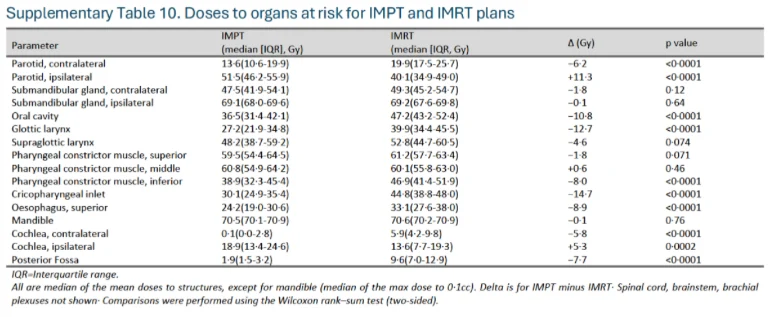
To be totally honest, I was disappointed in the dosimetry of both plans.
Yes, the IMPT plans were better, but there was no sparing of the contralateral SMG, and a glottic larynx mean dose of 40 Gy is very high.
There was no sparing of the ipsilateral parotid, which is ok, but actually the dose was higher in the IMPT patients.
The CPI doses were very high in both arms (44.8 vs. 30.1), as were the esophagus doses (33.1 vs. 24.2).
So personally I think these are suboptimal plans, perhaps due to the large 70 Gy volume in the neck.
I do not think they are representative of modern oropharyngeal IMRT planning (and possibly IMPT planning), even with standard ENI doses.
The results are nicely described in the paper, and in brief, the study was negative for the primary endpoints. The 1-year UWQOL scores are essentially identical, even in the patients with a predicted higher benefit based on NTCP calculations. The feeding tube rate at one year was very, very low in both arms (2%), but there was significantly more significant weight loss in the IMPT patients (18% vs 6%, p for the combined endpoint was 0.079).
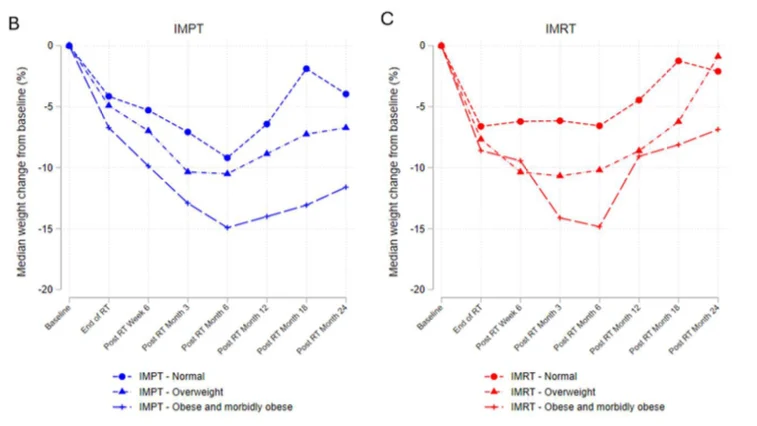
The weight loss curves are quite interesting and show that the most significant weight loss was in heavier patients.
Every pre-treatment BMI cohort preserved more weight over time, though it’s hard to interpret the clinical impact. There were fewer stomach tubes in the IMPT patients, so perhaps that explains the result, and maybe there are some long-term benefits in sustaining the weight loss in overweight/obese patients: hard to know. The results are what they are but do highlight the weight preservation with IMRT.
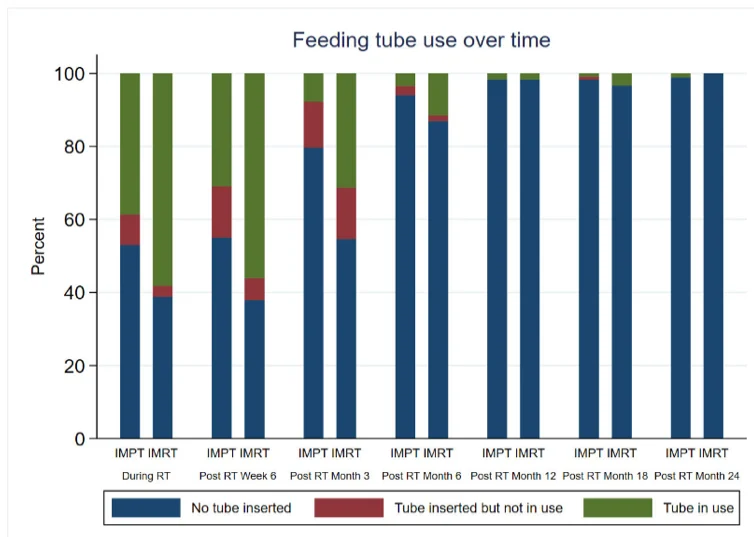
The investigators intentionally chose a one-year endpoint to avoid the messiness of why a given patient is given a g-tube. In absolute terms, more IMRT patients had tubes (58%, 40/59 vs. 45%, 61/135), but there were clearly more prophylactic stomach tubes in the IMRT patients, which highlights some arbitrariness with the decision-making.
In terms of reactive tubes, the numbers were 14/69 (20%) IMRT patients and 26/135 (19%), so all of a sudden it becomes difficult to interpret feeding tube use!
Of course, we don’t know how many patients with a prophylactically-placed tube would have needed a reactive tube, but this highlights how stomach-tube decision-making (as a function of arm) is really hard to resolve.
In fact, the grade 3 weight loss difference was already seen by 6 months, which tells me that IMPT patients who didn’t receive a tube could have benefitted from one (at least with respect to weight preservation).
This issue becomes particularly relevant in interpreting some of the acute grade 3 toxicity results, which clearly favored IMPT (grade 3+ 50% vs 72%), with the bulk of that difference being mucositis (37% vs. 54%).
Oral mucositis was assessed via CTCAE 5.0, which defines grade 3 mucositis as severe pain and unable to aliment or hydrate orally. Oral mucositis can be very difficult to measure, and there are a variety of scoring systems dedicated to it (such as the WHO scoring system), but it is possible that some of this mucositis difference is just because of the differential use of prophylactic feeding tubes (since once you have a tube, usually you use it) rather than directly due to the radiation on oropharyngeal mucosa.
It would be great to see differences in pain medication use, because that would be very telling in terms of what’s happening in the oral cavity. Protons do a significantly better job in the oral cavity, and that should be valuable for mucositis, but hard to know specifically here.
Side note: despite the g-tube use being 58% (IMRT) and 45% (IMPT), grade 3 dysphagia was only 24%/12%. I don’t understand that… while not every inserted tube was used, about 40% of IMPT patients and 60% of IMRT did use them.
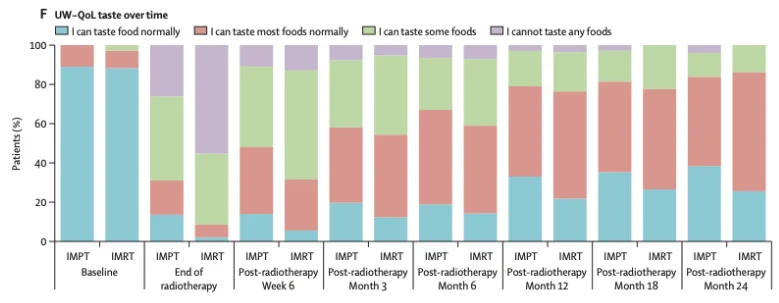
It is important to point out the transient improvement in dysgeusia in the IMPT patients. Both patient-reported (UWQOL taste, see chart) and physician-assessed taste was better in the IMPT patients (42% vs 66% grade 2 dysgeusia acutely, and 16% vs. 26% at 3 months), but there were no differences by 12 months.
However, I think taste preservation is very important, and there may be a subtle signal here.
The PRO data are remarkably helpful to understand the patient experience over time. Patients in the IMPT arm seemed to do better by the end of radiotherapy (no p value provided), but by 6 weeks on there were no differences.
I would also highlight the fact that while patients did recover over time, the majority were clearly experiencing significant side effects over time, and we need to continue to improve their long-term outcomes.
It is somewhat incredible that given the clear difference in dosimetry, patient-reported outcomes were no different in the long-run. We saw the same results in our dartboard trial of daily adaptive radiotherapy. We need to invest more work into understanding the dose:patient-reported response relationship to improve the long-term patient experience.
Unfortunately, there were a fair amount of missing data, especially for the PRO results (25% missing IMPT, 18% IMRT), and one cannot dismiss the possibility that these non-compliant patients may have had different outcomes and the equivalent of informative censoring.
There was no difference in any survival endpoint, though there was a small trend towards more LRR in the IMPT patients (7% versus 3%). I doubt that’s real, and there is insufficient follow-up to refute the inexplicable OS improvement after recurrence seen in the US trial.
TORPEdO was an incredible effort by the investigators and patients, and the paper analyzes the results extraordinarily well. Given the normalization of outcomes over a very short period of time following treatment, plus the difference in weight loss without any sacrifice in a very low risk of g-tube dependence over time, I agree with the paper’s conclusion: “In health-care settings where IMPT is not used routinely for oropharyngeal squamous cell carcinoma, IMRT remains the standard-of-care.”
Especially since IMRT in 2026 is markedly better than the delivered treatments in the trial, it is hard to see how IMRT shouldn’t always be the standard-of-care.
The key is not stopping there. It is critical to remember that in both arms, about 50% or more of patients reported altered appearance, taste, swallowing and saliva: we need to do better!
And additional improvement clearly will require something more meaningful than protons or photons.
Total dose, elective dose, and elective volumes all need to be personalized and optimized. Let’s go!”
Title: Proton beam therapy for oropharyngeal cancer (TORPEdO): a phase 3, randomised controlled trial
Authors: David J Thomson, James M Price, Matthew Tyler, Matthew Beasley, Jim Lester, Christopher M Nutting, Nachi Palaniappan, Robin Prestwich, Shanmugasundaram Ramkumar, Anna Thompson, Guy Betts, Helen Bulbeck, Frances Charlwood, Matthew Clarke, Matthew Lowe, Justin Roe, Justine Tyler, Lorna Wilson, Jane L Wolstenholme, Kevin Chiu, Judith Christian, Clare Cruickshank, Deborah Gardiner, Holly Tovey, Catharine M West and Emma Hall

Other articles featuring David Sher on OncoDaily.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}