
Post-transplant maintenance for AML: Review of literature by Talha Badar
Talha Badar shared a post on X:
“Post transplant maintenance for AML.
- How should you define effectiveness?
- Patients that can benefit the most?
- What should be the duration of therapy?
Review of literature, pitfalls.
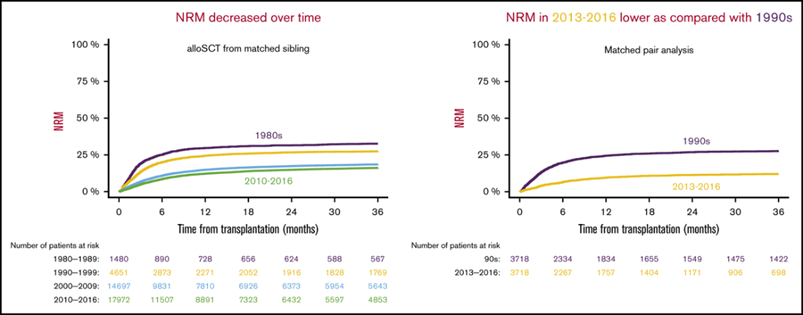
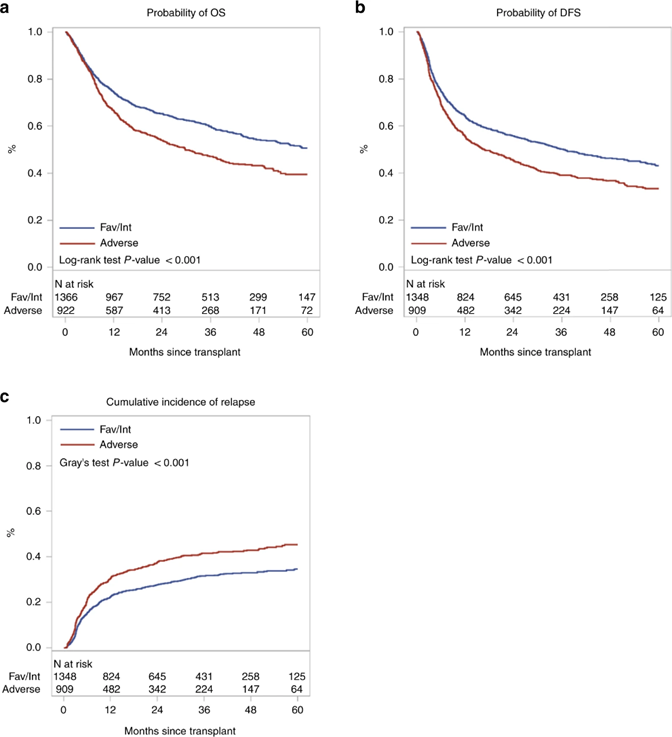
While NRM mortality has decreased significantly over recent decades, disease relapsed remains a major cause of allo-HCT failure in adverse risk AML (e.g TP53m, complex CG, monosomal CG etc)
Ref: An adapted European LeukemiaNet genetic risk stratification for acute myeloid leukemia patients undergoing allogeneic hematopoietic cell transplant. A CIBMTR analysis | Bone Marrow Transplantation.
Authors: Olaf Penack et al.

Current practices regarding maintenance therapy in AML post-allo-HCT
- FLT3m AML –> FLT3 inhibitors
- IDH1/2 –> Clinical trial,? IDH inhibitor
- High risk CG/TP53m –> Clinical trial,? HMA,? HMA +venetoclax
- Absence of molecular target, HR- AML –> Clinical trial,? HMA
Key points that influence decision on maintenance therapy post-allo-HCT
- High risk disease at time of allo-HCT
- Sub-optimal response prior to allo-HCT
- Highly active targeted therapy (FLT3i, IDHi, most recent menin inhibitor)
- Intensity of conditioning regimen, higher consideration with RIC
Post AlloHCT maintenance therapy for FLT3m AML
First one tested sorafenib; P1 study on 22 pts, 1 yr PFS 85% and OS 95%. (Chen et al BBMT 2014)
SORMAIN trial, PIII study, placebo controlled from China, 24 mo RFS 85% vs 53%, p= 0.002, OS 83% vs 58%, p= 0.019
RATIFY trial showed benefit of Midostaurin upfront, post AlloHCT maintenance was safe, not powered to show benefit in relapse maintenance.
Quizartinib: P1 study conducted showed acceptable tolerance and reduce risk of relapse. (link)
Crenolanib is also being tested as maintenance therapy, accrual completed, result awaited (NCT02400255)
BMTCTN conducted PIII placebo-controlled trial Gilteritinib as Post-Transplant Maintenance for AML With Internal Tandem Duplication Mutation of FLT3 | Journal of Clinical Oncology (link)
PE: RFS and SE: OS
RFS was not statistically significant in the Gilt arm, however, patients with detectable MRD had a higher RFS.
IDH inhibitors as maintenance therapy post-AlloHCT.
Multiple ongoing phase 1 and 2 trials are investigating the use of ivosedinib (NCT03564821 and NCT03839771).
and Enasidenib (NCT03515512, NCT03728335, NCT04522895, and NCT03839771) as maintenance therapies after allo-HCT.
P1 study of Enasidenib post-allo-HCT showed acceptable toxicity, relapse rate were lower at 13% at a median fu of 11.7 months (Fathi et al, ASH abstract 2020).
HMA based maintenance post-allo-HCT.
So far the data on effectiveness of HMA is conflicting!
Initial studies (P1/P2) showed encouraging results.
Oral AZA maintenance showed lower relapse rate and GVHD.
Authors: Marcos de Lima et al.

P3 study did not show benefit in improving RFS.
Authors: Betül Oran et al.

Should we continue to use HMA post-AlloHCT in HR AML, esp TP53m? or should we combine with venetoclax. Open label PIII study is ongoing (VIALE-T 10.1097/01.HS9.0000845132.53694.7f)
Conclusion
Post-transplant maintenance for AML.
While we as a clinician are always enthusiastic to use maintenance therapy post-AlloHCT in HR AML or those with strong therapeutic target, data is not convincing in majority of situations, except for FLT3.
Biggest obstacles are cytopenia and immunosuppression from non-targeted agents.
Better MRD assessment may help in preemptively using maintenance therapy effectively.”
Source: Talha Badar/X
More posts by Talha Badar in OncoDaily.
Dr. Talha Badar, MD, is a specialist in Hematology Oncology based in Mayo Clinic, Jacksonville, Florida. His primary areas of expertise include Leukemia, particularly Acute Myeloid Leukemia (AML), Myelodysplastic Syndrome (MDS), Acute Lymphoblastic Leukemia (ALL), and Bone Marrow Transplantation. Over his career, he has actively contributed to clinical research and clinical trials.
{kind=link}
{kind=link}
-
Challenging the Status Quo in Colorectal Cancer 2024
December 6-8, 2024
-
ESMO 2024 Congress
September 13-17, 2024
-
ASCO Annual Meeting
May 30 - June 4, 2024
-
Yvonne Award 2024
May 31, 2024
-
OncoThon 2024, Online
Feb. 15, 2024
-
Global Summit on War & Cancer 2023, Online
Dec. 14-16, 2023