


François-Clément Bidard, Head of Center for Clinical Investigation CIC-2501 at Inserm, shared a post on LinkedIn:
“Enclosed are the new results from SERENA-6 that I presented at ESMO Breast related to the screening step (‘before‘ randomization, detection of ESR1mut in patients treated with AI and CDK4/6i).
Important reminders:
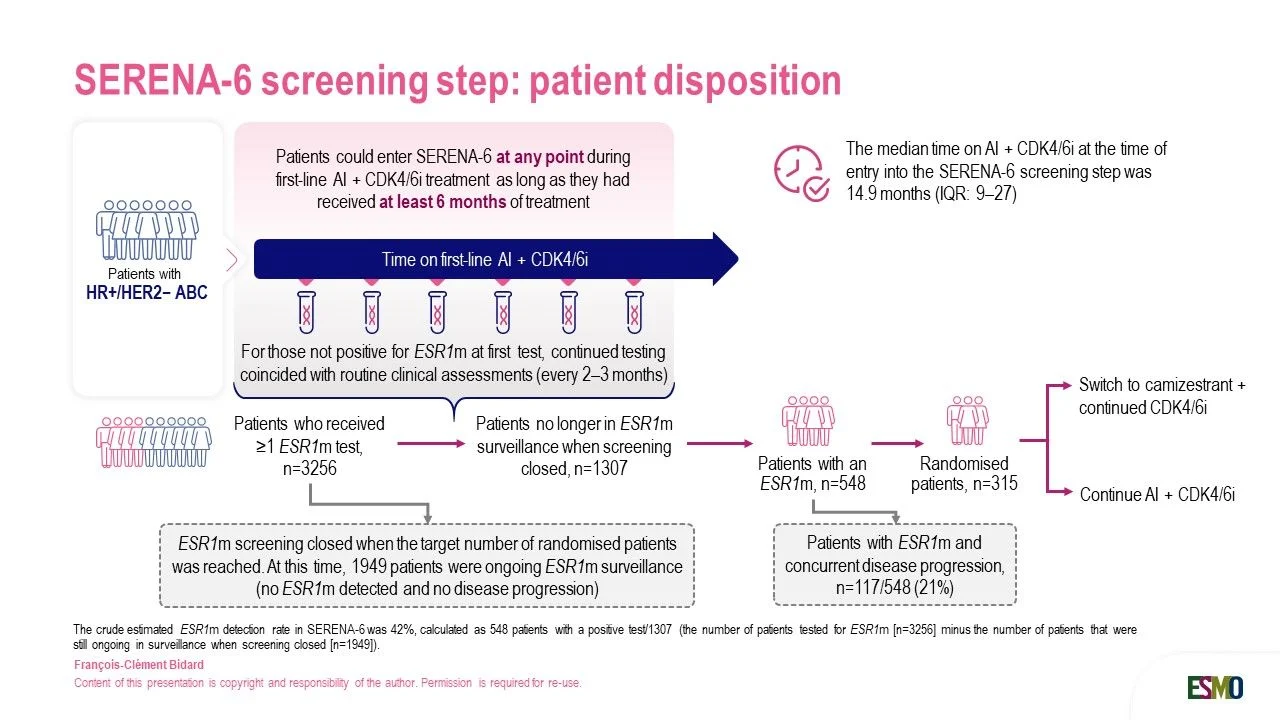
- In contrast to PADA-1 (inclusion occured before the start of AI+PAL), patients could enter SERENA-6 at any time while they were already on AI+any CDK4/6i (for at least 6 months). The median time already spent on AI+CDK4/6i at entry in the screening step was ~14 months.
- Screening was discontinued when the target number of patients was randomized, leaving ~2,000 pts still in screening and without ESR1m detected yet (they could have developped ESR1m later)
Key facts and interpretation:
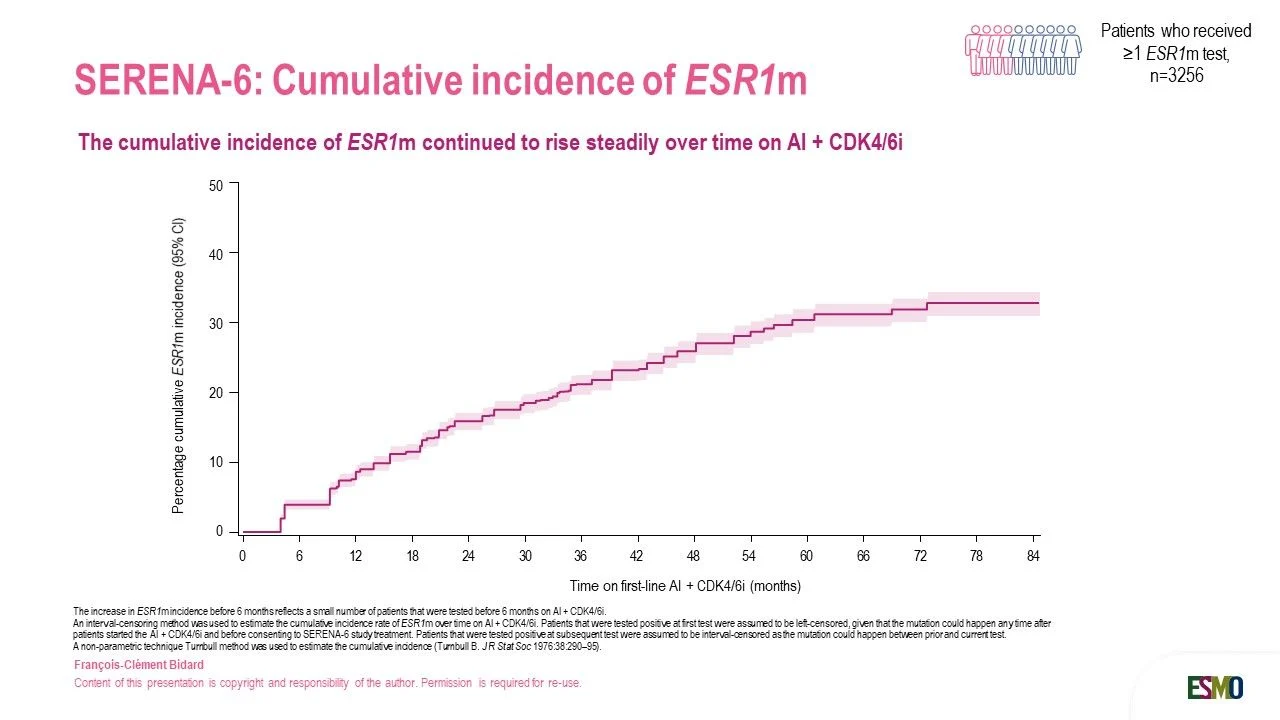
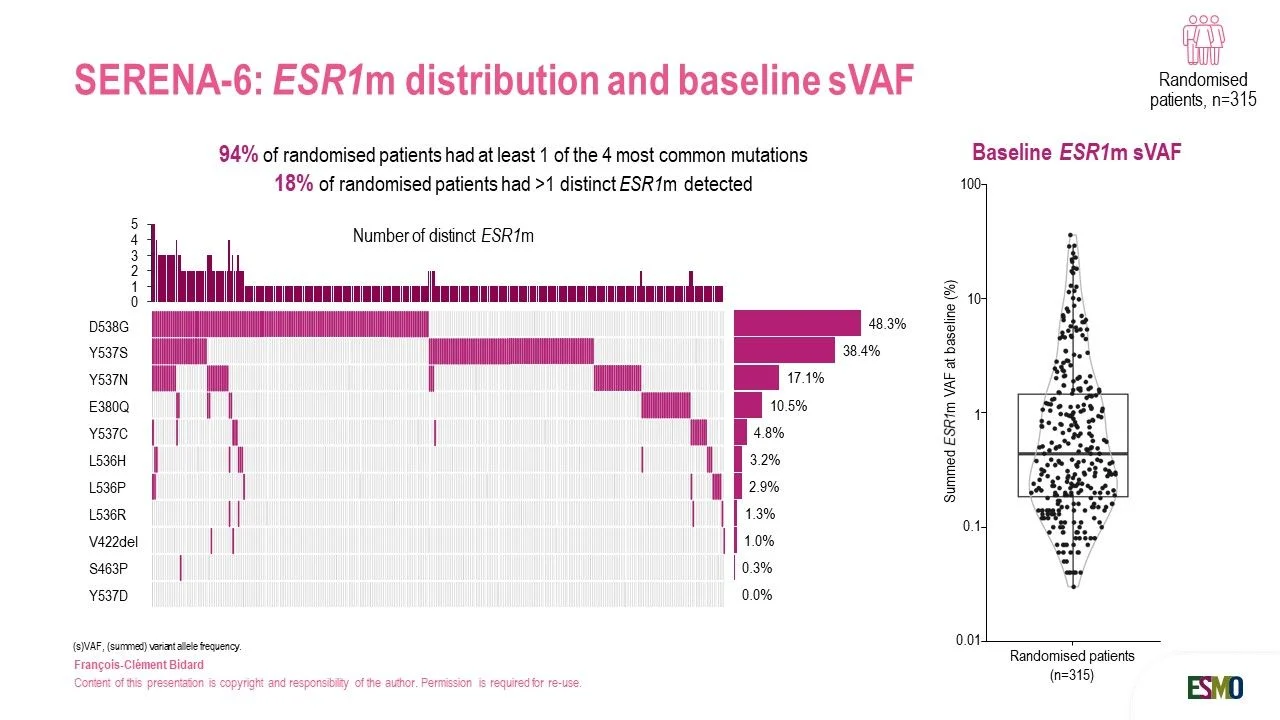
- The crude rate of ESR1m detection was ~40% in the informative population (i.e. patients who were not anymore in screening when it was discontinued). The cumulative incidence of ESR1m increases steadily over time. [findings very aligned with PADA-1]
- ~20% of pts positive for ESR1m displayed synchronous disease progression. In other words, ESR1m were detected too late in these patients could not be randomized. [Disease progression actually follows closely after ESR1m detection. This finding, already observed in PADA-1, argues against the idea that ESR1m interception is ‘too early’.]
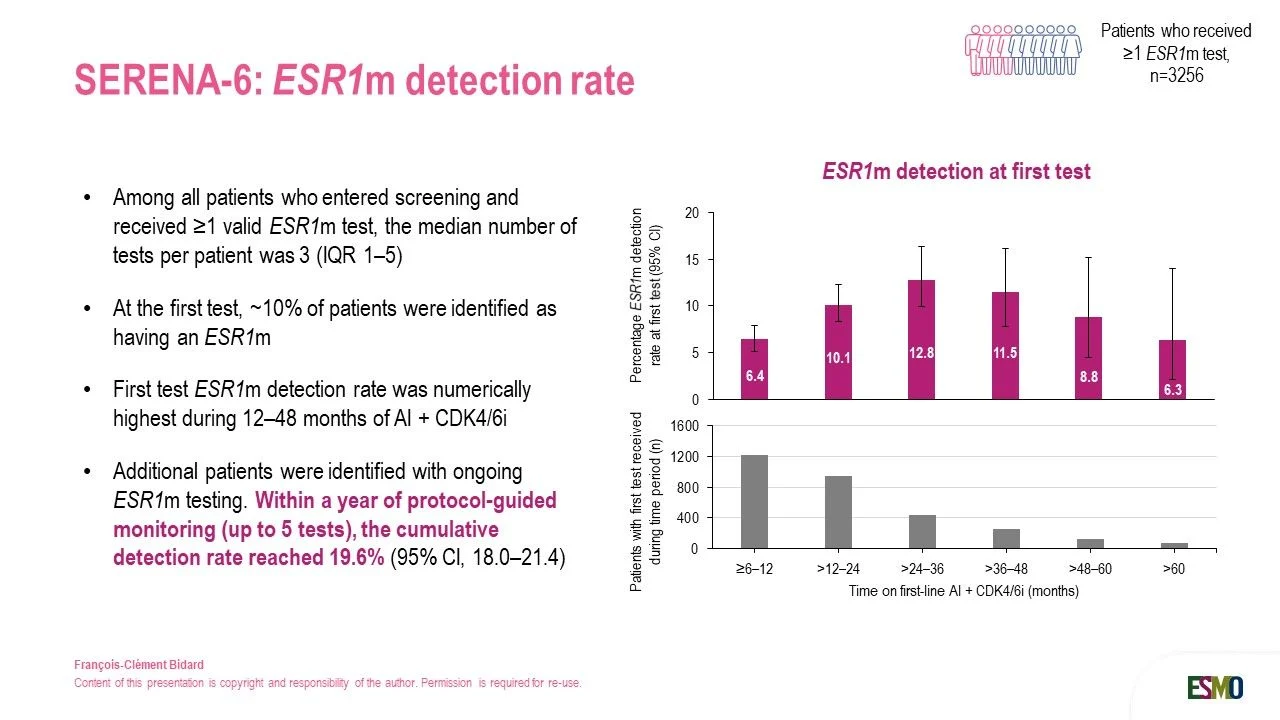
- ~10% of pts were ESR1m+ at the first test, and a total of ~20% of pts became ESR1m+ when screened over 12 months during routine hospital visits. [no need to screen for ages to find a significant % of patients being positive]
- The incidence of ESR1m was maximal between 1 and 4 years. [We confirm the bell-shaped curve observed in PADA-1, Luc Cabel et al, Ann Oncol 2026, while extending the duration of the ‘high risk’ zone.]
- Patients were almost exclusively randomized based on ESR1m in two hotspot regions (codon 380 in exon 5, codons 536-538 in exon 8). [Detecting SNVs at two hotspots is a walk in the park for molecular biologists and could be achieved with many assays, including cheap ones (e.g. ddPCR such as in PADA-1)]”

Other articles featuring François-Clément Bidard on OncoDaily.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}