


A new systematic review and meta-analysis published in JAMA Oncology suggests that local investigator-assessed progression-free survival and blinded independent central review-assessed progression-free survival produce broadly comparable estimates in randomized trials of hormone receptor-positive, HER2-negative metastatic breast cancer.
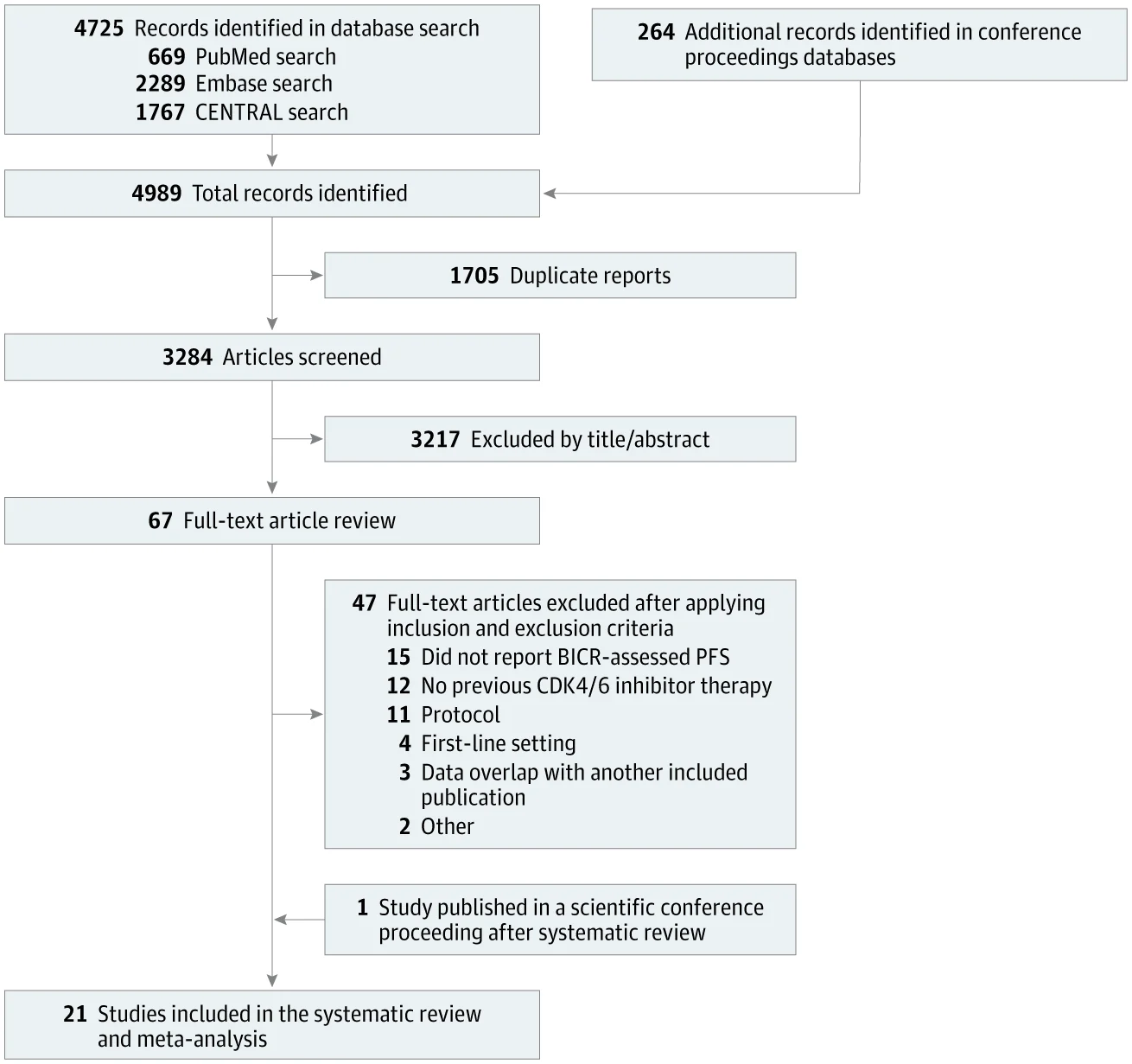
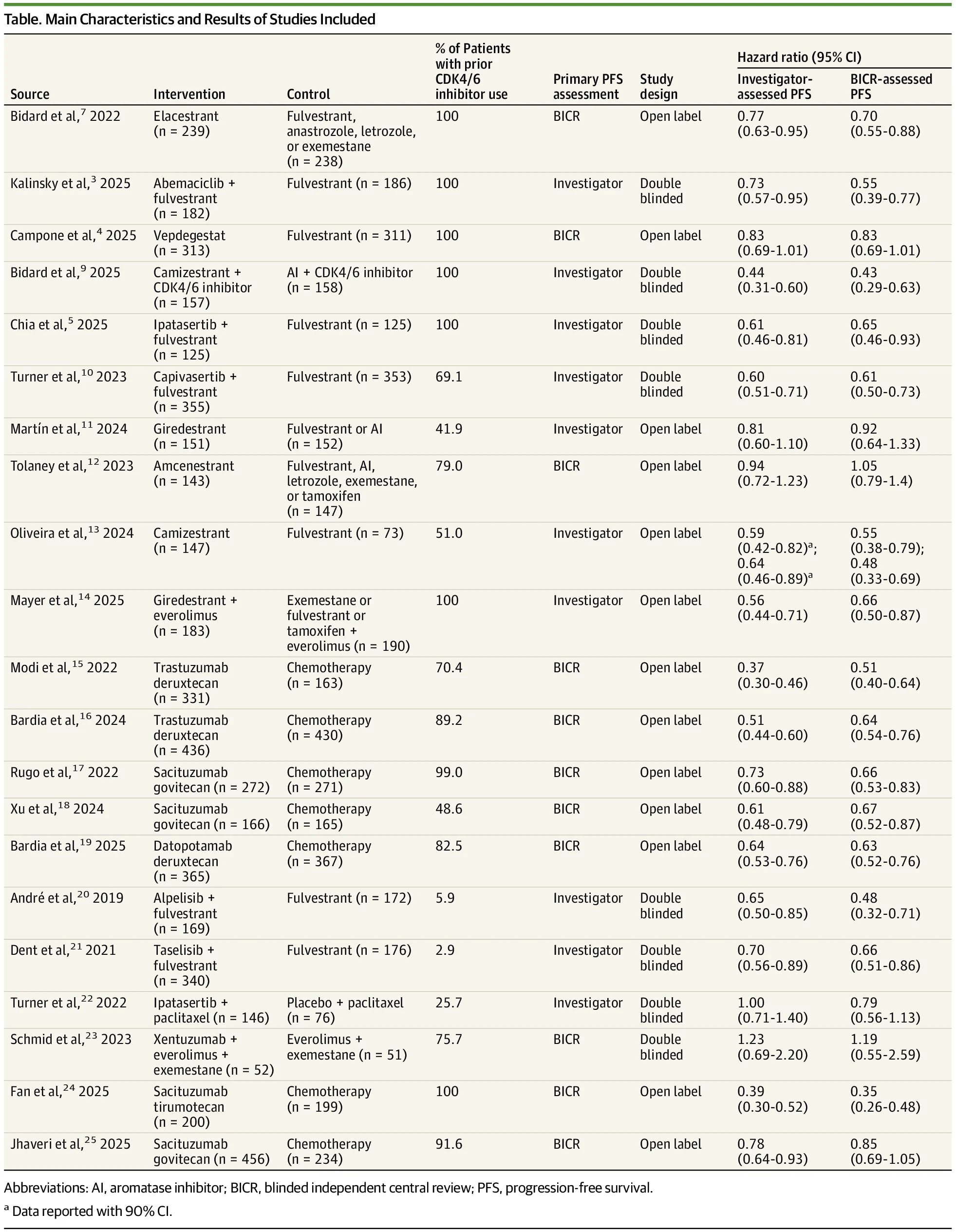
The analysis included 21 randomized clinical trials and 9,165 patients with HR-positive/HER2-negative metastatic breast cancer, focusing on studies that reported PFS by both local investigators and blinded independent central review, or BICR.
The findings are clinically relevant because PFS is one of the most commonly used endpoints in metastatic breast cancer trials. However, how PFS is measured can influence interpretation, regulatory discussions, trial cost, and cross-trial comparisons.
Why PFS Assessment Matters
Progression-free survival is widely used as a primary endpoint in metastatic breast cancer trials because it can capture whether a treatment delays tumor growth or disease worsening before overall survival data mature.
But PFS is also vulnerable to measurement variability. Local investigators assess progression in the context of real-time clinical care, including imaging, physical examination, symptoms, laboratory findings, and patient status. BICR, by contrast, uses blinded external reviewers who evaluate imaging according to protocol-defined criteria.
BICR is often used to reduce bias, especially in open-label trials where investigators know which treatment the patient received. However, it adds cost, logistics, and operational complexity. The key question is whether BICR meaningfully changes the PFS estimate compared with investigator assessment.

What the Meta-Analysis Studied
The authors searched PubMed, Embase, CENTRAL, and major conference proceedings through November 27, 2025.
Eligible studies were phase 2 or phase 3 randomized clinical trials in HR-positive/HER2-negative metastatic breast cancer that allowed or required prior CDK4/6 inhibitor therapy, evaluated second-line or later interventions, and reported PFS by both investigator assessment and BICR.
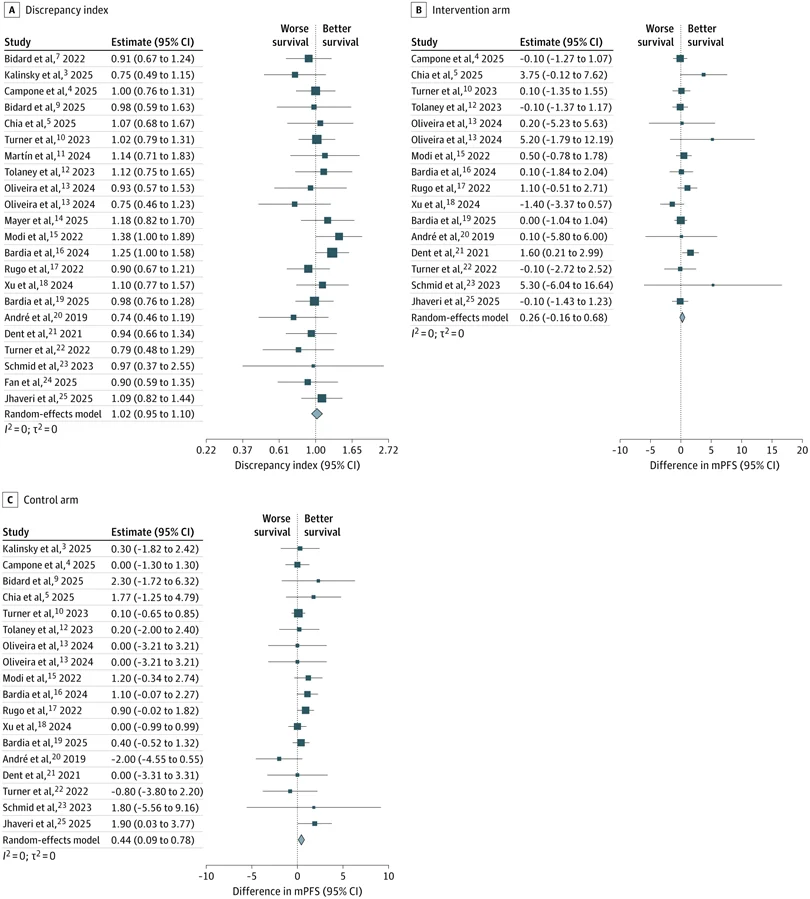
The main outcome was the discrepancy index, defined as the ratio between the BICR-assessed hazard ratio and the investigator-assessed hazard ratio. A discrepancy index close to 1 indicates that the two approaches produced similar treatment-effect estimates.
No Significant Difference Overall
Across the 21 trials, the overall discrepancy index was 1.02, with a 95% confidence interval of 0.95 to 1.10 and a p-value of 0.57.
This means there was no statistically significant difference between BICR-assessed and investigator-assessed PFS overall. The result was consistent across meta-regression analyses.
Subgroup analyses also showed no meaningful differences when the analysis was limited to trials requiring prior CDK4/6 inhibitor exposure, trials using endocrine or targeted therapy as the control arm, and open-label studies.
Median PFS Differences Were Small
The authors also evaluated absolute differences in median PFS between BICR and investigator assessment.
In the interventional arms, the pooled difference was 0.26 months, with a 95% confidence interval from −0.16 to 0.68 months, which was not statistically significant.
In the control arms, BICR-assessed median PFS was slightly longer, with a pooled difference of 0.44 months. This difference was statistically significant, but clinically small.
The authors noted that this small control-arm difference may reflect features of open-label trials, particularly those involving chemotherapy comparisons, where investigator bias may influence the timing or interpretation of progression.

Why This Is Important for Trial Design
The findings challenge the assumption that BICR is always necessary to generate reliable PFS estimates in HR-positive/HER2-negative metastatic breast cancer trials.
In this analysis, investigator-assessed PFS appeared reliable at the trial level, producing estimates similar to BICR. This has practical implications because BICR requires additional imaging workflows, external review infrastructure, data management, and cost.
However, the result does not mean BICR is never useful. Some trial settings may still warrant BICR, especially where the risk of bias is higher, endpoints are more subjective, imaging schedules vary, or regulatory confidence requires independent confirmation.

A Disease Setting With Unique Assessment Challenges
HR-positive/HER2-negative metastatic breast cancer can be difficult to assess radiographically. Progression may involve bone, skin, lymph nodes, pleural effusions, or other sites where RECIST-based measurement may be less straightforward than in trials dominated by measurable visceral disease.
This makes the comparison between investigator assessment and BICR especially important in this subtype. Local investigators may incorporate clinical context that is not available to central reviewers, while BICR may provide standardized imaging interpretation.
The study suggests that despite these differences, the overall PFS treatment-effect estimates were largely concordant.
Important Limitations
The analysis was based on trial-level data, not individual patient data. This limits the ability to evaluate patient-level discordance between investigator and BICR assessments.
The included trials also varied in treatment type, design, control arms, scan frequency, and whether BICR or investigator assessment was the primary analysis method.
The authors also noted that they could not adjust for some relevant operational variables, including timing between local and central assessments, imaging frequency, and how disagreements between assessment methods were handled.
The Bottom Line
This JAMA Oncology meta-analysis found that BICR-assessed and investigator-assessed PFS were broadly comparable across randomized trials in HR-positive/HER2-negative metastatic breast cancer.
The overall discrepancy index was 1.02, showing no statistically significant difference between the two approaches.
A small difference favoring longer BICR-assessed PFS was seen in control arms, but the absolute difference was less than half a month.
The message is practical: investigator-assessed PFS may be a reliable primary endpoint in many metastatic breast cancer trials, while BICR should be used selectively in settings where independent review is most likely to improve confidence, reduce bias, or support regulatory interpretation.
References
- Ravani LV, Bagheri Z, Kalinsky K, et al. Progression-Free Survival in Metastatic Breast Cancer by Local Investigators vs Blinded Independent Central Review: A Systematic Review and Meta-Analysis. JAMA Oncology. Published online July 16, 2026. doi:10.1001/jamaoncol.2026.1571.
- Dodd LE, Korn EL, Freidlin B, et al. Blinded independent central review of progression-free survival in phase III clinical trials: important design element or unnecessary expense? Journal of Clinical Oncology. 2008;26:3791-3796.
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372.
{kind=link}
{kind=link}
{kind=link}